ANEURYSMAL BONE CYST: A CASE SERIES OF AN AGGRESSIVE BENIGN TUMOR
Caio Falk Giannotti, Nathalia Sundin Palmeira de Oliveira, Jairo Greco Garcia, Marcelo de Toledo Petrilli, Dan Carai Maia Viola, Reynaldo Jesus Garcia

TL;DR
This case series evaluates treatment outcomes and recurrence rates in patients with aneurysmal bone cysts, a benign but aggressive bone tumor.
Contribution
The study provides epidemiological data and treatment outcomes for aneurysmal bone cysts in a pediatric cohort.
Findings
The overall recurrence rate of aneurysmal bone cysts was 30.4%.
No significant association was found between recurrence and variables like sex, age, or treatment type.
Most cysts were located in the lower limbs, and surgery with bone grafting was the most common treatment.
Abstract
The Aneurysmal Bone Cyst (ABC) is a benign yet aggressive bone tumor. This study aimed to evaluate sex, age, tumor location, tumor size, type of treatment (surgical, infiltration, embolization), and recurrence. Descriptive and quantitative statistical analyses were applied. The prevalence ratio and 95% confidence interval were calculated for the association between recurrence and sex, age, tumor size, Capanna's classification, and treatment type. Twenty-three cases of ABCs were included, eleven (47.8%) females and twelve (52.2%) males. The mean age of treated patients was 11.2±1.8 years. Most cysts were located in the lower limbs (56.5%). The mean follow-up time was 42.8±14.01 months. The mean cyst diameter at the beginning of treatment was 5.58± 1.04 cm; of these, 17.4% were up to 3 cm, 43.5% from 3.1 to 6 cm, and 39.1% over 6 cm. Regarding initial treatment, 6 (26%) patients…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
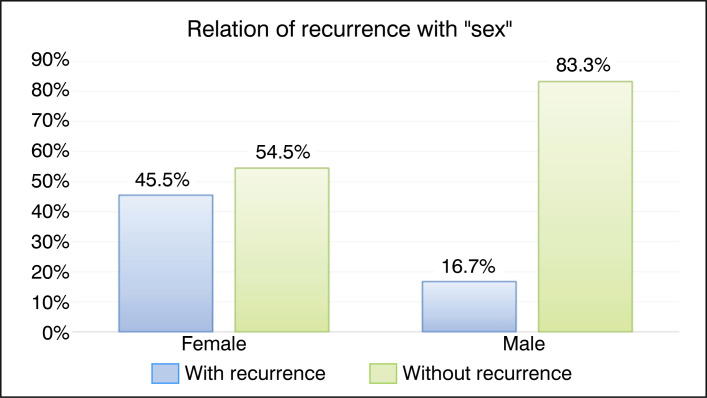 Figure 1
Figure 1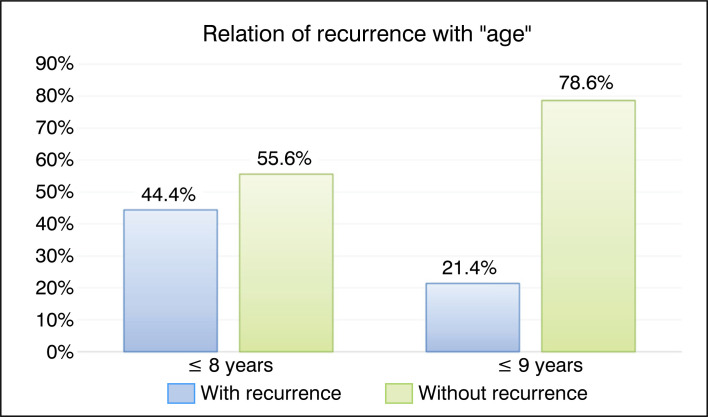 Figure 2
Figure 2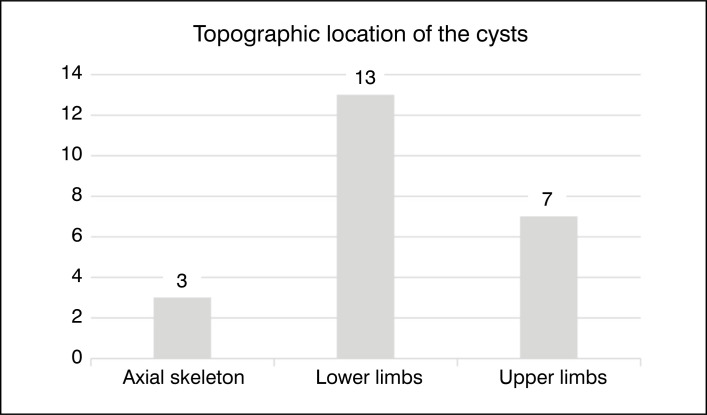 Figure 3
Figure 3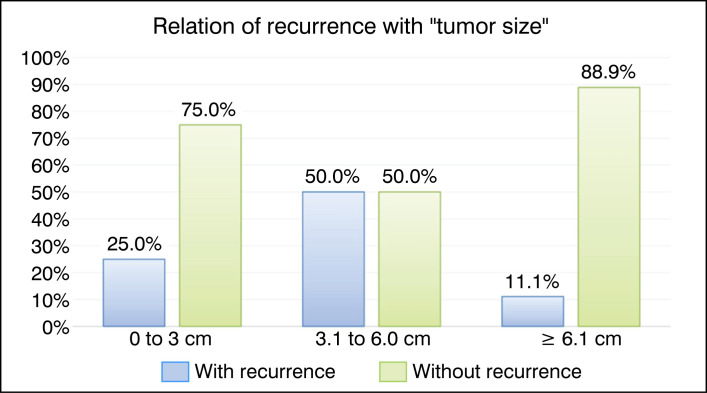 Figure 4
Figure 4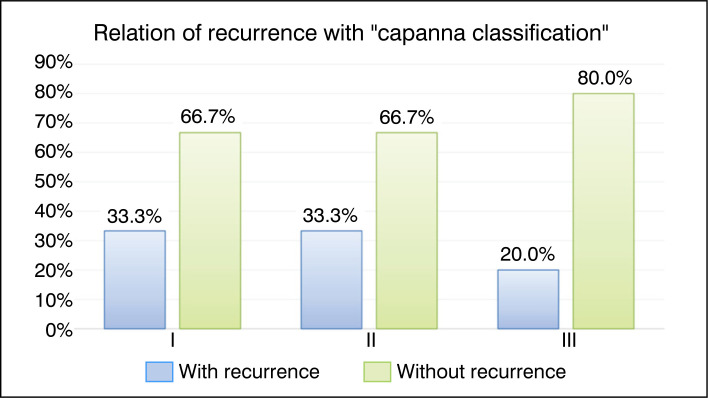 Figure 5
Figure 5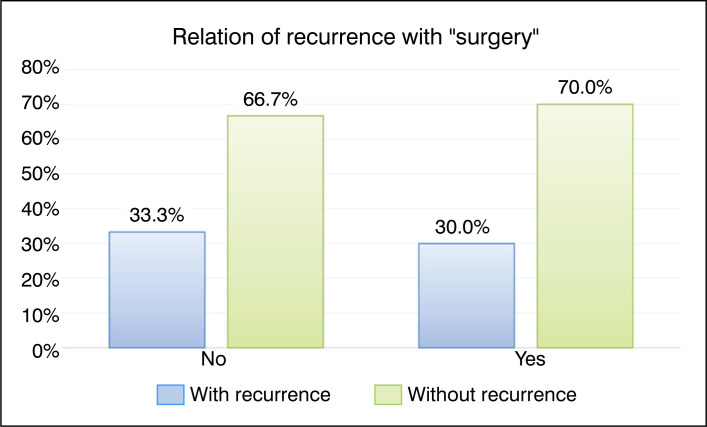 Figure 6
Figure 6| Cases | Sex | Age | Location | Cyst size (largest measurement) | Capanna classification | Type of treatment | Recurrence |
|---|---|---|---|---|---|---|---|
| 1 | F | 16 | Humerus | 4.5 cm | I | C | Yes |
| 2 | M | 14 | Tibia | 8.6 cm | III | C | No |
| 3 | F | 12 | Tibia | 6.0 cm | II | C | Yes |
| 4 | F | 12 | Tibia | 4.6 cm | III | C | No |
| 5 | F | 7 | Fibula | 5.0 cm | II | C | No |
| 6 | M | 6 | Column | 3.2 cm | II | I + E | No |
| 7 | M | 17 | Fibula | 10.6 cm | II | C | No |
| 8 | M | 8 | Metatarsus | 2.2 cm | I | C | No |
| 9 | M | 18 | Pelve | 6.9 cm | II | I | No |
| 10 | F | 4 | Tibia | 4.2 cm | III | C | Yes |
| 11 | M | 6 | Tibia | 7.0 cm | II | I | Yes |
| 12 | F | 8 | Femur | 7.0 cm | III | I + C | No |
| 13 | M | 15 | Metacarpus | 4.5 cm | II | C | No |
| 14 | M | 15 | Column | 6.2 cm | II | E + C | No |
| 15 | M | 6 | Metacarpus | 2.4 cm | II | C | No |
| 16 | F | 6 | Metacarpus | 2.4 cm | II | C | Yes |
| 17 | F | 8 | Talus | 4.2 cm | II | I + C | Yes |
| 18 | M | 13 | Tibia | 8.5 cm | III | C | No |
| 19 | F | 15 | Femur | 11.2 cm | II | I + C | No |
| 20 | F | 17 | Radius | 2.8 cm | I | C | No |
| 21 | M | 14 | Clavicle | 3.4 cm | II | C | No |
| 22 | F | 9 | Femur | 7.5 cm | II | C | No |
| 23 | M | 12 | Humerus | 5.5 cm | II | C | Yes |
| With Recurrence | Without Recurrence | PR (CI 95%) | P-value | ||||
|---|---|---|---|---|---|---|---|
| N | % | N | % | ||||
| Sex | Female | 5 | 45.5% | 6 | 54.5% | Ref. | 0.124 |
| Male | 2 | 16.7% | 10 | 83.3% | 0.37 (0.10 to 1.36) | ||
| Age | ≤ 8 years | 4 | 44.4% | 5 | 55.6% | Ref. | 0.187 |
| ≥ 9 years | 3 | 21.4% | 11 | 78.6% | 0.48 (0.14 to 1.64) | ||
| Tumor size | 0 to 3 cm | 1 | 25.0% | 3 | 75.0% | 0.50 (0.10 to 2.45) | 0.336 |
| 3.1 to 6.0 cm | 5 | 50.0% | 5 | 50.0% | Ref. | - x - | |
| ≥ 6.1 cm | 1 | 11.1% | 8 | 88.9% | 0.22 (0.04 to 1.12) | 0.084 | |
| Surgery | No | 1 | 33.3% | 2 | 66.7% | Ref. | 0.474 |
| Yes | 6 | 30.0% | 14 | 70.0% | 0.90 (0.15 to 5.26) | ||
| Capanna Classification | I | 1 | 33.3% | 2 | 66.7% | Ref. | - x - |
| II | 5 | 33.3% | 10 | 66.7% | 1.00 (no CI) | 0.485 | |
| III | 1 | 20.0% | 4 | 80.0% | 0.60 (0.06 to 6.45) | 0.536 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone Tumor Diagnosis and Treatments · Bone fractures and treatments · Oral and Maxillofacial Pathology
INTRODUCTION
The aneurysmal bone cyst (ABC) was first described by Jaffe and Lichtenstein, then known as Jaffe-Lichtenstein Disease.^ 1 ^ Previously classified as a pseudotumoral lesion, it was reclassified in 2020 in the World Health Organization's tumor classification compendium as a benign tumor lesion and grouped with giant cell tumor and non-ossifying fibroma as osteoclastic lesions rich in giant cells.^ 2 ^ This occurred after the finding that the pathogenesis of ABC originates from the translocation of the USP6 gene, evidenced by in situ hybridization in situ by fluorescence (FISH).
This tumor most frequently affects children and young adults, mainly in the second decade of life, with a slight predominance in females.^ 3 ^ The lesions preferentially occur in the metaphysis of long bones, predominantly in the femur, tibia, and humerus.^ 4 ^ Although rare, they can occur in small tubular bones such as metacarpals, metatarsals, and phalanges.^ 5–7 ^ In lesions of the spine and pelvis, they represent greater difficulty for surgical treatment.^ 8–10 ^
The radiological characteristic is a lytic lesion, typically eccentric and expansive, with a preference for the metaphyseal region of long bones. Lytic lesions may present cortical thinning and widening of the affected segment.^ 2,3 ^ The appearance of the lesions shows marked thinning of the cortex over the site, with minimal bone formation; changes are sometimes better visualized on computed tomography or magnetic resonance imaging.^ 11 ^
Although ABC is benign, there may be clinical and imaging characteristics that denote aggressiveness.^ 10 ^ Surgical treatment options include simple resection in non-displaceable bones or curettage of the lesion, associated with local adjuvant therapy and filling the tumor bed with bone graft or polymethylmethacrylate.^ 10,11 ^ The prognosis after treatment is considered good, although about 20% of cases present recurrence.^ 10 ^ A treatment program based on the evaluation of the morphological type and aggressiveness of these tumors is recommended and recognized as the Capanna Classification.^ 12 ^ The aim of our study was to evaluate a series of cases of children and adolescents with aneurysmal bone cysts and compare the treatment outcomes.
METHODS
A retrospective case series study on the aneurysmal bone cyst was conducted. Data were compiled from patients’ electronic clinical and imaging records, and a specific database was created for the study with full protection of patient identity. The study was approved by the institutional Ethics Committee and is registered in the Brazil Platform under the number CAE 25729119.0.0000.5505.
The records of 23 patients who underwent surgical and/or clinical treatment for cystic lesions suggestive of ABC with the first consultation in the service between January 1, 2005, and December 31, 2023, were analyzed.
The inclusion criteria for the study were patients with an anatomopathological diagnosis of aneurysmal bone cyst, aged between 1 and 30 years at diagnosis, treated at the institution, and who agreed to participate in the study, with signed informed consent and assent form. The exclusion criterion was noncompliance by the patient or their legal representative with participating in the study at any time. We used Microsoft Excel (Microsoft Office®) for creating the database and tables, and SPSS® V26 (2019) and Minitab 21.2 (2022) for statistical analysis.
All patients were evaluated according to the epidemiological variables: (1) sex; (2) age; (3) tumor location; (4) tumor size (largest diameter); (5) Capanna radiological classification for ABCs;^ 12 ^ (6) type of treatment performed (surgical, calcitonin injection, embolization, or a combination of modalities), (7) follow-up time in months, and (8) recurrence of the lesion. Epidemiological analyses of the studied variables were performed, with description of categorical variables (frequency and percentage) and continuous variables (mean and standard deviation). Fisher's exact test was used in analyses where the smallest frequency studied was less than 5. The prevalence ratio was calculated with a 95% confidence interval.
RESULTS
Table 1 presents complete data on sex, age, location, size, classification, type of treatment (infiltration, embolization, surgery), and recurrence status.
Twenty-three patients were included in the study, with eleven (47.8%) being female and twelve (52.2%) being male. As this is a pediatric hospital, the average age of the treated patients was 11.2±1.8 (4 to 18 years). The graphs in Figures 1 and 2 compare recurrence with the factors "Sex" and "Age", respectively. The results were not statistically significant.
Bar graph of the relationship between recurrence and the qualitative factor "sex".
Bar graph of the relationship between recurrence and the qualitative factor "age".
Regarding the location of the ABC, we observed that the vast majority were located in the lower limbs (56.5%). Figure 3 shows the distribution of the topographic location of the ABCs.
Graph of the distribution of the topographic location of Aneurysmal Bone Cysts: Axial skeleton (pelvis and spine); Lower limbs; Upper limbs.
The tumor sizes were evaluated as the average of the largest diameter on the initial treatment radiograph, which was 5.58±1.04 cm, with the smallest 2.2 cm and the largest 11.2 cm. Of these, 17.4% corresponded to cysts up to 3 cm, 43.5% from 3.1 to 6 cm, and 39.1% to cysts above 6 cm. The comparison of these factors with recurrence is illustrated in the graph in Figure 4, but the result was not statistically significant.
Bar graph of the relationship between recurrence and the qualitative factor "tumor size."
The radiographic classification of Capanna for the ABC was proposed in 1985, based on the radiographic appearance and morphology of these tumors. The classification is divided into five subgroups, as shown in Figure 2. Type I represents lesions centered in the metaphysis, without causing cortical thinning or expansion. Type II involves expansive tumors with cortical thinning that completely involve the affected metaphysis. Type III is the most common type reported by Capanna et al., characterized by an eccentric metaphyseal lesion that typically affects only one cortex. Type IV corresponds to subperiosteal lesions, which grow away from the bone, and type V involves periosteal lesions that expand around the bone and eventually penetrate the cortex below.^ 12 ^ Figure 5 presents a comparative graph of recurrence rates for the types of Capanna found in the study patients, with equivalent recurrence rates for types I and II and slightly lower for type III.
Bar graph of the relationship between recurrence and the qualitative factor "Capanna Classification."
Regarding treatment, 6 (26%) patients received infiltration: 5 (83.3%) received calcitonin infiltration, and 1 (16.7%) received dexamethasone and calcitonin infiltration. The dose of each calcitonin infiltration was three ampoules (3 ml) at a concentration of 100 UI/ml. In the case involving the association of calcitonin with dexamethasone, the dose was 2.5 ml at a concentration of 2 mg/ml. Of the patients treated with infiltration, two (33.4%) underwent surgical treatment after recurrence.
Two patients in total (8.6%) underwent embolization for local control. Both cases were of cysts located in the spinal column, and of them, only one underwent surgery for curettage and grafting at a later time. In total, twenty (86.9%) patients underwent surgery with bone autograft. The surgical treatment of all cases consisted of intralesional resection with extensive curettage, associated with local thermal (electrocautery or Argon scalpel) or chemical (absolute alcohol) adjuvant therapy, followed by grafting in the tumor bed using autograft from the iliac crest. Figure 6 presents a comparative graph of patients who underwent surgery and those who did not, and their respective recurrence rates. Although it shows a slight reduction in the recurrence rate among cases submitted to surgical intervention, the difference is not statistically significant.
Bar graph of the relationship between recurrence and the qualitative factor "Surgery."
The follow-up time was defined as the period from the first consultation in the service to the last consultation included in the study, yielding an average of 42.8±14.1 months (3 to 127 months).
The overall recurrence rate was 30.4% (n=7). We considered the cases that recurred in which there was progression of the size of the radiolucent image in the treated area in two consecutive follow-up X-rays or in which the attending physician reported, in the medical record, the diagnosis of recurrence. In the groups treated with a single method (surgery, infiltration, or embolization), the recurrence rate was 33.4%. In the group that combined the two methods, the recurrence rate among those who started treatment with surgery was 20% (1 in 5 cases). There was no recurrence in the only case initially treated with embolization and then surgery, nor in the only case treated with embolization associated with infiltration, both located in the spine.
Table 2 presents the prevalence and the bivariate analysis of the association between recurrence and the other variables mentioned. We did not identify any association between the investigated variables. Only one patient developed a pathological fracture, 90 months after curettage and grafting. Initially, conservative treatment was attempted with a cast to perform a new curettage and grafting at a later time. The case was re-evaluated, and a new curettage and grafting, followed by internal fixation with plate and screws, was chosen after 17 days of conservative treatment. By the end of this study, the aforementioned patient is three years post-operative with satisfactory consolidation and no signs of recurrence.
DISCUSSION
The aneurysmal bone cyst (ABC) is a benign neoplasm rich in giant cells, cystic in appearance, multiloculated, and containing blood.^ 2 ^ Although current medical literature presents several works with case series on ABC,^ 3–7 ^ there is a lack of studies in Brazil conducted with children and adolescents treated in specialized orthopedic oncology institutions.
In the present study, aneurysmal bone cyst was the predominant lesion in male children and adolescents. This finding differs from the data found in national^ 13 ^ and international literature.^ 14,15 ^ In fact, most patients diagnosed with ABC are children and adolescents.^ 13 ^ ABC can occur in childhood and early adulthood, and there is a slightly increased incidence rate in women (1 to 1.3).^ 13,15 ^
In our case series, the cysts were predominantly located in the lower limbs, including the tibia, femur, talus, and metatarsus. Although ABC can occur in any bone, it usually affects the metaphysis of long bones, such as the femur and tibia.^ 13,15 ^ It can also affect the vertebrae and pelvis.^ 13,15 ^ The diagnosis should be confirmed by biopsy and histopathological evaluation.^ 15 ^ ABC is an aggressive benign tumor that often presents with pain, pathological fracture, and may show local recurrence after treatment.^ 10,13,16 ^
In this study, most cases of ABC presented radiological classification of Capanna type II, that is, a central expansive lesion affecting the entire bone diameter, promoting cortical thinning. Another study also conducted in Brazil^ 14 ^ and international studies also found in their sample a higher prevalence of Capanna type II lesions,^ 17,18 ^ although in its original description, Capanna states a higher prevalence of type II.^ 12 ^ We did not find in our study, among the included patients, lesions of classification IV or V.
The treatments included infiltration (calcitonin or dexamethasone + calcitonin), embolization for cases involving the spine, and surgery with graft placement. Once ABC is suspected, the patient should be referred to an orthopedic oncologist.^ 13 ^ Since it is a bone lesion that may present as active with aggressive and destructive characteristics of the bone, the aneurysmal bone cyst is indicated for intervention. The most frequently performed treatment, according to the literature, is intralesional resection, with curettage of the lesion.^ 2,11,12 ^
The use of local adjuvants (phenol, absolute alcohol, electrocautery, argon scalpel) is recommended to optimize tumor cell destruction after curettage, and the affected area should subsequently be filled with bone graft (autologous or homologous) or polymethylmethacrylate (PMMA).^ 11 ^ Extensive lesions and/or those involving joints may be treated with marginal or even wide resection, requiring reconstruction of the joint (endoprosthesis) or the affected bone segment.^ 11 ^ Endovascular embolization of the arteries supplying the lesion can be performed, aiming to achieve local control in large or surgically difficult-to-access lesions.
In recent years, due to its predominantly osteolytic characteristics and its abundance of multinucleated giant cells resembling osteoclasts, Denosumab has been studied for the treatment of ABC. This medication works by blocking the RANKL receptor, thereby reducing osteoclast activation.^ 19 ^ However, studies still do not present a consensus regarding the appropriate dose and duration of treatment. In the present study, the recurrence rate of ABC was 30.4%. By treatment modality, we observed a recurrence rate of 33.4% in patients who received a single treatment (either surgery or infiltration only). In the combined therapy, we observed a 20% recurrence. Moreover, we found no association between recurrence rates and sex, age, or size of the cyst. The recurrence rate after ABC treatment is quite high, in accordance with its aggressive benign nature.
In the literature, recurrence rates after surgical treatment varied from 10 to 59%.^ 20 ^ Vergel de Dios et al.^ 20 ^ reported that 90% of recurrences occurred in patients under 20 years of age, and the authors associated recurrence with younger age. Still, the statistical analysis did not confirm this association.^ 20 ^
CONCLUSION
The observed epidemiology is consistent with pediatric cohorts reported in the literature. Both surgery and calcitonin infiltration are appropriate treatment options for aneurysmal bone cysts, and embolization can be employed concomitantly or independently of these methods to achieve local control of lesions in surgically difficult-to-access locations. There was no statistically significant relationship between recurrence and the evaluated risk factors, as the value 1.0 was always within the Prevalence Ratio interval.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jaffe HL Lichtenstein L Solitary unicameral bone cyst: With emphasis on the roentgen picture, the pathologic appearance and the pathogenesis Arch Surg 1942441004102510.1001/archsurg.1942.01210240043003 · doi ↗
- 2WHO Classification of Tumours Editorial Board Soft tissue and bone tumours 5th ed.Lyon International Agency for Research on Cancer 2020
- 3Ramírez AR Stanton RP Aneurysmal bone cyst in 29 children J Pediatr Orthop 200222453353912131454 · pubmed ↗
- 4Chan G Arkader A Kleposki R Dormans JP Case report: primary aneurysmal bone cyst of the epiphysis Clin Orthop Relat Res 201046841168117210.1007/s 11999-010-1228-520107940 PMC 2835586 · doi ↗ · pubmed ↗
- 5Song KS Lee SW Bae KC Sohn ES 3rd Aneurysmal bone cyst involving the metacarpal bone in a child Am J Orthop (Belle Mead NJ)2015443 E 68E 7025750953 · pubmed ↗
- 6Iltar S Alemdaroğlu KB Karalezli N Irgit K Caydere M Aydoğan NH A case of an aneurysmal bone cyst of a metatarsal: review of the differential diagnosis and treatment options J Foot Ankle Surg 2009481747910.1053/j.jfas.2008.10.00119110164 · doi ↗ · pubmed ↗
- 7Dhamangaonkar AC Sathe A Banerjee S An Unusual Case of Aneurysmal Bone Cyst of Proximal Phalanx in a 2 Year Old Child J Hand Surg Asian Pac Vol 202025111411810.1142/S 242483552072002932000601 · doi ↗ · pubmed ↗
- 8Boriani S Lo SF Puvanesarajah V Fisher CG Varga PP Rhines LD Aneurysmal bone cysts of the spine: treatment options and considerations J Neurooncol 2014120117117810.1007/s 11060-014-1540-025059450 · doi ↗ · pubmed ↗