AI-Enabled Customer Relationship Management Platforms for Patient Services in Health Care, Early Lessons From Governance, and Program-Level Outcomes
Anup Kant Gupta

TL;DR
This study explores how AI-powered CRM platforms improve patient services in healthcare through better affordability, adherence, and access.
Contribution
It presents early lessons and governance practices from four enterprise implementations of AI-enabled CRM in healthcare.
Findings
AI-enabled CRM platforms can enhance affordability in healthcare programs.
Governance practices are linked to improved patient adherence and access.
Program-level outcomes show promise in leveraging AI for patient services.
Abstract
This research letter summarizes early lessons from 4 enterprise implementations of artificial intelligence–enabled customer relationship management platforms in health care and describes governance practices associated with improvements in affordability, adherence, and access at program level.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
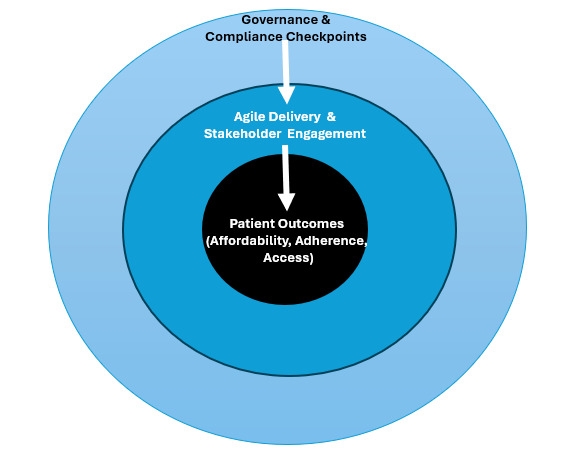 Figure 1
Figure 1| Patient service | Artificial intelligence functionality | Outcome | Example (anonymized) |
| Affordability | Automated co-pay verification | Reduced processing time (4 days to 3 days, a 25% improvement) | Fortune 10 rollout (USA) |
| Adherence | Predictive risk alerts | 12% reduction in therapy discontinuation | Consulting-led program |
| Access | Automated prior authorization | Therapy initiation shortened (20 days to 17 days, a 15% improvement) | Enterprise-wide program |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsArtificial Intelligence in Healthcare and Education · Electronic Health Records Systems · AI in Service Interactions
Introduction
Health systems continue to face pressure to improve patient outcomes while safeguarding affordability and equitable access [1-4]. Electronic health records support clinical workflows but are not designed for proactive patient outreach or service coordination [5]. Artificial intelligence (AI)-enabled customer relationship management (CRM) platforms support automated eligibility checks, outreach, and risk alerts [6-8]. This research letter summarizes early descriptive insights from enterprise implementations of AI-enabled CRM platforms.
Methods
Program Selection and Sampling Frame
A case-informed thematic analysis was conducted across 4 large health care programs. These were the largest CRM-based patient service deployments accessible to the author during this period. Programs were included if they had live AI-enabled CRM workflows for affordability, adherence, or access for at least 12 months. Each program operated independently with different teams, geographies, and product lines. Data reflect operations recorded between January 2019 and March 2024 across the 4 programs. All outcomes reflect a descriptive analysis of the operational dashboards and do not infer causal relationships.
Data Sources and Definitions
The following three data sources were used, each aggregated at program level.
Governance documents summarizing decision logs, compliance checkpoints, and escalation patterns.Stakeholder feedback was gathered through routine program review meetings and documented in standard internal templates.Internal dashboards tracking key operational indicators. These dashboards were deidentified, contained no patient level data, and were part of routine program monitoring.
Program level outcome metrics were defined as follows.
Adoption: proportion of active CRM users among provisioned patient service staff within a measurement window.Affordability efficiency: average time for co-pay or financial assistance verification.Therapy initiation time: average days between benefit verification and therapy start.Discontinuation rate: proportion of enrolled patients who stopped therapy during a defined period.
Baseline values came from preimplementation operations, and follow-up reflected the first stable post launch period. Findings are observational.
Ethical Considerations
This work used only aggregated, deidentified operational dashboards and program documents. No patient-level identifiable data or human subject interaction occurred. Institutional review board approval was not required.
Results
Theme 1: Patient Outcome Alignment and Sponsorship
Programs that centered goals on patient experience and outcomes such as therapy initiation time or affordability enrollment sustained stronger executive sponsorship. Programs framed as IT upgrades struggled to maintain alignment.
Theme 2: Continuous Engagement and Adoption
High adoption correlated with structured engagement of patient service teams and compliance officers. Regular feedback cycles supported adoption above 85% vs below 60% in minimally engaged programs [2].
Theme 3: Hybrid Governance Improved Delivery Efficiency
All 4 programs used a hybrid model that combined Agile sprints with scheduled compliance reviews. This approach reduced backlog resolution time by about 30%. Figure 1 summarizes the governance structure.
Hybrid governance framework for artificial intelligence–enabled customer relationship management. The framework illustrates three concentric layers: (1) patient outcomes (affordability, adherence, access) at the core, (2) agile delivery and stakeholder engagement in the middle layer, and (3) governance and compliance checkpoints in the outer layer. Arrows depict how governance structures enable engagement, which in turn drives improved patient outcomes.
Theme 4: Program-Level Improvements in Affordability, Adherence, and Access
Changes reflect aggregated dashboards and are not causal. Examples include a reduction in co-pay verification time from 4 days to 3 days (25% faster), a 12% reduction in therapy discontinuation rates, and a shortening of therapy initiation time from 20 days to 17 days (15% faster) (Table 1).
Discussion
Summary of Findings
Across 4 large-scale implementations, AI-enabled CRM platforms supported improvements in affordability, adherence, and access through workflow automation, risk identification, and coordinated service tasks. The most consistent predictors of success were early alignment with patient-centered outcomes, continuous stakeholder engagement, and hybrid governance structures.
Interpretation and Limitations
Results reflect aggregated, unaudited operational dashboards and cannot establish causality [9,10]. Findings describe program-level improvements observed post implementation and may not generalize to organizations with different scales, regulatory environments, or infrastructure maturity.
Future Directions
Future studies should incorporate multi-site comparative designs, validated outcomes, and integration with digital therapeutics and device streams to strengthen evidence for CRM-enabled patient service transformation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Digital Health and Innovation Global Strategy on Digital Health 2020–20252025 Geneva, Switzerland World Health Organization
- 2Greenhalgh T Wherton J Papoutsi C Lynch J Hughes GA'Court C Hinder S Fahy N Procter R Shaw S Beyond adoption, a new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale up, spread, and sustainability of health and care technologies J Med Internet Res 201711011911 e 367 10.2196/jmir.877529092808 v 19i 11e 36729092808 PMC 5688245 · doi ↗ · pubmed ↗
- 3Blease C Kaptchuk TJ Bernstein MH Mandl KD Halamka JD Des Roches CM Artificial intelligence and the future of primary care: exploratory qualitative study of UK general practitioners' views J Med Internet Res 20190320213 e 12802 10.2196/1280230892270 v 21i 3e 1280230892270 PMC 6446158 · doi ↗ · pubmed ↗
- 4Topol EJ High-performance medicine: the convergence of human and artificial intelligence Nat Med 201901251445610.1038/s 41591-018-0300-73061733910.1038/s 41591-018-0300-730617339 · doi ↗ · pubmed ↗
- 5Adler-Milstein Julia Holmgren A Kralovec P Worzala C Searcy T Patel Vaishali Electronic health record adoption in US hospitals: the emergence of a digital "advanced use" divide J Am Med Inform Assoc 2017110124611421148 10.1093/jamia/ocx 08029016973409135029016973 PMC 7651985 · doi ↗ · pubmed ↗
- 6Davenport T Kalakota R The potential for artificial intelligence in healthcare Future Healthc J 201906629498 10.7861/futurehosp.6-2-9431363513 S 2514-6645(24)01059-2PMC 661618131363513 · doi ↗ · pubmed ↗
- 7Obermeyer Z Emanuel EJ Predicting the future, big data, machine learning, and clinical medicine N Engl J Med 20160929375131216121910.1056/nejmp 160618127682033 PMC 5070532 · doi ↗ · pubmed ↗
- 8Jiang F Jiang Y Zhi H Dong Y Li H Ma S Wang Y Dong Q Shen H Wang Y Artificial intelligence in healthcare: past, present and future Stroke Vasc Neurol 20171224230243 10.1136/svn-2017-00010129507784 svn-2017-00010129507784 PMC 5829945 · doi ↗ · pubmed ↗