Paratesticular sarcoma of the spermatic cord: A rare case of dedifferentiated leiomyosarcoma
Resul Çi̇çek, İbrahim Topçu, Bulut Dural, Serhat Toprak, Ömer Faruk Yıldırım, Yasin Karaçor

TL;DR
This paper reports a rare case of paratesticular sarcoma diagnosed as dedifferentiated liposarcoma, emphasizing the need for thorough evaluation and complete surgical removal.
Contribution
The novelty lies in presenting a rare case with detailed histopathological and immunohistochemical findings for accurate diagnosis.
Findings
The tumor was diagnosed as dedifferentiated liposarcoma after comprehensive evaluation.
Radical inguinal orchiectomy was performed for treatment.
Comprehensive pathological evaluation is crucial for accurate diagnosis and management.
Abstract
Paratesticular sarcomas are extremely rare tumors characterized by aggressive biological behavior and a significant risk of recurrence and metastasis. We present a rare case of paratesticular sarcoma ultimately diagnosed as dedifferentiated liposarcoma following comprehensive histopathological and immunohistochemical evaluation. The patient presented with complaints of scrotal edema and discomfort, and radical inguinal orchiectomy was performed. The definitive diagnosis was established through comprehensive histological and immunohistochemical evaluation and was defined as dedifferentiated liposarcoma. This report emphasizes the critical importance of comprehensive pathological evaluation and highlights total surgical excision as the primary approach in the treatment of paratesticular sarcomas due to their rarity and complex diagnosis
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
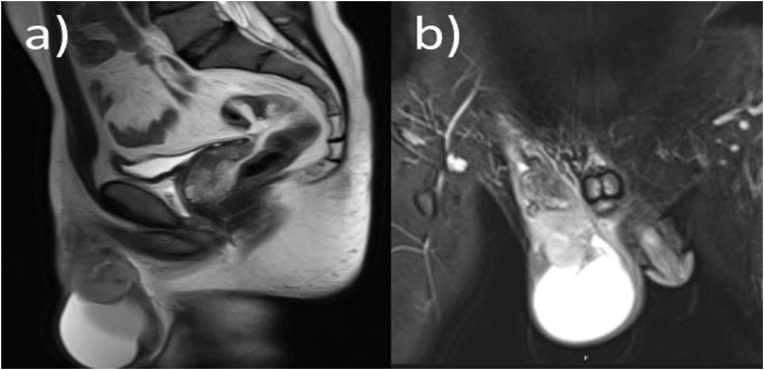 Figure 1
Figure 1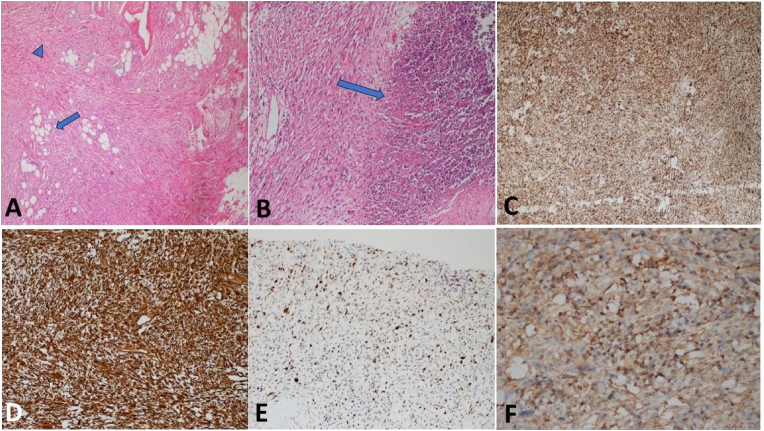 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTesticular diseases and treatments · Sarcoma Diagnosis and Treatment · Urologic and reproductive health conditions
Introduction
1
Paratesticular sarcomas constitute roughly 2% of all male genitourinary cancers, predominantly originating from the spermatic cord.1 These tumors display a wide histological range and may clinically resemble benign disorders such lipomas, epididymal cysts, or inguinal hernias, sometimes resulting in delayed or inadvertent diagnosis.2^,^3
Leiomyosarcoma (LMS) is a rare malignant soft-tissue neoplasm derived from smooth muscle cells and is noted as the second most prevalent malignant paratesticular tumor following liposarcoma.4^,^5 It primarily impacts males in their fifties and sixties, usually manifesting as a gradually increasing, painless scrotal lump.1 As the tumor advances, symptoms include discomfort, compressive effects, and signs of local invasion may manifest. Dedifferentiated liposarcoma represents a high-grade subtype with aggressive behavior and a significant risk of local recurrence, particularly when arising from the spermatic cord. Accurate distinction from leiomyosarcoma is critical, as morphological overlap may lead to diagnostic misclassification without appropriate molecular or immunohistochemical confirmation6.
Complete surgical excision is the fundamental treatment for spermatic cord leiomyosarcoma and other malignant mesenchymal tumors. Achieving negative surgical margins may be difficult due to anatomical limitations, hence Elevating the risk of local recurrence.5^,^7
This case report details the clinical course, diagnostic methodology, and surgical outcomes of a patient diagnosed with paratesticular sarcoma reported as undifferentiated leiomyosarcoma. By synthesizing this case with previously documented data, we aim to increase clinical awareness and provide insights into the management and follow-up methods for these rare but aggressive malignancies.
Case
2
A 61-year-old male patient exhibited scrotal soreness and a progressively increasing lump that had persisted for roughly 6 months. The physical examination disclosed a solid, non-painful paratesticular tumor. Imaging studies revealed a solid lesion situated in the spermatic cord, measuring approximately 7.2 × 5.0 cm (Fig. 1A–B). Thoracoabdominal computed CT revealed no indications of distant metastatic illness.Fig. 1. Pelvic magnetic resonance imaging demonstrating a well-defined, heterogeneous solid mass arising from the spermatic cord in the paratesticular region. The lesion shows predominantly intermediate signal intensity on T1-weighted images and heterogeneous high signal intensity on T2-weighted images, with displacement of adjacent scrotal structures and no evidence of direct testicular invasion.Fig. 1
The patient underwent radical inguinal orchiectomy as the definitive surgical procedure. Histopathological evaluation demonstrated a densely cellular tumor composed of spindle-shaped cells arranged in intersecting fascicles, exhibiting fibrosarcoma-like architecture with scattered lipoblasts and areas of necrosis (Fig. 2A and B). Immunohistochemical analysisFig. 2Tumoral proliferation composed of fibrosarcoma-like spindle cells arranged in intersecting fascicles (arrowhead), with scattered lipoblasts (arrow) (A, H&E × 40), areas of necrosis (arrow) (B, H&E × 100), and immunohistochemical positivity for p16 (C, × 100), vimentin (D, × 100), and nuclear MDM2 expression (E, × 100).Fig. 2
showed strong positivity for p16 (Fig. 2C), vimentin (Fig. 2D), and nuclear MDM2 expression (Fig. 2E–F), confirming the diagnosis of dedifferentiated liposarcoma. Although CDK4, smooth muscle actin, and desmin are well-established diagnostic markers for liposarcoma and leiomyosarcoma respectively, these markers were not contributory in the present case and therefore were not emphasized in the diagnostic interpretation.
Despite negative surgical margins for tumor involvement, the lesion's closeness to adjacent anatomical structures constrained the attainable margin width. The postoperative period was uneventful. Due to the tumor subtype's aggressive biological behavior and significant recurrence potential, the patient was enrolled in a systematic surveillance program. No local recurrence or distant metastases were observed during a 9-month follow-up period. The patient was enrolled in a structured surveillance program consisting of regular physical examinations and cross-sectional imaging.
Discussion
3
Paratesticular sarcomas are uncommon malignant mesenchymal tumors originating from tissues including the spermatic cord, epididymis, and testicular tunics, representing roughly 1–2% of all male genitourinary malignancies.4 Owing to their gradual development and generally asymptomatic nature, these tumors are frequently misidentified as benign paratesticular diseases, such as lipomas, hernias, or epididymal cysts, potentially leading to delayed diagnosis and inadequate initial treatment.2
The biological behavior of paratesticular sarcomas is predominantly influenced by histological subtype and tumor grade. High-grade tumors, including dedifferentiated liposarcoma and leiomyosarcoma, have aggressive clinical trajectories, marked by elevated incidences of local recurrence and distant metastasis relative to low-grade mesenchymal tumors.8 Extensive institutional studies have repeatedly shown that histology, grade, tumor size, and margin status are the primary prognostic factors affecting oncological outcomes.7
The precise diagnosis of paratesticular sarcomas continues to be difficult despite advancements in imaging techniques. Ultrasonography and magnetic resonance imaging are effective for determining lesion location and size; however, these modalities lack adequate specificity to consistently distinguish between benign and malignant mesenchymal tumors or to anticipate histological subtype. Thus, a conclusive diagnosis depends on histological analysis post-surgical excision, highlighting the restricted utility of imaging as an independent diagnostic method.
Immunohistochemistry is essential for the categorization of paratesticular sarcomas and for differentiating them from histological mimickers. Dedifferentiated liposarcomas are distinguished by the amplification and overexpression of MDM2 and CDK4, which function as very sensitive and specific diagnostic indicators. Markers such as p16 and vimentin, while not specific, may provide supportive evidence in high-grade mesenchymal tumors and should be interpreted in conjunction with morphological features and lineage-specific markers(2). Leiomyosarcomas generally have positivity for smooth muscle markers, including smooth muscle actin and desmin6, 9.
Nonetheless, immunohistochemistry results should invariably be analyzed alongside morphological characteristics, as no singular marker is wholly unique, especially in high-grade or poorly differentiated neoplasms.
Surgical excision is the fundamental treatment for paratesticular sarcomas. Radical inguinal orchiectomy with high closure of the spermatic cord is recognized as the preferred surgical technique, facilitating en bloc resection and reducing the likelihood of tumor seeding.1
Numerous high-impact studies have highlighted that insufficient initial surgery, such as scrotal violation or incomplete excision, correlates with markedly elevated rates of local recurrence.4^,^7 Achieving extensive negative margins may be technically difficult due to the proximity of the tumor to critical inguinal structures.
The function of adjuvant therapy in paratesticular sarcomas is still contentious. Retrospective results indicate that adjuvant radiation may diminish local recurrence in high-grade tumors or instances with narrow or positive surgical margins, however a definitive survival advantage has not been consistently established7 Chemotherapy is often designated for metastatic or unresectable conditions, with limited and inconsistent efficacy in genitourinary soft tissue sarcomas.3
Due to the significant risk of local recurrence and delayed metastasis—especially in dedifferentiated liposarcoma and high-grade leiomyosarcoma—prolonged follow-up is necessary. Previous series have reported that local recurrence of dedifferentiated liposarcoma most commonly occurs within 24–36 months following surgery, although late recurrences beyond five years have also been described. Prior research has indicated local recurrence rates of 40–50% for dedifferentiated liposarcomas, with the lungs being the predominant location of distant metastasis.6^,^10 5Consequently, prolonged monitoring with regular cross-sectional imaging is highly advised, even for patients with initially positive surgical results.
In conclusion, paratesticular sarcomas are uncommon yet potentially malignant neoplasms
that necessitate a heightened level of suspicion for prompt identification. Complete surgical excision is the principal therapeutic approach, whereas histological and immunohistochemical evaluations are essential for precise tumor categorization. Due of the potential for late recurrence and metastasis, systematic long-term follow-up is essential to enhance oncological outcomes. Thoroughly documented case reports and short series are crucial in enhancing diagnostic and therapeutic approaches for these rare cancers.
CRediT authorship contribution statement
Resul Çi̇çek: Writing – review & editing. İbrahim Topçu: Writing – original draft. Bulut Dural: Data curation. Serhat Toprak: Data curation. Ömer Faruk Yıldırım: Data curation. Yasin Karaçor: Data curation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ahmed F.Aslam A.Tanveer Y.Jaffry S.Leiomyosarcoma of the spermatic cord: a rare paratesticular neoplasm case report World J Surg Oncol 2012022943533733410.1186/s 12957-022-02539-9PMC 8957147 · doi ↗ · pubmed ↗
- 2ÜnlüY.Huq G.E.Özyalvaçli G.Paratesticular sarcomas: a report of seven cases Oncol Lett 9120153083122543598110.3892/ol.2014.2629 PMC 4246635 · doi ↗ · pubmed ↗
- 3Keenan R.A.Nic An Riogh A.U.Stroiescu A.Paratesticular sarcomas: a case series and literature review Therapeutic advances in urology 112019175628721881802910.1177/1756287218818029 PMC 632901830671140 · doi ↗ · pubmed ↗
- 4Dotan Z.A.Tal R.Golijanin D.Adult genitourinary sarcoma: the 25-year Memorial Sloan-Kettering experience J Urol 17652006203320391707024710.1016/j.juro.2006.07.021 · doi ↗ · pubmed ↗
- 5Reback T.Pang K.H.Haider A.Paratesticular sarcoma: analysis of oncological outcomes and prognostic factors Clin Genitourin Cancer 202510233110.1016/j.clgc.2025.10233140221301 · doi ↗ · pubmed ↗
- 6Crago A.M.Singer S.Clinical and molecular approaches to well differentiated and dedifferentiated liposarcoma Curr Opin Oncol 23420113733782155212410.1097/CCO.0b 013e 32834796 e 6PMC 3253354 · doi ↗ · pubmed ↗
- 7Ballo M.T.Zagars G.K.Pisters P.W.Feig B.W.Patel S.R.Acv Eschenbach Spermatic cord sarcoma: outcome, patterns of failure and management J Urol 16642001130613101154706310.1016/s 0022-5347(05)65758-8 · doi ↗ · pubmed ↗
- 8Galosi A.B.Scarpelli M.Mazzucchelli R.Adult primary paratesticular mesenchymal tumors with emphasis on a case presentation and discussion of spermatic cord leiomyosarcoma Diagn Pathol 912014902488550010.1186/1746-1596-9-90PMC 4039061 · doi ↗ · pubmed ↗