Magnesium Toxicity in an Obstetric Patient Due to Preeclampsia-Related Renal Dysfunction Despite Administration of a Standard Pritchard Regimen: A Case Report
Ndapewoshali L Pinehas, Ambrose Rukewe, Onochie U Nweze

TL;DR
A pregnant woman with eclampsia and kidney issues developed magnesium toxicity after standard treatment, requiring cesarean section, ventilation, and dialysis.
Contribution
Highlights magnesium toxicity risk in preeclampsia patients with renal dysfunction despite standard treatment protocols.
Findings
Magnesium toxicity occurred in a preeclampsia patient with renal dysfunction despite standard magnesium sulfate treatment.
Emergency cesarean section, mechanical ventilation, and hemodialysis were required for successful management.
Undetected hypermagnesemia can lead to severe maternal and fetal complications.
Abstract
Magnesium toxicity could occur in the treatment of preeclampsia/eclampsia, especially when the patient has coexisting renal impairment. If undetected and promptly treated, hypermagnesemia can cause severe fetomaternal complications and death. We present the case of a 22-year-old pregnant woman at 32 weeks of gestation, who was referred to our hospital with eclampsia, treated with intramuscular magnesium sulfate following a standard Pritchard regimen. An emergency cesarean section was carried out under general anesthesia due to multiorgan dysfunction. Following the cesarean delivery, she was successfully managed with mechanical ventilation and hemodialysis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
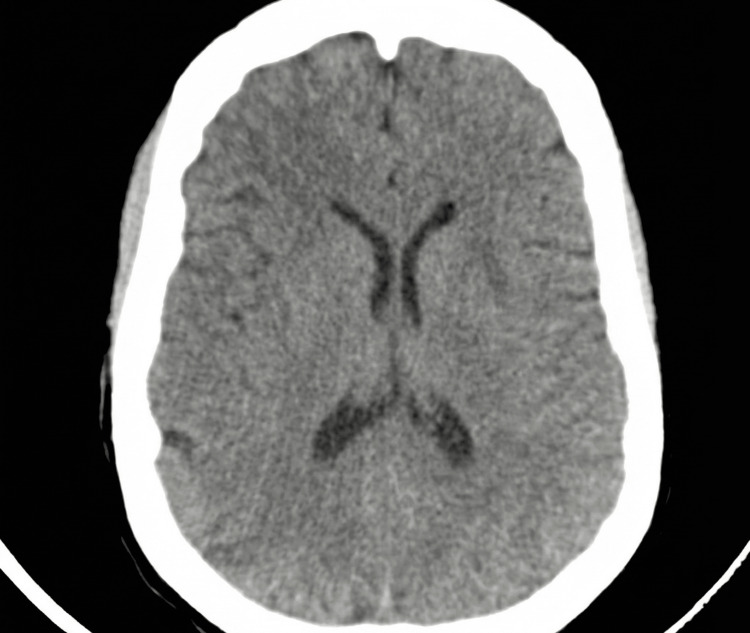 Figure 1
Figure 1| Variable | On admission | Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | Day 6 | Day 7 | Post-discharge | Reference range |
| Potassium (mmol/L) | 3.5 | 3.3 | 4.0 | 4.6 | 4.3 | 5.1 | 5.7 | 4.9 | 3.4 | 3.5-5.1 |
| Sodium (mmol/L) | 138 | 139 | 139 | 135 | 133 | 134 | 136 | 138 | 142 | 136-145 |
| Urea (mmol/L) | 14.6 | 15.7 | 18.7 | 23.9 | 15.8 | 23.2 | 27.8 | 25.4 | 6.0 | 2.9-8.2 |
| Creatinine (μmol/L) | 311 | 349 | 457 | 567.7 | 453 | 668 | 773 | 649 | 55.4 | 64-108 |
| Calcium (mmol/L) | - | 2.27 | 2.06 | 2.38 | 2.20 | 2.34 | 2.22 | 2.16 | 1.76 | 2.1-2.6 |
| Phosphate (mmol/L) | - | 2.68 | 2.26 | 2.32 | 1.40 | 1.83 | 1.76 | 0.85 | 0.33 | 0.8-1.5 |
| Magnesium (mmol/L) | - | >3.9 | >3.9 | >3.9 | 1.9 | 1.88 | 1.82 | 1.34 | 1.16 | 0.7-1.0 |
| Total protein (g/dL) | - | 56 | 44 | 48 | 44 | 49 | 45 | 52 | 61 | 6.0-8.3 |
| Albumin (g/dL) | - | 24 | 21 | 20 | 17 | 17 | 15 | 17 | 25 | 3.4-5.5 |
| Bilirubin (mg/dL) | - | 99 | 36 | 14 | 10 | 9 | 9 | 8 | 16 | 0.1-1.2 |
| ALT (IU/L) | - | 194 | 155 | 128 | 91 | 79 | 63 | 57 | 69 | 10-40 |
| AST (IU/L) | - | 352 | 193 | 101 | 62 | 66 | 72 | 55 | 79 | 10-35 |
| ALP (IU/L) | - | 153 | 133 | 157 | 165 | 203 | 236 | 288 | 342 | 30-130 |
| Hemoglobin (g/dL) | 8.8 | 8.4 | 7.2 | 7.3 | 7.1 | 6.9 | - | 6.6 | 9.4 | >11 |
| Platelets (×10⁹/L) | 37 | 68 | 67 | 83 | 100 | 139 | 244 | 382 | 435 | 150-400 |
| Variable | Before ventilatory support | After ventilatory support | Reference range |
| pH | 6.8 | 7.34 | 7.35-7.45 |
| pCO2 (mmHg) | 61.7 | 19.5 | 35-45 |
| pO2 (mmHg) | 93 | 140 | 75-100 |
| HCO3 (mmol/L) | 11.3 | 10.4 | 22-29 |
| O2 saturation (%) | 90.4 | 96.2 | 95-100 |
| Lactate (mmol/L) | 2.49 | 1.9 | 0.5-2.2 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPregnancy and preeclampsia studies · Magnesium in Health and Disease · Preterm Birth and Chorioamnionitis
Introduction
Magnesium sulfate is the first-line treatment for seizure prophylaxis in severe preeclampsia and the control of seizures associated with eclampsia. Despite having a low therapeutic index, hypermagnesemia in obstetric patients is rare, but some case reports have described severe complications, including deaths from overdose or under-excretion caused by renal impairment [1-3].
We present this case of magnesium toxicity in an eclamptic patient with renal insufficiency, as a complication treated with one of the recommended magnesium sulfate regimens (Pritchard), to highlight the need for cautious administration and close monitoring in low-resource settings.
Case presentation
A 22-year-old female patient (gravida 4 and para 3) at 32 weeks of gestation was referred to our hospital with a diagnosis of eclampsia complicated by hemolysis, elevated liver enzymes, and low platelets (HELLP syndrome). She was taken to the local health center after two episodes of seizure at home. Upon arrival at the center, she had another clonic-tonic seizure, and her blood pressure (BP) was 167/106 mmHg, pulse rate 91/min, random blood sugar was 8.8 mmol/L, and urine output via urethral catheter was 500 mL. Magnesium sulfate was administered using the Pritchard regimen (a loading dose of 4 g of magnesium sulfate in 200 mL saline intravenously over 10 minutes, followed by intramuscular injections of 5 g of magnesium sulfate in each buttock, making a total of 14 g). The patient was a known chronic hypertensive who had defaulted on methyldopa for two years. Sublingual nifedipine 10 mg and oral methyldopa 250 mg eight hourly were added. After being stabilized for 2 hours 30 minutes, she was transferred to a nearby district hospital.
Upon arrival at the district hospital, BP was 154/110 mmHg, pulse rate 85, and urine dipstick revealed protein ++. Intramuscular hydralazine 6.25 mg was administered, but the BP remained uncontrollable. Magnesium sulfate was continued at a dose of 5 g intramuscularly four hourly on alternate buttocks; she received four doses totaling 20 g. Altogether, she got 34 g of magnesium sulfate (14 g at the health center and 20 g at the district hospital). She was said to be in the latent phase of labor, with one contraction in 10 minutes lasting 26 seconds; vaginal examination revealed a 1 cm dilated cervix, 50% effaced, station level -1, and intact membranes. The fetal assessment on ultrasound revealed an alive, singleton, intrauterine pregnancy with good cardiac activity, cephalic presentation, estimated fetal weight 1.674 kg, and gestational age 31 weeks and 2 days. The patient was then transferred to the Windhoek Central Hospital.
On examination at our hospital, the patient appeared ill-looking, with altered consciousness (Glasgow Coma Scale (GCS) was 12/15; E = 3, V = 4, and M = 5) and complete loss of patella reflex (which corresponds to zero on a standard deep tendon reflex scale). Her cardiovascular and respiratory system examination was unremarkable (BP was 129/69 mmHg, pulse rate was 97/min, respiratory rate was 20/min, and SaO₂ averaged less than 92% on room air). She was oliguric (700 mL/24 hours), and her urine was dark brown in color. Her laboratory workup results showed elevated levels of urea (14.6 mmol/L), creatinine (311 μmol/L), magnesium (>3.9 mmol/L), alanine transaminase (229 IU/L), aspartate transaminase (717 IU/L), and low platelet count of 37 × 10⁹/L (Table 1). The CT scan of the brain (Figure 1) was suggestive of posterior reversible encephalopathy syndrome (PRES), with no signs of hemorrhage or acute ischemic injury. The diagnosis of eclampsia with HELLP syndrome, acute kidney injury (based on rising serum creatinine levels and significant oliguria (<0.5 mL/kg/hr)), and magnesium toxicity was made. The immediate management involved the administration of 10% intravenous calcium gluconate, 10 mL slowly over 10 minutes. Calcium gluconate was repeated eight hours later. Abdominal ultrasound reported both kidneys as slightly hyperechoic, with reduced corticomedullary differentiation; the right kidney measured 9.7 × 4.0 cm, and the left kidney measured 11.0 × 5.8 cm. No focal lesion, hydronephrosis, or perinephric collections bilaterally; the urinary bladder was empty; uterus normal, no obvious pelvic collections; liver normal, gallbladder with sludge inside; no ductal dilatation or features of cholecystitis; spleen normal; no ascites. No electrocardiography (ECG) was done.
Computed tomography brain indicative of posterior reversible encephalopathy syndrome (PRES)
The decision to deliver the baby operatively was made 16 hours after admission due to multi-organ dysfunction secondary to eclampsia. An emergency cesarean section was performed under standard endotracheal general anesthesia, without muscle relaxant technique, which lasted about 30 minutes. Intraoperatively, the patient was hemodynamically stable, with BPs ranging 108/56-120/64 mmHg, pulse rate 86-92/min, and SaO₂ 96%-99%. The estimated blood loss was 300 mL. A 1.945 kg male baby was delivered, with an Apgar score of 2/10 at 1 minute, 6/10 at 5 minutes, and 8/10 at 10 minutes following resuscitation by the attending neonatologist. The baby was then transferred to the neonatal intensive care unit (NICU) for respiratory support and observation.
The patient remained intubated, admitted to the ICU, and ventilated on pressure-controlled synchronized intermittent mandatory ventilation (PC-SIMV) mode, as the arterial blood gas (ABG) showed metabolic acidosis without respiratory compensation (Table 2). On days 1-3, the laboratory workup (Table 1) revealed worsening oliguria and deteriorating liver and renal functions (rising creatinine levels and liver enzymes), but the serum magnesium was reported to be >3.9 mmol/L (our laboratory did not report the peak magnesium level over the three days). Four more doses of calcium gluconate were administered. She had two sessions of hemodialysis on days 3 and 4, after which her serum magnesium levels reduced to 1.8 mmol/L, and urine output improved.
The patient was successfully weaned off the mechanical ventilator and discharged from the ICU on day 7, in a stable clinical condition, with normal renal function and no neurological deficit.
Discussion
This case report highlights the importance of careful administration of magnesium sulfate and close monitoring of patients treated for severe preeclampsia with co-existing renal compromise. Hypermagnesemia often results from accidental overdose in the absence of kidney disease, or, as in this index case, from under-excretion due to preeclampsia-related renal dysfunction [1,4-6]. It was significant that this patient had a positive history of chronic hypertension and two years of non-compliance with antihypertensive medication.
Preeclampsia, a pregnancy-associated hypertension and proteinuria, has a 2%-8% global prevalence and is a significant cause of fetomaternal morbimortality, especially in low- and middle-income countries (LMICs). Magnesium sulfate is the drug of choice for prophylaxis of eclampsia in patients with severe preeclampsia and the treatment of eclampsia [7-9]. The patient received 34 g of magnesium sulfate in 24 hours, which was within the recommended daily dose range according to the Pritchard regimen. A healthy kidney would excrete at least 90% of this dose during the first 24 hours; this was not possible in our patient. The Zuspan regimen (4 g intravenous injection over 10-15 minutes, followed by 1 g per hour for 24 hours), with a relatively lower overall dose, would be less hazardous. The total dose in 24 hours in the Dhaka regimen is marginally less by 3 g than Zuspan’s. Furthermore, a study found a 12-hour modification of the Zuspan regimen with about 40% less overall dose, non-inferior to the standard 24-hour treatment [3,10,11]. According to Agarwal et al., low-dose regimens are effective, reduce the risk of magnesium toxicity, and are advisable in low-resource settings where serum magnesium assays are not feasible [12]. However, the ease of intramuscular injections in rural health centers, like the one this patient was taken to after the seizures, makes the Pritchard regimen popular [13].
In our patient, we could not determine the peak serum magnesium level, as the laboratory result on days 1-3 was >3.9 mmol/L despite worsening oliguria, and ABG, which depicted severe metabolic acidosis without respiratory compensation, along with rising serum creatinine concentrations indicating deteriorating renal function. If an ECG evaluation had been done, it would have flagged magnesium toxicity, as a prolonged PR interval and widened QRS are early warning signs. However, her cloudy sensorium, loss of patella reflex, and need for ventilatory support (ostensibly from muscle weakness) were suggestive of moderate to severe magnesemia - an estimate up to or more than 5 mmol/L based on these clinical features, in the absence of actual measurement, since the toxic effects are related to serum magnesium levels. This brings into focus the failure of our laboratory to report the exact serum level. The administration of intravenous calcium gluconate probably reduced the risk of cardiac arrhythmias [5]. The decision for cesarean delivery was beneficial in view of maternal multiorgan dysfunction, but the low Apgar score at birth might be due to elevated ionized magnesium levels from placental transfer, causing hypotonia that necessitated resuscitation and NICU admission [14]. We cannot confirm this in the neonate, since the neonatal magnesium level was not measured. It is noteworthy that the severity of magnesium toxicity in this patient was hampered by obvious laboratory limitations, such as a lack of ECG, no available peak serum magnesium level, and inconclusive ABG results, in keeping with our low-resource practice environment.
Her admission into the ICU for ventilatory support and hemodialysis restored the physiologic magnesium levels and renal function in keeping with the international guideline that hemodialysis treatment is required if kidney function is impaired [15]. Failure to correct the toxic magnesium levels would have worsened the respiratory compromise and led to cardiac arrest, which was avoided in this case.
Conclusions
In a low-resource setting, consider a lower magnesium sulfate dose that would prevent or manage eclampsia, and prompt hemodialysis should be employed if renal impairment co-exists. Routine clinical and laboratory workups of patients treated with magnesium sulfate should include assessment of patella reflexes, respiratory rate, ECG, blood biochemistry, and ABG.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Accidental intravenous infusion of a large dose of magnesium sulphate during labor: a case report J Anaesthesiol Clin Pharmacol Kumar K Al Arebi A Singh I 3773792920132410636510.4103/0970-9185.117105 PMC 3788239 · doi ↗ · pubmed ↗
- 2Cardiopulmonary arrest after the administration of magnesium sulphate. A case report S Afr Med J Richards A Stather-Dunn L Moodley J 145671985 https://pubmed.ncbi.nlm.nih.gov/3969602/3969602 · pubmed ↗
- 3Magnesium sulfate in eclampsia and pre-eclampsia: pharmacokinetic principles Clin Pharmacokinet Lu JF Nightingale CH 3053143820001080345410.2165/00003088-200038040-00002 · doi ↗ · pubmed ↗
- 4Acute magnesium toxicity in an obstetric patient undergoing general anaesthesia for caesarean delivery Int J Obstet Anesth Mc Donnell NJ Muchatuta NA Paech MJ 2262311920102021934510.1016/j.ijoa.2009.09.009 · doi ↗ · pubmed ↗
- 5Iatrogenic magnesium toxicity following intravenous infusion of magnesium sulfate: risks and strategies for prevention BMJ Case Rep Cavell GF Bryant C Jheeta S 2094992015201510.1136/bcr-2015-209499 PMC 452152326231187 · doi ↗ · pubmed ↗
- 6An integrative review of the side effects related to the use of magnesium sulfate for pre-eclampsia and eclampsia management BMC Pregnancy Childbirth Smith JM Lowe RF Fullerton J Currie SM Harris L Felker-Kantor E 341320132338386410.1186/1471-2393-13-34PMC 3570392 · doi ↗ · pubmed ↗
- 7Risk factors of pre-eclampsia/eclampsia and its adverse outcomes in low- and middle-income countries: a WHO secondary analysis P Lo S One Bilano VL Ota E Ganchimeg T Mori R Souza JP 09201410.1371/journal.pone.0091198 PMC 396237624657964 · doi ↗ · pubmed ↗
- 8Public health perspectives of preeclampsia in developing countries: implication for health system strengthening J Pregnancy Osungbade KO Ige OK 481095201120112154709010.1155/2011/481095 PMC 3087154 · doi ↗ · pubmed ↗