HepAssis2® bioartificial liver system in treating acute‐on‐chronic liver failure patients: Findings from a phase 1 randomised, open‐label clinical trial
Zibiao Zhong, Wenjin Liang, Yong'an Dai, Chengbiao Xue, Dawei Zhou, Zhigao Xu, Ling Li, Li Pan, Chongxiang He, Xin Zhou, Wei Zhou, Lihua Zhou, Zhongzhong Liu, Zhiping Xia, Xiaoli Fan, Guizhu Peng, Yanfeng Wang, Ping Zhou, Shaojun Ye, Qifa Ye

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
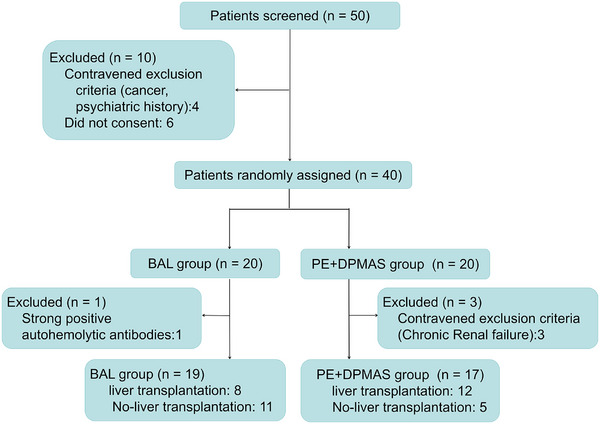 FIGURE 1
FIGURE 1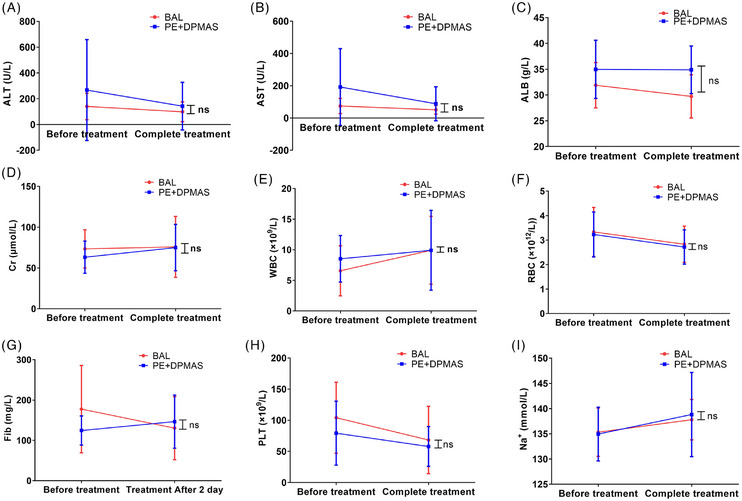 FIGURE 2
FIGURE 2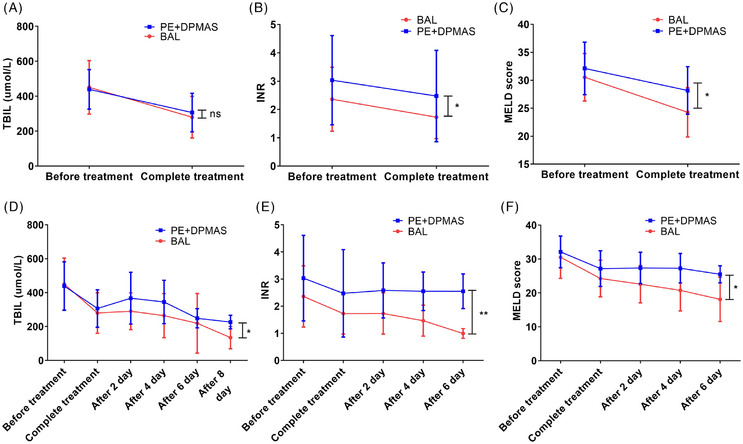 FIGURE 3
FIGURE 3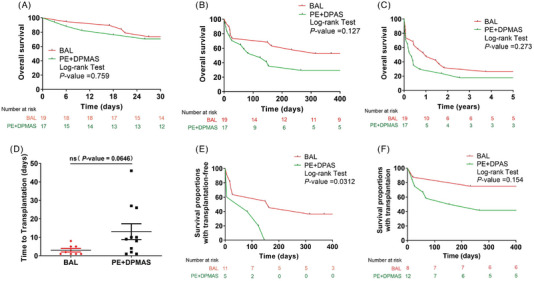 FIGURE 4
FIGURE 4- —Key Project of Health Commission of Hubei Province
- —Chutian Talents Program in Science and Technology Innovation Team
- —National Natural Science Foundation of China10.13039/501100001809
- —Wuhan Science and Technology Project10.13039/501100018583
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver physiology and pathology · Liver Disease and Transplantation · Organ Transplantation Techniques and Outcomes
1
Dear Editor,
Acute‐on‐chronic liver failure (ACLF) carries a grave prognosis of clinical syndrome, with its 28‐day mortality reported to be 50%.1 In China, a high‐endemic region for hepatitis B virus (HBV), over 80% of ACLF cases are HBV related.2 Because of the persistent shortage of donor livers and limited access to timely transplantation, the effective bridging therapies to sustain patients and improve survival are urgently needed.3 Bioartificial liver (BAL) systems represent a promising solution by providing both detoxification and synthetic hepatic functions.4, 5 Our research constitutes the first phase 1 randomised, open‐label trial for patients with HBV‐ACLF who were treated with the HepAssis2^®^ BAL system. The system's design (Figure S1) centres on an optimised bioreactor containing the immortalised L‐02 human foetal hepatocyte line.6
Ethical approval for this phase 1 trial was granted by the Medical Ethics Committee of Zhongnan Hospital of Wuhan University (no. 2016003). This trial was also formally registered at the Chinese Clinical Trial Registry (ChiCTR2300075781), 40 patients diagnosed with HBV‐ACLF were recruited from Zhongnan Hospital of Wuhan University over 2 years (January 2018 to December 2019). The main inclusion criteria are as followed: (1) informed consent from patient/legal guardian; (2) the diagnosis of ACLF was applied according to the following criteria: serum total bilirubin >171 µmol/L (or daily increase ≥17.1 µmol/L) plus prothrombin activity ≤40%; and (3) none of end‐stage complications (irreversible respiratory failure, cerebral herniation, sepsis or other severe infections). Using a randomisation schedule generated with SPSS 17.0, the 40 subjects were randomly allocated to two groups in a sequential order of enrollment. One group (N = 17 following exclusions) was treated with the combination of plasma exchange and the dual plasma molecular adsorption system (PE + DPMAS) according to the clinical guidelines for ACLF, and the other received the HepAssis2^®^ BAL system therapy (N = 19 after exclusions) (Figure 1), alongside standard medical care. The primary outcome is the safety assessment, while the secondary outcomes are the model for end‐stage liver disease (MELD) score, total bilirubin level, coagulation function and annual survival rate.
Flow chart of study selection.
Our key findings indicated that the BAL group received 1.5 ± .7 plasma‐free sessions, whereas the PE + DPMAS group received 1.4 ± .6 sessions, which require 2547.1 ± 451.5 mL of plasma per session (Table S1). Only three patients experienced chills during the initiation of BAL treatment, which can be resolved promptly with intravenous methylprednisolone. In addition, no other significant adverse events were observed, such as severe allergic reactions or embolic phenomena. Furthermore, we conducted a comparative analysis of laboratory indicators such as renal function, electrolytes and haematological parameters before and after treatment. The results showed no significant differences. It confirmed that the BAL treatment was safe (Figure 2).
Comparative analysis of liver and kidney functions, blood cell counts, electrolytes and coagulation function indicators before and after treatment in two groups.
Compared to the control group, the BAL group demonstrated a superior efficacy in reducing MELD scores post‐treatment (p <.05), which implies a more substantial alleviation of hepatic disease severity. Additionally, reductions in total bilirubin and international normalised ratio (INR) during the first week post‐treatment were also more marked in the BAL group (Figure 3). We further applied the Kaplan‒Meier method for long‐term survival analysis and performed intergroup comparisons using the log‐rank test with Bonferroni correction. We have found that there are no statistically significant survival differences between the two groups at 28 days, 1 year or 5 years. Sequentially, a substantial number of patients underwent liver transplantation as a bridging procedure in two groups (12/17 in the control group vs. 8/19 in the BAL group). Further subgroup analysis revealed that among patients who did not undergo liver transplantation, the 1‐year survival rate was significantly higher in the BAL group compared to the PE + DPMAS group (p = .0312). In contrast, among the subgroup of patients who received liver transplantation, there was no statistically significant difference (p = .154) (Figure 4). These findings suggest that BAL therapy may confer a distinct survival advantage for ACLF patients who are not candidates for or do not receive liver transplantation.
Comparative analysis of total bilirubin (TBIL), international normalised ratio (INR) and model for end‐stage liver disease (MELD) score before and after a single treatment (A‒C) and during the full‐cycle treatment (D‒F) in two groups.
Comparison of the 28 days, 1 year and 5 years overall survival rates of patients of two groups (A‒C), the waiting time (D) for bridging liver transplantation, and with transplantation‐free (E) or with transplantation (F) in two groups.
In conclusion, this first‐in‐human clinical trial of BAL therapy for ACLF patients confirmed its comparable safety to the conventional PE + DPMAS regimen and highlighted its clinical advantage in improving the 1‐year overall survival rate for patients who did not undergo liver transplantation. These findings underscore its potential as a key bridging therapy for ACLF patients. Additionally, the plasma‐free session of BAL therapy further enhanced its safety profile. However, the main limitations of this trial included its single‐centre design and relatively limited number of participants. Furthermore, differences were observed in baseline prothrombin time, INR and alanine aminotransferase. These differences are likely attributable to substantial individual variability and the limited sample size; this can also be seen from the standard deviation data. Nevertheless, there was no significant difference in the key baseline assessment indicator of the MELD score. Furthermore, after correcting the laboratory parameters, our findings remained unchanged. With advances in multidisciplinary integration, BAL therapy stands at the forefront of liver regenerative medicine.7, 8 These advances provide a more effective and feasible alternative for the treatment of liver failure.9, 10 Nevertheless, larger‐scale, multicentre trials are warranted in the future to confirm these promising findings and further elucidate the role of BAL therapy.
AUTHOR CONTRIBUTIONS
Yanfeng Wang, Ping Zhou, Shaojun Ye and Qifa Ye were responsible for the conception and supervision of the study. Zibiao Zhong and Wenjin Liang performed most of the experiments. Yong'an Dai, Chengbiao Xue, Dawei Zhou, Wei Zhou, Lihua Zhou, Zhongzhong Liu, Zhigao Xu, Xiaoli Fan, Guizhu Peng, Ling Li, Li Pan, Chongxiang He and Xin Zhou performed patient recruitment and clinical treatment. Zibiao Zhong and Wenjin Liang analysed the data and wrote the paper with suggestions from other authors.
CONFLICT OF INTEREST STATEMENT
The authors declare they have no conflicts of interest.
ETHICS STATEMENT
The studies involving human participants were reviewed and approved by the Ethics Committee of Zhongnan Hospital of Wuhan University (no. 2016003). All of the participants provided their written informed consent to participate in this study.
Supporting information
FIGURE S1. Structural model diagram of HepAssis2^®^ bioartificial liver system.
TABLE S1. Characteristics of patients with Bioartificial liver (BAL) or combination of plasma exchange and the dual plasma molecular adsorption system (PE + DPMAS) group.
Supporting Information
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Moreau R , Jalan R , Gines P , et al. Acute‐on‐chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology. 2013;144(7):1426‐1437, 1437.e 1‐9. doi:10.1053/j.gastro.2013.02.042 23474284 · doi ↗ · pubmed ↗
- 2Wu T , Li J , Shao L , et al. Development of diagnostic criteria and a prognostic score for hepatitis B virus‐related acute‐on‐chronic liver failure. Gut. 2018;67(12):2181‐2191. doi:10.1136/gutjnl-2017-314641 28928275 · doi ↗ · pubmed ↗
- 3Choudhury A , Kulkarni AV , Arora V , et al. Acute‐on‐chronic liver failure (ACLF): the ‘Kyoto Consensus’‐steps from Asia. Hepatol Int. 2025;19(1):1‐69. doi:10.1007/s 12072-024-10773-4 PMC 1184676939961976 · doi ↗ · pubmed ↗
- 4Feng L , Wang Y , Fu Y , et al. Stem cell‐based strategies: the future direction of bioartificial liver development. Stem Cell Rev Rep. 2024;20(3):601‐616. doi:10.1007/s 12015-023-10672-5 38170319 · doi ↗ · pubmed ↗
- 5Hu X , Yang T , Li C , et al. Human fetal hepatocyte line, L‐02, exhibits good liver function in vitro and in an acute liver failure model. Transplant Proc. 2013;45(2):695‐700. doi:10.1016/j.transproceed.2012.09.121 23498809 · doi ↗ · pubmed ↗
- 6Li P , Liang X , Xu S , et al. A non‐bioartificial liver support system combined with transplantation in HBV‐related acute‐on‐chronic liver failure. Sci Rep. 2021;11(1):2975. doi:10.1038/s 41598-021-82719-x 33536531 PMC 7859234 · doi ↗ · pubmed ↗
- 7Xue WS , Zhang HJ , Ke JJ , et al. A bioartificial transgenic porcine whole liver expressing human proteins alleviates acute liver failure in pigs. Hepatobiliary Pancreat Dis Int. 2023;22(3):270‐281. doi:10.1016/j.hbpd.2022.06.012 35835690 · doi ↗ · pubmed ↗
- 8Wu S , Yue P , Ma Y , et al. Hemoperfusion adsorbents for removal of common toxins in liver and kidney failure: recent progress, challenges, and prospects. Adv Mater. 2025;37:e 2305152. doi:10.1002/adma.202305152 37566803 · doi ↗ · pubmed ↗