Multiple Granular Cell Tumors of the New Born: A Case Report and Literature Review
Fawzia M. Butt, Shamim A. Butt, M. L. Chindia

TL;DR
A newborn had multiple benign oral tumors that were surgically removed, leading to a full recovery.
Contribution
This case report adds to the limited literature on congenital granular cell epulis in newborns.
Findings
The tumors were confined intra-orally and did not spread.
Surgical excision led to smooth recovery and excellent prognosis.
The case highlights the rarity and clinical management of this condition in newborns.
Abstract
Congenital granular cell epulis, a rare benign tumor, predominant in females present on the maxillary alveolar ridge. A newborn exhibited multiple oral tumors, interfering with breastfeeding. CT scan showed its confinement intra‐orally. The tumors were excised and surgical site closed primarily. Recovery was smooth with excellent prognosis. Preoperative clinical photo highlighting the intra oral maxillary masses.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
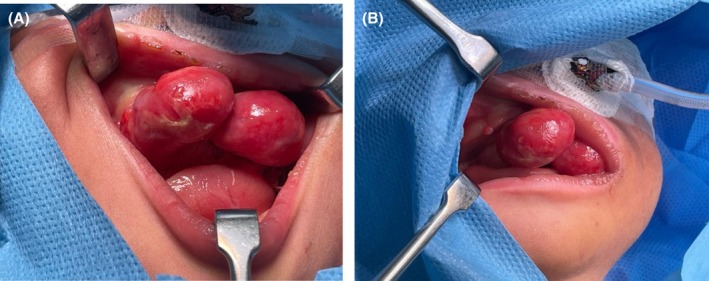 FIGURE 1
FIGURE 1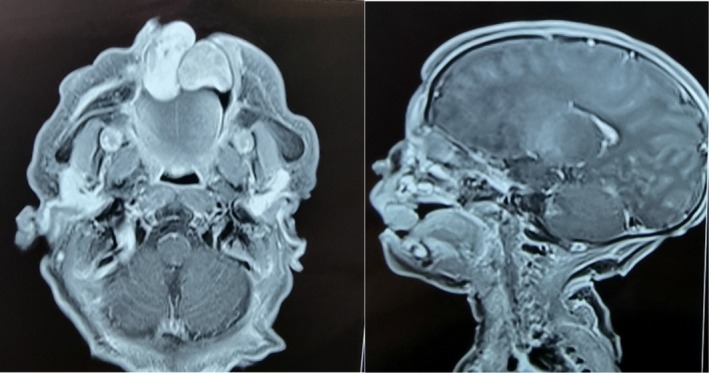 FIGURE 2
FIGURE 2 FIGURE 3
FIGURE 3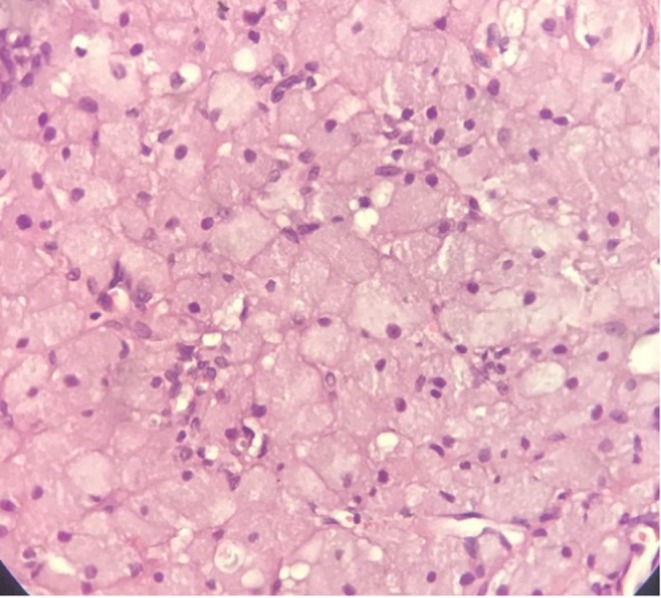 FIGURE 4
FIGURE 4 FIGURE 5
FIGURE 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTumors and Oncological Cases · Teratomas and Epidermoid Cysts · Chromatin Remodeling and Cancer
Introduction
1
In 1871, Dr. Franz Ernst Christian Neumann, a German pathologist, was credited for the description of an uncommon and unusual neonatal lesion termed the congenital granular cell epulis (CGCE). In Greek, Epulis means “swelling on the gingiva” [1]. Alternative nomenclature used for this lesion may include any of the following: Neumann tumor, granular cell myoblastoma, gingival granular cell tumor (GCT), granular cell fibroblastoma, Abrikosov tumor, granular cell lesion, and congenital epulis. However, the World Health Organization recommends the distinctive term “congenital granular cell epulis” [1, 2]. Approximately 250 cases of this benign lesion have been documented to date, with a female to male ratio of 10:1 [3, 4]. CGCE is a rare lesion and may be overlooked in the differential diagnosis of intraoral tumors [5].
Often, CGCE is present in the neonate's oral cavity as a soft lesion primarily in the alveolar ridge. It is a benign tumor with multiple lesions comprising nearly 10% of cases [3]. Though its histogenesis is unknown and debatable, it has been suggested that CGCE initiation emanates from undifferentiated mesenchymal, epithelial, nerve‐related cells, fibroblasts, pericytes, smooth muscle, or it could be neuroectodermal in origin [6]. Previous occasional cases of minor midface hypoplasia, an absent or a hypoplastic tooth have been reported. However, no cases are known to be associated with dental abnormalities or congenital anomalies [5]. Diagnosis is primarily clinical, making the differential diagnosis broad; hence, the importance of imaging cannot be overemphasized [4]. Tumor detection prenatally is possible via magnetic resonance imaging (MRI) or ultrasound (US) since CGCE manifestation occurs during the third trimester of pregnancy [3]. It is visible as a clear hypoechoic bulging oral mass accompanied by branched vascularization, with rapid growth during the third trimester of pregnancy and immediately ceasing at birth [2]. We present a case of CGCE noted immediately after birth.
Case History and Examination
2
An Oral and Maxillofacial Surgeon was consulted one hour after the delivery of a female neonate weighing 3400 g via caesarean section, to assess multiple pink, pedunculated swellings protruding from the patient's oral cavity (Figure 1). The general pediatric assessment indicated impending challenges with breastfeeding and respiration. Notably, there was evidence of lip incompetence, as well as dryness and crusting. Intravenous support had been instituted for nutrition and hydration. Intraoral inspection revealed two large pedunculated masses {2.5 cm largest diameter on the anterior maxillary alveolar mucosa and three smaller ones on the mandibular alveolar ridge (5–8 mm in diameter)}. The mucosa was well vascularized and pink in color.
(A, B) Preoperative photo highlighting the exuberant pedunculate intra‐oral maxillary masses.
Methods (Investigations, Differential Diagnosis and Treatment)
3
An MRI of the head and neck was requested to rule out the presence of feeder vessels close to the larger masses. The radiology scan reported two pedunculated masses iso dense on T1W1 and mixed signal intensity on T2W1 with post contrast enhancement were seen that appeared to arise from the alveolar aspect of the palate without erosion or cleft of the palate. The left mass was reported to be round and measured 13 mm in diameter, and the right measured 26mmx10mmx10mm{anteroposterior (AP)X transverse (TV)X craniocaudal (CC)}. The mass abutted the tongue with inferior and with slight posterior displacement. The airway was otherwise intact. All other structures including the neck and visualized vasculature were unremarkable. A differential diagnosis of a granular cell epulis, melanotic neuroectodermal tumor of infancy, infantile myofibroma, and teratoma was made.
The radiological diagnosis was in keeping with the clinical differential diagnosis of a granular cell epulis (Figure 2). Theater was promptly scheduled because of feeding difficulties. Under general anesthesia using nasotracheal intubation, 0.5 mL of 2% lignocaine with adrenaline (1:80,000) was infiltrated around the tumor bases. The tumor was excised via an elliptical incision, and the margins were primarily closed with 6–0 vicryl sutures. The specimens were submitted for histopathology and immunohistochemistry (IHC) (Figure 3). The patient breastfed a few hours later and had an uneventful recovery. She was discharged on the third postoperative day with an excellent prognosis.
MRI showing two pedunculated masses which are iso dense on T1W1 and mixed signal intensity on T2W1 with post contrast enhancement seen that appear to arise from the alveolar aspect of the palate without erosion or cleft of the palate.
Intra operative photo of the five excised masses.
Results
4
The histopathology report showed sections of a nodular tumor composed of sheets and nests of thin fibrous stroma. The tumor cells were rounded to polygonal cells with distinct cellular borders. There was abundant eosinophilic, granular cytoplasm, and smaller vesicular nuclei with no mitosis and necrosis. These features are consistent with those of CGCE (Figure 4.) The IHC report showed tumors cells were positive for Vimentin, neuron‐specific enolase (NSE), 8% positivity K167 for and negative for Desmin, Smooth Muscle Actin (SMA), (cytokeratin) CK, CD34, CD68, Inhibin, S100 and Calretinin.
Hematoxylin and Eosin stain tissue (MagnificationX40) showing sections of a nodular tumor composed of sheets and nests of thin fibrous stroma. The tumor cells are rounded to polygonal cells with distinct cellular borders. There is abundant eosinophilic, granular cytoplasm, and smaller vesicular nuclei showing hardly any mitosis nor necrosis.
Discussion
5
The occurrence of multifocal lesions within black neonates is found to be rare [7]. The last documented case in Kenya to our knowledge was reported in 1994 [8]. Owing to this rare occurrence, we report the third Kenyan case of a black female neonate who was postnatally diagnosed with CGCE [3]. CGCE tumors are typically soft, have a smooth surface, and are well‐defined. They may be pedunculated or sessile, multilobed, and display pink or red coloring. Their size can vary from just a few millimeters up to 9 cm in diameter. They are predominantly found more in the maxillary than the mandibular alveolus. Clinically, the lesion firmly attaches like a polyploid nodule to the labial or palatal gingiva. It can be erythematous or ulcerated, with the bone and teeth not involved [1, 2, 3, 5, 8]. Diagnosis can be based on clinical parameters; however, histopathological and histochemical criteria are equally fundamental in the determination of tumor diagnosis and management. The histological presentation was not of an atypical nature. The following IHC markers: S‐100, laminin, CD34, CD68, Nerve growth factor receptor (NGFR)/p75, inhibin‐alpha, chromogranin, desmin, keratins, SMA, CD31, and GLUT‐1 are absent during testing and those that test positive are Vimentin and NSE. As for our patient, the IHC tests showed the tumor to be negative for Desmin, SMA, CK, CD34, CD68, Inhibin, S100, Calretinin, while positive for Vimentin and NSE, identical to the trend reported [9, 10]. The proliferation index of the tumor disclosed was 8% showing Ki‐67 positivity which is similar to the range documented in some studies, that is, from 11.1%–16.7% and 15.1%–33.3% respectively [11, 12, 13].
The features outlined were typical of the tumor's description in the literature. The presence of multiple tumors, compounded by their size/s, may have led to the interference in the newborn's respiration and nutrition. Hence the need for urgent surgical intervention. The multidisciplinary team involved a gynecologist, neonatologist, maxillofacial surgeon, and anesthesiologist. The recommended treatment of choice is surgical excision, which usually has excellent prognosis [14]. Cases of recurrences have not been documented even when incomplete margins are excised, any malignant variation, or any futuristic disruption in teeth, nor gingiva [5]. There has been no association of CGCE with any syndromes or genetic defects; therefore, patients have no risk factors for other deformities or passing it on as an inherited gene [2]. After the meticulous excision we have had a follow up for a year and the patient has no signs recurrence (Figure 5).
Post operative photo after a 6 month period.
Conclusion
6
Neonates born with CGCE need swift action due to the immediate respiratory and nutritional demands of the patient, especially if the tumors are multifocal and large in size. Although a rare and benign lesion, the surgeon must be familiar with the differential diagnosis to proceed with ease and diligence. The treatment plan for CGCE should embrace a multidisciplinary approach including counseling the parents/caregivers, reassuring them of treatment outcomes and life normalcy for the newborn as the review process continues to life normalcy.
Author Contributions
Fawzia M. Butt: conceptualization, data curation. Shamim A. Butt: writing – original draft. M. L. Chindia: writing – review and editing.
Funding
The authors have nothing to report.
Consent
Written informed consent for this case report and associated photographs was obtained from the patient and has been uploaded.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. Aresdahl , B. Lindell , M. Dukic , and A. Thor , “Congenital Granular Cell Epulis—A Case Report,” Oral and Maxillofacial Surgery Cases 1, no. 1 (2015): 8–11, 10.1016/j.omsc.2015.04.001. · doi ↗
- 2R. Conrad and M. C. N. Perez , “Congenital Granular Cell Epulis,” Archives of Pathology & Laboratory Medicine 138, no. 1 (2014): 128–131, 10.5858/arpa.2012-0306-RS.24377822 · doi ↗ · pubmed ↗
- 3E. Torresani , I. Girolami , S. Marletta , A. Eccher , and C. Ghimenton , “Congenital Granular Cell Epulis of Newborn: Importance of Prenatal Diagnosis,” Pathologica 113, no. 4 (2021): 280–284, 10.32074/1591-951X-135.34542544 PMC 8488987 · doi ↗ · pubmed ↗
- 4A. M. Xavier , M. Janardhanan , R. Veeraraghavan , and B. R. Varma , “Congenital Granular Cell Epulis: A Rare Paediatric Tumour of Newborn,” BMJ Case Reports 15, no. 1 (2022): e 244326, 10.1136/bcr-2021-244326.PMC 872845934983807 · doi ↗ · pubmed ↗
- 5M. Jarjanazi , N. Martini , W. Abbas , Y. Molhem , and M. Morjan , “Congenital Granular Cell Mass of the Alveolar Ridge in a Newborn,” Journal of Pediatric Surgery Case Reports 88 (2023): 102517.
- 6Y. Liang , Y.‐S. Yang , and Y. Zhang , “Multiple Congenital Granular Cell Epulis in a Female Newborn: A Case Report,” Journal of Medical Case Reports 8 (2014): 413, 10.1186/1752-1947-8-413.25482350 PMC 4295338 · doi ↗ · pubmed ↗
- 7M. L. Chindia and D. O. Awange , “Congenital Epulis of the Newborn: A Report of Two Cases,” British Dental Journal 176, no. 11 (1994): 426–428, 10.1038/sj.bdj.4808472.8018433 · doi ↗ · pubmed ↗
- 8M. d. C. Navas‐Aparicio , A. Acuña‐Navas , and D. G. Colombari , “Congenital Granular Cell Tumor of the Newborn. A Case Report and Literature Review,” Odovtos ‐ International Journal of Dental Sciences (2024): 135–141, 10.15517/ijds.2022.51475. · doi ↗