Knowledge, attitude, and practice of physicians toward the management of diabetic ketoacidosis
Mabrouk AL-Rasheedi, Baharudin Ibrahim, Khawaja Husnain Haider, Ahmed Amin Ali, Hadzliana Zainal

TL;DR
This study assesses Saudi physicians' knowledge, attitudes, and practices in managing diabetic ketoacidosis, finding significant gaps that suggest a need for better training.
Contribution
The study identifies demographic and professional factors influencing DKA management knowledge and highlights the need for targeted educational programs.
Findings
Only 4.1% of physicians demonstrated good knowledge of DKA management protocols.
Endocrinologists and older physicians showed significantly higher knowledge scores.
Targeted educational interventions are needed to improve DKA management practices.
Abstract
Diabetic ketoacidosis (DKA) is a serious complication of uncontrolled diabetes that results from insufficient insulin, high blood sugar levels, dehydration, and disturbances in acid-base status in the blood. This condition can arise from infections or treatment errors, such as inadequate insulin dosing or missed doses, and affects both type 1 and type 2 diabetes. The study aims to identify gaps in physicians’ knowledge, attitudes, and practices (KAP) regarding the updated Diabetic Ketoacidosis protocol from the Ministry of Health (MoH) to enhance educational programs and improve patient outcomes. This cross-sectional study, conducted between July 2023 and July 2024, involved 242 physicians treating DKA across ten tertiary hospitals in five administrative regions of Saudi Arabia. Interns and physicians with less than one year of experience were excluded. Data were collected using a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
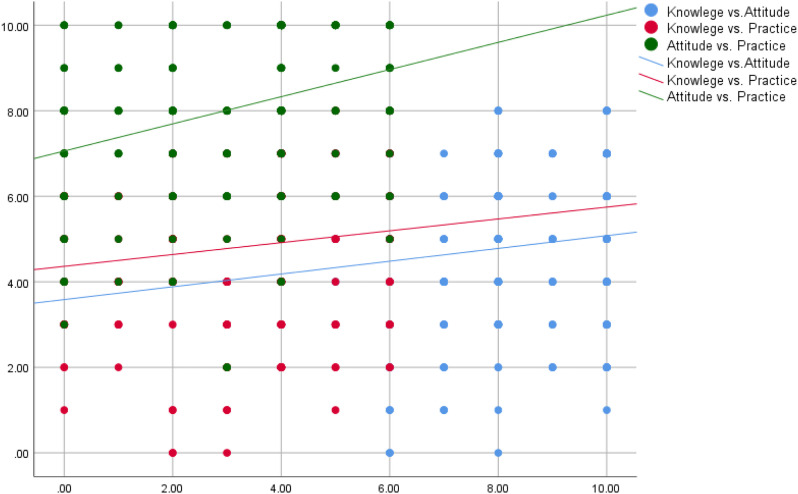 Figure 1
Figure 1| Region | First tertiary hospital | Second tertiary hospital |
|---|---|---|
| Central | King Salman Hospital | King Fahad Hospital |
| Northern | King Khaled Hospital | King Abdulaziz Hospital |
| Southern | King Fahad Hospital | Gazan General Hospital |
| Eastern | Dammam Medical City | King Khaled Hospital |
| Western | Ohud Hospital | King Faisal Medical City |
| Socio-demographic characteristics | Study sample (n =242) | |
|---|---|---|
| No. | % | |
| Sex | ||
| • Male | 124 | 51.2 |
| • Female | 118 | 48.8 |
| Age | ||
| • 20-30 | 87 | 36.0 |
| • 30-40 | 95 | 39.3 |
| • 40 or more | 60 | 24.8 |
| Marital status | ||
| • Single | 86 | 35.5 |
| • Married | 132 | 54.5 |
| • Divorced | 15 | 6.2 |
| • Widow | 9 | 3.7 |
| Nationality | ||
| • Saudi | 148 | 61.2 |
| • Non-Saudi | 94 | 38.8 |
| Region | ||
| • Northern Region | 23 | 9.5 |
| • Southern Region | 30 | 12.4 |
| • Central Region | 77 | 31.8 |
| • Eastern Region | 53 | 21.9 |
| • Western Region | 59 | 24.4 |
| The highest level of education | ||
| • Bachelor | 68 | 28.1 |
| • Diploma | 46 | 19.0 |
| • Master | 25 | 10.3 |
| • Doctorate | 20 | 8.3 |
| • Resident (Board) | 64 | 26.4 |
| • Fellowship | 19 | 7.9 |
| Specialty | ||
| • GPs | 61 | 25.2 |
| • Emergency medicine | 44 | 18.2 |
| • Endocrinology | 24 | 9.9 |
| • Family Medicine | 36 | 14.9 |
| • Intensive care unit | 25 | 10.3 |
| • Internal Medicine | 52 | 21.5 |
| Seniority | ||
| • General practice | 41 | 16.9 |
| • Resident | 78 | 32.2 |
| • Senior | 39 | 16.1 |
| • Specialist | 41 | 16.9 |
| • Consultant | 43 | 17.8 |
| Experience years | ||
| • 1-5 | 99 | 40.9 |
| • 5-10 | 66 | 27.3 |
| • 10-15 | 27 | 11.2 |
| • 15-20 | 27 | 11.2 |
| • >20 | 23 | 9.5 |
| Age (Years) | ||
| Min. – Max. | 21 – 61 | |
| Mean ± SD | 35.5± 8.8 | |
| Parameter | Study sample (n =242) |
|---|---|
| Knowledge (Q1-Q10) | Percentage (%) |
| Poor | 140 (57.9) |
| Fair | 92 (38.0) |
| Good | 10 (4.1) |
| Min. – Max. | 0.0 – 8.0 |
| Mean ± SD. | 4.79 ± 1.85 |
| Attitude (Q11-Q15) | |
| Unfavorable | 21 (8.7) |
| Neutral | 55 (22.7) |
| Favorable | 166 (68.6) |
| Min. – Max. | 2.0 – 10.0 |
| Mean ± SD | 8.03 ± 1.81 |
| Practice (Q16-Q18) | |
| Poor | 117 (48.3) |
| Good | 125 (51.7) |
| Min. – Max. | 0.0 – 6.0 |
| Mean ± SD | 3.05 ± 1.84 |
| Parameters | Knowledge | Attitude | Practice | |||
|---|---|---|---|---|---|---|
| Mean ± SD | p | Mean ± SD | p | Mean ± SD | p | |
| Gender | ||||||
| Male | 4.4 ± 1.88 |
| 8.19 ± 1.87 | 0.169 | 3.39 ± 1.8 |
|
| Female | 5.19 ± 1.74 | 7.86 ± 1.74 | 2.7 ± 1.82 | |||
| Age groups | ||||||
| 20-30 | 4.17 ± 1.83 |
| 7.80 ± 1.67 | 0.053 | 2.84 ± 1.96 | 0.272 |
| 31-40 | 4.63 ± 1.87 | 7.97 ± 1.98 | 3.06 ± 1.84 | |||
| 41 or more | 5.92 ± 1.29 | 8.45 ± 1.70 | 3.35 ± 1.62 | |||
| Marital status | ||||||
| Single | 4.07 ± 1.78 |
| 7.53 ± 1.84 |
| 2.57 ± 1.89 |
|
| Married | 5.05 ± 1.81 | 8.34 ± 1.75 | 3.33 ± 1.75 | |||
| Divorced | 6.20 ± 1.21 | 8.60 ± 1.68 | 3.47 ± 1.85 | |||
| Widow | 5.33 ± 1.73 | 7.22 ± 1.56 | 3.0 ± 2.0 | |||
| Region | ||||||
| Northern region | 4.57 ± 1.67 |
| 7.74 ± 2.34 | 0.775 | 3.22 ± 2.15 | 0.325 |
| Southern region | 4.23 ± 1.96 | 8.37 ± 1.71 | 3.57 ± 1.50 | |||
| Central Region | 3.97 ± 1.77 | 7.92 ± 1.73 | 3.21 ± 1.73 | |||
| Eastern Region | 5.55 ± 1.87 | 8.08 ± 1.91 | 2.68 ± 1.85 | |||
| Western Region | 5.53 ± 1.38 | 8.07 ± 1.68 | 2.86 ± 1.95 | |||
| Years of experience | ||||||
| 0-5 | 4.09 ± 1.89 |
| 7.85 ± 1.69 | 0.232 | 2.83 ± 1.84 | 0.205 |
| 6-10 | 4.86 ± 1.73 | 7.91 ± 2.01 | 2.98 ± 1.97 | |||
| 11-15 | 5.0 ± 1.92 | 8.19 ± 1.86 | 3.37 ± 1.74 | |||
| 16-20 | 6.11 ± 1.28 | 8.56 ± 1.55 | 3.70 ± 1.73 | |||
| >20 | 5.74 ± 1.1 | 8.35 ± 1.97 | 3.09 ± 1.59 | |||
| Nationality | ||||||
| Saudi | 4.39 ± 1.87 |
| 8.05 ± 1.72 | 0.844 | 3.22 ± 1.79 | 0.084 |
| Non-Saudi | 5.41 ± 1.64 | 8.0 ± 1.97 | 2.80 ± 1.90 | |||
| Level of education | ||||||
| Bachelor | 4.04 ± 1.78 |
| 7.74 ± 1.98 | 0.608 | 3.03 ± 1.85 | 0.406 |
| Diploma | 5.41 ± 1.57 | 7.85 ± 1.87 | 2.61 ± 2.20 | |||
| Master | 4.52 ± 1.87 | 8.32 ± 1.65 | 3.12 ± 1.79 | |||
| Doctorate | 5.0 ± 2.18 | 8.15 ± 1.76 | 3.45 ± 1.67 | |||
| Resident (Board) | 4.88 ± 1.77 | 8.27 ± 1.64 | 3.05 ± 1.71 | |||
| Fellowship | 5.74 ± 1.76 | 8.21 ± 1.9 | 3.74 ± 1.33 | |||
| Specialty | ||||||
| GPs | 4.18 ± 1.84 |
| 8.07 ± 1.72 | 0.260 | 3.15 ± 1.88 | 0.063 |
| Emergency medicine | 4.64 ± 1.92 | 7.84 ± 1.78 | 2.68 ± 2.0 | |||
| Endocrinology | 6.25 ± 1.26 | 8.33 ± 2.12 | 3.46 ± 1.82 | |||
| Family medicine | 4.14 ± 1.73 | 7.92 ± 1.78 | 2.94 ± 1.66 | |||
| Intensive care unit | 6.12 ± 1.36 | 8.72 ± 1.37 | 3.88 ± 1.39 | |||
| Internal medicine | 4.75 ± 1.69 | 7.75 ± 1.98 | 2.75 ± 1.88 | |||
| Seniority: | ||||||
| General practice | 4.24 ± 1.87 |
| 7.85 ± 1.73 |
| 3.02 ± 1.94 |
|
| Resident | 4.47 ± 1.92 | 8.04 ± 1.90 | 2.62 ± 1.94 | |||
| Senior | 5.10 ± 1.83 | 7.79 ± 2.17 | 3.54 ± 1.73 | |||
| Specialist | 4.44 ± 1.55 | 7.59 ± 1.50 | 2.54 ± 1.87 | |||
| Consultant | 5.91 ± 1.52 | 8.81 ± 1.47 | 3.93 ± 1.10 | |||
| Parameter | Age | Years of experience | Knowledge | Attitude | Practice | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| r | p | r | p | r | p | r | p | r | p | |
| Knowledge | 0.341 | <0.001* | 0.346 | <0.001* | 0.146 | 0.023* | 0.137 | 0.033* | ||
| Attitude | 0.118 | 0.067 | 0.128 | 0.047* | 0.146 | 0.023* | 0.322 | <0.001* | ||
| Practice | 0.099 | 0.124 | 0.139 | 0.031* | 0.137 | 0.033* | 0.322 | <0.001* | ||
| Predictors | Unstandardized coefficients | Standardized coefficients | t | Individual predictors sig | 95.0% Confidence interval for B | ||
|---|---|---|---|---|---|---|---|
| B | Std. error | Beta | Lower bound | Upper bound | |||
| (Constant) | 2.860 | .825 | 3.467 | .001* | 1.234 | 4.486 | |
| Age (Years) | .023 | .030 | .108 | .743 | .458 | -.037 | .083 |
| Gender “Female” a | .168 | .244 | .045 | .687 | .493 | -.313 | .648 |
| Years of experience | .014 | .038 | .054 | .380 | .705 | -.060 | .088 |
| Nationality “non-Saudi”b | .303 | .281 | .080 | 1.079 | .282 | -.251 | .858 |
| Region c | |||||||
| Eastern Region | .763 | .326 | .171 | 2.338 | .02* | .120 | 1.407 |
| Northern Region | .189 | .410 | .030 | .460 | .646 | -.620 | .998 |
| Western Region | .660 | .327 | .153 | 2.020 | .045* | .016 | 1.304 |
| Southern Region | -.217 | .375 | -.039 | -.581 | .562 | -.956 | .521 |
| Marital status d | |||||||
| Married | .183 | .295 | .049 | .620 | .536 | -.399 | .764 |
| Divorced | .692 | .511 | .090 | 1.354 | .177 | -.315 | 1.700 |
| Widow | -.015 | .616 | -.002 | -.024 | .981 | -1.229 | 1.200 |
| Specialty e | |||||||
| Emergency medicine | .111 | .461 | .023 | .241 | .810 | -.798 | 1.020 |
| Endocrinology | 1.150 | .542 | .186 | 2.123 | .035* | .082 | 2.218 |
| Family Medicine | -.136 | .486 | -.026 | -.280 | .780 | -1.094 | .822 |
| Intensive care unit | 1.037 | .553 | .171 | 1.875 | .062 | -.053 | 2.128 |
| Internal Medicine | .073 | .446 | .016 | .163 | .870 | -.807 | .953 |
| Seniority e | |||||||
| Resident | -.177 | .462 | -.045 | -.383 | .702 | -1.088 | .734 |
| Senior | .385 | .565 | .077 | .682 | .496 | -.728 | 1.499 |
| Specialist | -.133 | .541 | -.027 | -.245 | .807 | -1.200 | .934 |
| Consultant | .660 | .682 | .136 | .967 | .335 | -.685 | 2.005 |
| Level of education f | |||||||
| Diploma | .587 | .394 | .125 | 1.491 | .137 | -.189 | 1.364 |
| Master | -.442 | .457 | -.073 | -.967 | .335 | -1.342 | .458 |
| Doctorate | -.415 | .546 | -.062 | -.760 | .448 | -1.490 | .660 |
| Resident (Board) | -.018 | .364 | -.004 | -.049 | .961 | -.736 | .700 |
| Fellowship | -.426 | .580 | -.062 | -.735 | .463 | -1.569 | .716 |
| Predictors | Unstandardized coefficients | Standardized coefficients | t | Individual predictors sig | 95.0% Confidence interval for B | ||
|---|---|---|---|---|---|---|---|
| B | Std. error | Beta | Lower bound | Upper bound | |||
| (Constant) | 8.195 | .942 | 8.697 |
| 6.338 | 10.053 | |
| Age (Years) | -.035 | .034 | -.168 | -1.020 | .309 | -.101 | .032 |
| Gender “Female” a | -.249 | .271 | -.069 | -.918 | .360 | -.784 | .286 |
| Years of experience | .024 | .042 | .091 | .565 | .573 | -.059 | .106 |
| Nationality “non-Saudi”b | -.163 | .314 | -.044 | -.520 | .604 | -.781 | .455 |
| Region c | |||||||
| • Eastern Region | -.293 | .368 | -.067 | -.797 | .426 | -1.018 | .431 |
| • Northern Region | -.621 | .457 | -.101 | -1.361 | .175 | -1.521 | .278 |
| • Western Region | -.296 | .367 | -.070 | -.808 | .420 | -1.019 | .427 |
| • Southern Region | .218 | .417 | .040 | .523 | .602 | -.604 | 1.039 |
| Marital status d | |||||||
| • Married | .825 | .328 | .227 | 2.513 |
| .178 | 1.472 |
| • Divorced | .532 | .571 | .071 | .931 | .353 | -.594 | 1.657 |
| • Widow | .121 | .685 | .013 | .177 | .860 | -1.229 | 1.472 |
| Specialty e | |||||||
| • Emergency medicine | -.829 | .513 | -.177 | -1.617 | .107 | -1.840 | .181 |
| • Endocrinology | -.570 | .609 | -.094 | -.936 | .350 | -1.769 | .630 |
| • Family Medicine | -.814 | .540 | -.160 | -1.507 | .133 | -1.879 | .251 |
| • Intensive care unit | -.161 | .620 | -.027 | -.259 | .796 | -1.383 | 1.062 |
| • Internal Medicine | -.796 | .496 | -.181 | -1.604 | .110 | -1.774 | .182 |
| Seniority f | |||||||
| • Resident | .536 | .514 | .138 | 1.041 | .299 | -.478 | 1.549 |
| • Senior | .069 | .629 | .014 | .109 | .913 | -1.171 | 1.308 |
| • Specialist | -.144 | .602 | -.030 | -.239 | .811 | -1.330 | 1.043 |
| • Consultant | 1.278 | .760 | .270 | 1.681 | .094 | -.220 | 2.777 |
| Level of education g | |||||||
| • Diploma | .426 | .440 | .092 | .967 | .334 | -.442 | .426 |
| • Master | .924 | .509 | .155 | 1.815 | .071 | -.079 | .924 |
| • Doctorate | -.212 | .608 | -.032 | -.349 | .728 | -1.409 | -.212 |
| • Resident (Board) | .696 | .405 | .170 | 1.717 | .087 | -.103 | .696 |
| • Fellowship | -.267 | .645 | -.040 | -.414 | .679 | -1.539 | -.267 |
| Knowledge | .107 | .076 | .110 | 1.420 | .157 | -.042 | .107 |
| Predictors | Unstandardized coefficients | Standardized coefficients | t | Individual predictors sig | 95.0% Confidence interval for B | ||
|---|---|---|---|---|---|---|---|
| B | Std. error | Beta | Lower bound | Upper bound | |||
| (Constant) | 3.152 | 1.014 | 3.107 |
| 1.152 | 5.151 | |
|
| -.074 | .031 | -.357 | -2.361 |
| -.136 | -.012 |
|
| -.527 | .252 | -.144 | -2.092 |
| -1.023 | -.030 |
|
| .064 | .039 | .242 | 1.651 | .100 | -.012 | .140 |
|
| -.305 | .291 | -.081 | -1.049 | .295 | -.878 | .268 |
| Region c | |||||||
| • Eastern Region | -.863 | .341 | -.194 | -2.531 |
| -1.534 | -.191 |
| • Northern Region | -.157 | .425 | -.025 | -.371 | .711 | -.994 | .679 |
| • Western Region | -.649 | .340 | -.152 | -1.909 | .058 | -1.320 | .021 |
| • Southern Region | .049 | .386 | .009 | .126 | .900 | -.712 | .810 |
| Marital status d | |||||||
| • Married | .658 | .308 | .178 | 2.132 |
| .050 | 1.265 |
| • Divorced | .284 | .530 | .037 | .537 | .592 | -.760 | 1.328 |
| • Widow | 1.253 | .635 | .129 | 1.975 |
| .002 | 2.504 |
| Specialty e | |||||||
| • Emergency medicine | -.880 | .478 | -.185 | -1.843 | .067 | -1.822 | .061 |
| • Endocrinology | .180 | .565 | .029 | .318 | .750 | -.933 | 1.293 |
| • Family Medicine | -.199 | .503 | -.039 | -.396 | .693 | -1.191 | .793 |
| • Intensive care unit | .154 | .574 | .026 | .268 | .789 | -.978 | 1.286 |
| • Internal Medicine | -.563 | .462 | -.126 | -1.217 | .225 | -1.474 | .348 |
| Seniority f | |||||||
| • Resident | -.090 | .477 | -.023 | -.188 | .851 | -1.031 | .852 |
| • Senior | 1.195 | .582 | .239 | 2.052 |
| .047 | 2.342 |
| • Specialist | -.066 | .557 | -.013 | -.118 | .906 | -1.164 | 1.033 |
| • Consultant | 1.312 | .709 | .273 | 1.851 | .066 | -.085 | 2.708 |
| Level of education g | |||||||
| • Diploma | -.128 | .408 | -.027 | -.314 | .754 | -.933 | .677 |
| • Master | -.381 | .475 | -.063 | -.803 | .423 | -1.317 | .554 |
| • Doctorate | -.622 | .563 | -.093 | -1.106 | .270 | -1.731 | .487 |
| • Resident (Board) | -.328 | .378 | -.079 | -.868 | .386 | -1.073 | .417 |
| • Fellowship | -.420 | .598 | -.062 | -.702 | .483 | -1.598 | .759 |
|
| .118 | .070 | .119 | 1.672 | .096 | -.021 | .256 |
|
| .226 | .063 | .223 | 3.579 |
| .102 | .350 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes and associated disorders · Diabetes Management and Research · Chronic Disease Management Strategies
Introduction
a metabolic disorder characterized by impaired glucose oxidation resulting from insufficient insulin (1).
This condition is classified into Type 1 DM (T1DM) and Type 2 DM (T2DM). Diabetic ketoacidosis (DKA) is classically considered a complication of Type 1 Diabetes Mellitus (T1DM) due to absolute insulin deficiency. However, evidence shows that patients with Type 2 Diabetes Mellitus (T2DM) can also develop DKA, particularly under conditions of severe stress, infection, or relative insulin deficiency. In these cases, increased counter-regulatory hormones (glucagon, cortisol, catecholamines) and elevated free fatty acids promote ketogenesis, leading to metabolic acidosis (2).
Clinically, this association is important because physicians should not exclude DKA in patients with T2DM presenting with acute illness, poor glycemic control, or interruption of insulin therapy. Recognition of this link ensures timely diagnosis and management, reducing morbidity and mortality (3).
According to the review of the 10th Edition of the International Diabetes Federation (IDF), Atlas, 537 million adults worldwide have diabetes, projected to reach a colossal 783 million by 2045 (4, 5). This alarming trend, particularly in low- and middle-income countries, is burdening their healthcare systems due to high morbidity and mortality rates (6). The Middle East and North Africa region (MENA) carried the highest prevalence of diabetes in 2019 at 12.2% and is expected to witness a 96% increase in diabetes prevalence by 2045 (7).
The urgency of this situation, akin to a looming storm, cannot be overstated, and healthcare professionals must be aware and prepared for the impending challenges. A cross-sectional study conducted between 2007 and 2009 in Saudi Arabia, involving 18034 individuals over the age of 30, reported a diabetes prevalence of 25.4%, with 10.2% of those cases being previously undiagnosed. This prevalence was significantly higher in urban areas than rural ones (8).
If left unchecked, the situation may worsen due to serious complications associated with uncontrolled DM, with DKA being one of the most common. DKA arises from insufficient insulin, elevated blood sugar levels, dehydration, and increased acidity. Infections or treatment errors, such as inadequate insulin dosing, missed doses, or issues with insulin delivery, are important risk factors (9, 10).
Additional contributing factors include digestive disorders, heart problems, inflammatory diseases, pancreatitis, and substance abuse. Abdominal pain, nausea, vomiting, and fruity odor on the breath are common symptoms among patients (11). Moreover, some patients may also experience the typical signs of DM, such as frequent urination and thirst (12). The mortality rate following a single episode of DKA is reported to be 5.2%, and it rises by 6-fold with five or more admissions of DKA (13).
Physicians should promptly initiate the appropriate management of DKA by conducting a thorough physical examination, obtaining essential metabolic parameters, and establishing a definitive diagnosis, followed by starting an appropriate suitable treatment plan to prevent complications (14, 15).
The aim of this study was to highlight the gaps in physicians’ knowledge, attitudes, and practices (KAP) concerning the recently released updated DKA protocol from the Ministry of Health (MoH). Assessing these factors is vital for enhancing educational programs for physicians and ultimately improving the management of DKA. The need for improved physician education is evident, and this study’s findings can catalyze continuous learning and professional development, ultimately leading to better patient outcomes.
Methods
Study design and participants
A cross-sectional study design was conducted during the period from July 2023 and to July 2024 among physicians treating diabetic patients having DKA in Saudi Arabia. Saudi Arabia. Due to the high prevalence of diabetes, all five administrative health regions (Eastern, Western, Southern, Northern, and Central) were included in the survey. Two tertiary hospitals were selected from each region (Table 1). The study was conducted at the 10 selected institutions representing the five regions of the kingdom. Any physician not dealing with diabetic patients, having less than one year’s experience, and who are currently in their internship year was excluded from the study (16, 17).
The sample size was determined based on an estimated 93,966 physicians across different specialties. Of these, 25% worked in EDs and ICUs, giving a minimum sample size of 80 physicians at a 95% confidence interval, 0.05 alpha error, and 80% power. The sample was raised to 242 physicians.
Data collection tool
The data collection tool was a designed questionnaire evaluated by five experts and validated through a pilot study. It consists of two sections: the first section contains sociodemographic characteristics (age, sex, marital status, level of education, years of experience, specialty, and seniority), while the second section comprises three subsections assessing the studied participants’ KAP. The knowledge subsection had ten questions, scoring 1 for correct answer and 0 for incorrect, with a total score of 10. Participants were classified according to their level of knowledge into good (8-10), fair (5-7) and poor (<5). The attitude subsection comprised five questions with a three-point Likert scale (disagree, neutral, and agree). Each question scored 0 for an unfavorable attitude, 1 for a neutral attitude, or 2 for a favorable attitude, with a total score of 10. Attitude was classified into favorable (8-10), neutral (5-7), and unfavorable (<5). The practice subsection consisted of three questions with a three-point Likert scale (disagree, neutral, and agree). Each question was scored 2 with a total score of 6. poor practice was scored as 0, neutral practice as 1, and good practice as 2. Participants were classified as having poor practice (scoring only 2 out of 6) or good practice if scoring three or more (18).
Ethical considerations
The study was approved by the USM Ethical Committee and by the Ethics Committees of the respective hospitals in Saudi Arabia and followed the international ethical guidelines of the Declaration of Helsinki (19). All participants were informed of the purpose and nature of the study, the privacy and confidentiality of data, and that participation was voluntary. Informed consent was obtained from all participants before the study was initiated. This process involved explaining the study protocol, ensuring anonymity by representing all subjects with codes rather than their names, and allowing participants to freely ask questions about the study with the option to withdraw at will without any consequences.
Statistical analysis
Data was coded and entered using the statistical package for the Social Sciences (SPSS) version 25. According to the distribution of variables using the Kolmogorov-Smirnov test, non-parametric quantitative data was summarized by median as measures of central tendency & range as measures of dispersion. In contrast, parametric quantitative variables were summarized using mean and standard deviation. Frequencies and percentages describe categorical variables. Independent sample t-test and Kruskal-Wallis test were used to detect significant differences between quantitative variables. Pearson correlation was used to assess the correlation between quantitative variables (20). Multiple linear regression analysis was performed to detect the independent contribution of different factors affecting the knowledge, attitude, and practice of Physicians; enter method was selected, and R2 was used to detect the amount of variance in knowledge, attitude, and practice accounted by predictors, included in the model. Significance is considered when p is below 0.05.
Results
Table 2 presents the sociodemographic characteristics of the physicians. Males accounted for 51.2% of the sample, while females represented 48.8%. The mean age was 35.5 ± 8.8 years, ranging from 21 to 61 years. Overall, 61.2% of the participants were Saudi physicians. As regards region (31.8% of physicians from the Central region, followed by (24.4%) from the Western region, and the lowest percentage from the Northern region (9.5%). Regarding educational degrees, Physicians had ‘Bachelor and Board’ constituted 28.1% and 26.4%, respectively; 25.2% of Physicians were GPs, 21.5% were Internists, 18.2% were ER Physicians,14.9% were family medicine Physicians, and the remaining 10.3% and 9.9% were from ICU and Endocrinology departments, respectively.
More than half of physicians (57.9%) had a poor level of knowledge, with a mean score of 4.79 ± 1.85, while 68.6% had a favorable attitude toward MOH guidelines in DKA treatment, and 51.7% had a good practice, with means scores of 8.03 ± 1.81 and 3.05 ± 1.84, respectively, Table 3.
Table 4 shows the factors affecting knowledge, attitude, and practice. Knowledge was significantly higher among females than males (5.19 ± 1.74), p=0.001; physicians aged more than 40 years (5.92 ± 1.29), p<0.001; ever-married physicians, p<0.001; physicians from eastern and western regions (5.55 ± 1.87 and 5.53 ± 1.38, respectively), p<0.001, and physicians with more than 15 years of experience (6.11 ± 1.28 for experience 16–20 and 5.74 ± 1.1 for more than 20 years experience), p<0.001. Non-Saudi physicians and those with a higher education (more than bachelor’s degrees) had a higher knowledge than other physicians (p<0.001). Similarly, endocrinologists and ICU physicians had higher knowledge (6.25 ± 1.26 and 6.12 ± 1.36, respectively), p<0.001, akin to the consultant and senior physicians (5.91 ± 1.52 and 5.1 ± 1.83, respectively), p<0.001.
For attitude, only marital status and seniority had a significant effect on physicians’ attitudes toward MOH guidelines.
Table 5, Knowledge shows a moderate positive correlation with age and years of experience, and weak but significant correlations with attitude and practice.
Attitude has a weak correlation with experience, and a stronger significant correlation with practice.Practice shows a weak correlation with experience, and the strongest correlation with attitude.
Knowledge correlated moderately with age and experience, while attitude showed the strongest correlation with practice (Table 5, Figure 1).
Correlation between KAP among physicians.
Tables 6, 7, 8 illustrate three models to predict the effect of the independent contribution of different factors on KAP (Table 6). An overall model including sex, age, marital status, nationality, region, education, specialty, and seniority is statistically significant in predicting knowledge (F = 4.55, p<.001*). This Model explains 34.5% of the variability in the level of expertise of Physicians. Eastern region, Western region, and Endocrinology specialty are significant for contributing to the prediction of knowledge as b, t, p of these predictors, respectively [(.763, 2.338,.02) & (.660, 2.02,.045) and 1.15, 2.123, 035)]. At the same time, other factors did not significantly contribute to predicting knowledge.
Table 7 Over, all models, including sex, age, marital status, nationality, region, education, specialty, seniority, and knowledge level, are statistically significant in predicting attitude e as (F = 1.57, p=.044*), Model explains (16%) of variability in attitude score of Physicians. Married physicians are significant in predicting attitude as b, t, p (.825, 2.513, and.013, respectively), while other factors were non-significant.
(Table 8) Over, all models, including sex, age, marital status, nationality, region, education, specialty, seniority, knowledge level, and attitude, are highly statistically significant in predicting the practice of Physicians as (F = 3.427, p<.001*), Model explain (30.2%) of variability in practice of Physicians. Age, gender, years of experience, Eastern region, Married Physicians, widow Physicians, senior Physicians, and attitude are significant for predicting physicians’ practice as a p-value of these predictors <.05, while other factors were non-significant.
Discussion
This current study aims to evaluate the KAP of physicians in Saudi Arabia in terms of DKA management. Considering the results, the present study provided several crucial observations. Most tertiary hospitals in Saudi Arabia have established standardized protocols for DKA management, and adherence to these protocols by physicians in emergency departments, intensive care units, and medical wards is essential to safeguard patient safety and uphold high standards of medical practice.
Most physicians had a low knowledge of DKA management, and more than half had a score below the cut-off mark. However, only 42% of physicians in this study understood the MOH guidelines on managing DKA, and only 68.6% of physicians had a good attitude toward the MOH guidelines on DKA management. On the same note, weak practice behavior was recorded in the management of DKA, with only 51.7% of the physicians recording good practice behavior.
We also explored the key factors that influenced the KAP scores. Specifically, our analysis revealed that knowledge scores were notably higher among female physicians, older physicians, and those with over 15 years of experience. Additionally, endocrinologists and ICU physicians demonstrated the highest levels of knowledge. In contrast, particularly those under 30 and with less than 15 years of experience had considerably lower knowledge levels. Interestingly, we found a strong correlation between knowledge and practice, as well as knowledge and attitude, suggesting that individuals with a more favorable attitude toward the process tend to possess adequate knowledge.
The results of Alemam (21) study agree with our research, indicating that lack of knowledge, inappropriate attitudes, and practices were reported in 57.2, 58.2, and 62.6% of the studied PCPs, respectively. The previous study mentioned that age below 32, being unmarried, having Bachelor’s or Master’s degrees only, working experience for less than 5 years, and being in a GP position were significantly correlated with lack of knowledge, which goes hand in hand with the present study.
Our study also shows that knowledge was significantly higher among physicians with more than 15 years of experience, an observation supported by Onyiriuka et al. (22) who reported that a significantly higher proportion (36.7%) of physicians who have practiced for more than 10 years answered questionnaires correctly compared with their counterparts (22.2%) whose medical practice was 10 years or less.
Hepprich et al. discovered that 32% of Type 1 diabetic patients were unaware of DKA, and nearly half failed to identify either a symptom or a cause of DKA. This lack of knowledge correlated with the inadequate understanding of DKA management exhibited by more than 57% of physicians in the current study. Despite our research focusing on different groups—patients in their study and healthcare providers in ours—there exists an issue with DKA education throughout the continuum of care. Interestingly, Hepprich et al. also noted an overestimation of patients’ understanding of DKA and highlighted similar information deficits among healthcare professionals. These data imply variations in the knowledge and updates of healthcare providers. Also, the patients themselves may not have the technical expertise to manage DKA appropriately, indicating a need for continuous training. Our study is consistent with this line of research. It emphasizes the need for continuous, multi-faceted educational approaches to address the knowledge deficit and enhance DKA management results in alignment with the study of Hepprich et al. (23).
Hassan et al. reveal significant deficiencies in understanding DKA among diabetic patients and healthcare professionals. Only 42% of participants recognized DKA as an emergency, and merely 33% identified polydipsia as a key symptom. This concurs with our data that over half of the physicians had inadequate knowledge about DKA and its treatment, highlighting a widespread lack of awareness in the patient and medical communities. It is pertinent to mention that Hassan et al. primarily focused on diabetic patients from the northern and western regions of Saudi Arabia. Nevertheless, similar to Hassan et al. we emphasized the need for targeted educational initiatives to enhance clinicians’ understanding of DKA. Notably, Hassan et al. also investigated knowledge of DKA prevention and management among patients presenting in emergency departments. They also observed that many patients allowed to manage DKA believed that frequent self-monitoring of blood sugar was the best preventive strategy. This underscores the need for targeted, multi-faceted educational approaches to address these knowledge deficits and enhance DKA management results in alignment with the published data (24).
A cross-sectional study in the central region of Saudi Arabia aimed to assess the knowledge, attitudes, and practices related to diabetes among patients diagnosed with the condition. The findings indicated that the patients exhibited generally high knowledge scores (73.6%) and positive attitude scores (87.7%). However, their practice scores were notably low at 45%. The authors identified a moderate positive correlation between self-knowledge and attitude (r = 0.503, P < 0.001), as well as between knowledge and practice (r = 0.337, P < 0.001). Additionally, there was a lower positive correlation between attitude and practice (r = 0.235, P < 0.001). However, their poor practice scores show a pressing need to design better diabetes education programs that improve their knowledge and lead to improved practices in managing diabetics. This disparity between understanding and performance underlines the urgency for comprehensive patient education emphasizing self-management, to manage diabetic complications (25).
Knowledge gaps among physicians
According to our data, Elghamrawy et al. reported that although the majority recognize the typical symptoms of DKA, and select the appropriate therapeutic options for effectively managing DKA, there were still some gaps in knowledge, as a sizeable portion of the participants were unable to accurately identify several of the essential characteristics of DKA (26). Also, Madkhly et al. found that the majority of medical students had basic knowledge about diabetes, including its clinical aspects and therapy. On the other hand, there were certain knowledge gaps about DKA, however 76% were aware of the mode of insulin administration (27).
Similarly, Singh et al. assessed medical officers in primary health facilities. They found that while they had a solid understanding of T2DM, their knowledge of DKA was lacking, with only 50% recognizing its general characteristics and treatment. Despite the information deficiencies, our survey found that 68.6% of physicians had a positive disposition toward MOH recommendations for DKA care (28). This commitment to following established norms and guidelines for enhancing patient outcomes is reassuring and underscores the dedication of healthcare providers.
Powers et al. recognized diabetes as a significant public health issue, they emphasize that diabetes self-management education and support is crucial for effective diabetes management, yet there is a low participation rate in these programs (29). Specifically, many providers have misunderstandings about the necessity and effectiveness of self-management education and support, and they may have difficulty identifying when and how to make referrals. they cited that only 6.8% of privately insured individuals with newly diagnosed type 2 diabetes participated in diabetes self-management education and support within 12 months of diagnosis, and only 5% of Medicare participants receive diabetes self-management education and support during their first year of diagnosis. This low acknowledgment of diabetes self-management education and support as an essential component of diabetes treatment underscores a significant gap in care, highlighting a disparity between perception and a thorough comprehension of integrated care techniques (30). Our data reveals that merely 51.7% of physicians exhibited proficient practice in managing DKA despite a predominantly favorable disposition toward MOH standards. This divergence between attitude and practice underscores possible obstacles in applying information to clinical practice.
Hamelin et al. reported that majority of physicians reported the guidelines to be useful (83.6%); 54.6% of respondents were familiar with the guidelines, and 54.7% claimed to use them in clinical practice, thus underscoring the significance of resource access in knowledge application to practice (31). Although physicians possess a good comprehension of T2DM-related theory, the practical application of this information, especially about diagnostic criteria, such as HbA1c, is inadequate due to insufficient facilities and resources at these centers (32).
This corresponds with our observation that although physicians acknowledge the significance of specific tests and procedures, logistical limitations frequently hinder their ability to implement these procedures. Furthermore, physicians possessing higher knowledge ratings were more inclined to demonstrate positive attitudes and superior clinical practices (33). Our study revealed a favorable correlation among knowledge, attitude, and practice ratings, indicating that an increase in knowledge may enhance attitudes and, in turn, improve clinical practices in DKA care.
Implications for clinical practice and policy
The findings of this study have clinical significance for managing DKA in Saudi Arabia. Identified gaps highlight an urgent need to enhance KAP related to this life-threatening condition. More than half of the physicians demonstrate a knowledge gap, underscoring the urgency for continuous education and development initiatives. These efforts should target various medical specialties, particularly first-line physicians who are most likely to encounter these cases, and subsequently refer them to specialists, such as endocrinologists. Training should extend beyond general principles of DKA management to include practical decision-making skills, ensuring that physicians are fully equipped to handle DKA in real-world scenarios.
Recommendations and future directions
At the policy level, healthcare unit administrators should consider implementing uniform policies to manage DKA across various facilities. This approach would ensure that all patients receive the same high-quality care, regardless of location. Furthermore, incorporating regular audit and feedback cycles within the healthcare organization could help assess adherence to guidelines for managing DKA patients.
Based on the data from this study, physicians in Saudi Arabia have proposed several recommendations for future research and enhancements in managing DKA. There is a noticeable absence of comprehensive educational programs, which should be an essential component of continuing medical education. These programs should focus on theoretical knowledge and practical skills, particularly for emergency medicine physicians. To prevent inconsistencies or inefficiencies in DKA management, the Ministry of Health (MOH) should establish standardized clinical management guidelines for DKA, which should be regularly updated and disseminated to all clinics nationwide.
Additionally, targeted training initiatives should be implemented for high-risk physicians, especially those who are young and inexperienced, through mentorship programs involving qualified consultants in endocrinology and intensive care. Regular evaluations of DKA management practices within healthcare organizations should be conducted to assess compliance with clinical guidelines, using the results to enhance training efforts. Furthermore, it is crucial to develop patient education programs that improve understanding of DKA prevention and early identification, complementing the educational efforts of physicians.
Limitations
The primary limitation of this study is its reliance on cross-sectional study data, which captures information at a single point in time. As a result, it does not provide insights into changes in knowledge, attitudes, and practices (KAP) over time or reflect the evolving awareness within the community. Additionally, this research is based exclusively on the perceptions of the respondents, which raises the possibility of socially desirable responses; thus, participants may report a level of knowledge or adherence to guidelines that exceed their actual practices. Furthermore, the study’s participants were limited to medical specialists with at least two years of clinical practice and no general practice experience. This constraint in the study population might have hindered the generalization of the findings to the broader population of physicians.
Conclusion
The findings of this study offer a thorough evaluation of physicians’ KAP regarding the management of DKA in Saudi Arabia. The results indicate a significant lack of understanding and poor adherence to the best practices surrounding DKA; over half of the physicians misinterpreted at least one aspect of the condition, while the remaining physicians demonstrated favorable management practices. Such shortcomings are of concern, particularly given the severity of DKA and the associated high risk of morbidity and mortality. Factors such as age, experience, and specialty served as predictors, revealing that endocrinologists and ICU physicians exhibited higher levels of knowledge. In contrast, younger, less experienced physicians showed knowledge gaps in several key areas.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chandrasekaran P Weiskirchen R . The role of obesity in type 2 diabetes mellitus-An overview. Int J Mol Sci. (2024) 25:1882. doi: 10.3390/ijms 25031882, PMID: 38339160 PMC 10855901 · doi ↗ · pubmed ↗
- 2Puttanna A Padinjakara RNK . Diabetic ketoacidosis in type 2 diabetes mellitus. Pract Diabetes. (2014) 31:112–6. doi: 10.1002/pdi.1852 · doi ↗
- 3Centers for Disease Control and Prevention (CDC) . Diabetic Ketoacidosis. Virginia, USA: The American Diabetes Association (ADA) (2024).
- 4Widianti S . Analysis of dietary compliance on blood glucose level changes in diabetes mellitus patients. Nurs Case Insight J. (2024) 2:92–6. doi: 10.63166/12vqgv 63 · doi ↗
- 5Kumar A Gangwar R Ahmad Zargar A Kumar R Sharma A . Prevalence of diabetes in India: A review of IDF diabetes atlas 10th edition. Curr Diabetes Rev. (2024) 20:105–14. doi: 10.2174/1573399819666230413094200, PMID: 37069712 · doi ↗ · pubmed ↗
- 6Ahmed SH Zahid M Waseem S Zafar A Shaikh TG Sabri T . The current state of primary healthcare in Pakistan: a way forward for low-to-middle income countries. Primary Health Care Res Dev. (2024) 25:e 59. doi: 10.1017/S 1463423624000549, PMID: 39478436 PMC 11569849 · doi ↗ · pubmed ↗
- 7Asdaq SMB Mannasaheb BA Orfali R Shaikh IA Alshehri A Alghamdi A . Antidiabetic and antioxidant potential of Crocin in high-fat diet plus streptozotocin-induced type-2 diabetic rats. Int J Immunopathology Pharmacol. (2024) 38:03946320231220178. doi: 10.1177/03946320231220178, PMID: 38233742 PMC 10798082 · doi ↗ · pubmed ↗
- 8Nanditha A Susairaj P Satheesh K Raghavan A Snehalatha C Ramachandran A . The rising prevalence of type 2 diabetes among the youth in southern India—An ancillary analysis of the Secular T Rends in Diab Etes in India (ST Ri DE-I) study. J Diabetes. (2024) 16:e 13576. doi: 10.1111/1753-0407.13576, PMID: 38923743 PMC 11200006 · doi ↗ · pubmed ↗