Multifactorial conceptual model of cancer-related accelerated aging
Lisa Morse, Sandra Weiss, Christine S. Ritchie, Melisa L. Wong, Thomas Hoffmann, Margaret Wallhagen, Christine Miaskowski

TL;DR
This paper introduces a model explaining how cancer can speed up aging, affecting patients' health and quality of life.
Contribution
The paper presents a new conceptual model linking cancer with accelerated aging through multiple interrelated factors.
Findings
The model integrates six concepts to explain cancer-related aging.
It can help identify patients at risk and guide personalized treatment.
The model is based on Life Course Theory and empirical evidence.
Abstract
Evidence suggests that cancer-related accelerated aging contributes to an earlier onset of chronic diseases; persistent symptoms; and decrements in patients’ quality of life. This review presents the Multifactorial Model of Cancer-related Accelerated Aging (MMCRAA), a conceptual framework that is grounded in Life Course Theory and supported by empiric evidence. The model includes six inter-related concepts: person, behavioral, biological, treatment, symptom, and life course factors. The MMCRAA can be used by clinicians and researchers to identify patients at increased risk for cancer-related accelerated aging; guide personalized treatment planning; and inform the development of interventions and research.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
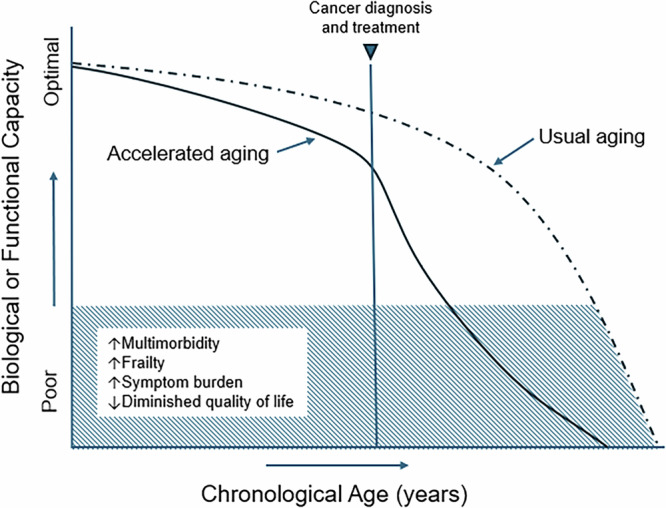 Figure 1
Figure 1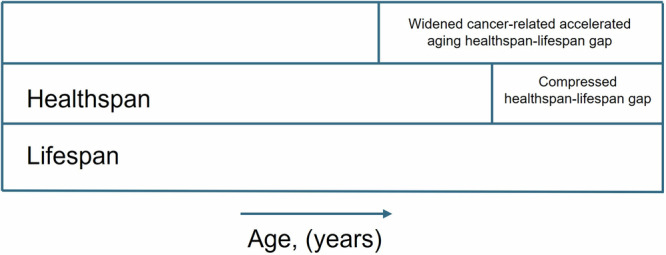 Figure 2
Figure 2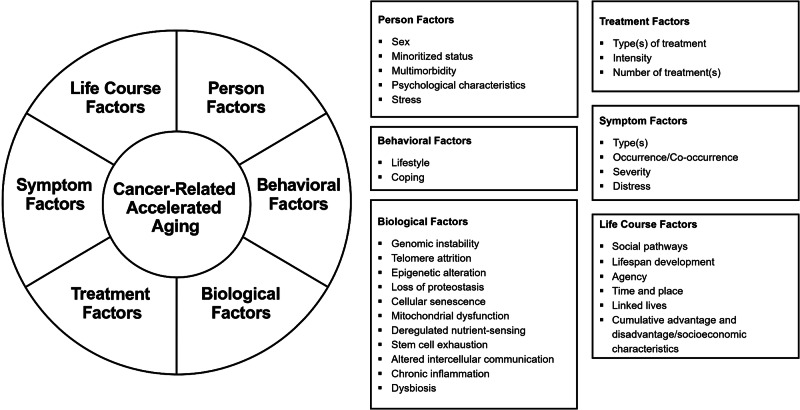 Figure 3
Figure 3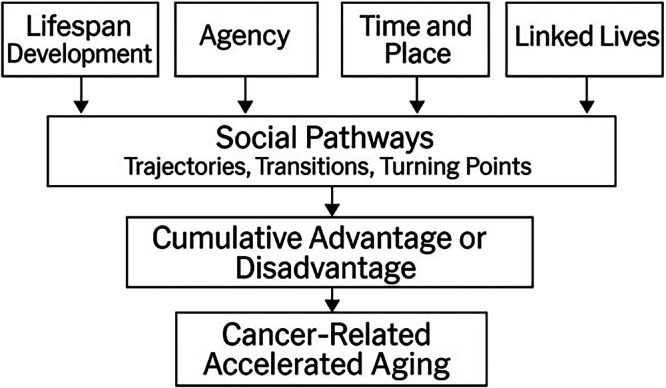 Figure 4
Figure 4- —Department of Veterans Affairs, Veterans Health Administration, Office of Academic Affiliations VA Quality Scholars Advanced Fellowship Program
- —University of California, San Francisco, School of Nursing graduate fellowship
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer survivorship and care · Frailty in Older Adults · Cancer-related cognitive impairment studies
Introduction
While advances in cancer detection and treatment have led to reductions in cancer mortality^1^, these increases in life expectancy can be accompanied by an earlier onset of chronic disease^2^, persistent unrelieved symptoms^3^, and diminished quality of life^4^. For example, compared to the general population, some patients with cancer experience an earlier onset of multi-morbidity^2,5–7^, frailty^8^, cognitive impairment^9^, and functional decline^10^. A growing body of evidence suggests that cancer-related accelerated aging contributes to these health burdens^11–13^.
Accelerated aging is characterized by physiological (i.e., reduced ability to maintain homeostasis) and/or functional decline that occurs earlier than expected for a patient’s chronological age^14^. Estimates of biological or functional age, terms often used interchangeably, compare a patient’s biological parameter(s) or clinical assessment(s) to norms for the general population at a specific chronological age. Patients with a biological or functional age that exceeds their chronological age are considered to be accelerated in their aging (see Fig. 1). While correlated with chronological age, estimates of biological and/or functional age more accurately predict inter-individual variability in the severity of functional decline, increased risk for mortality, and the occurrence of diseases associated with aging^15^.Fig. 1. Hypothesized aging trajectories in patients with cancer receiving treatment.This figure depicts the relationship between biological or functional capacity and chronological age in individuals experiencing usual versus accelerated aging. The solid line illustrates an accelerated aging trajectory, marked by an earlier onset and longer duration of health burdens such as multimorbidity, frailty, persistent symptoms, and reduced quality of life. In addition, depending on various early life exposures and genetic risk factors, the accelerated aging trajectory may be present before cancer diagnosis and treatment. The dashed line represents a usual aging trajectory, with a shorter period of health decline occurring closer to the end of life. (Adapted from Guida et al.).
Compression of morbidity is a concept that refers to extending the amount of time in good health (i.e., healthspan) by delaying the time spent in poor health to a shorter duration at the end of life^16^. As shown in Fig. 2, cancer-related accelerated aging appears to widen the gap between the healthspan and lifespan. In fact, depending on various multifactorial factors (e.g., sociodemographic context^17^, chronological age^18^), patients with cancer can lose between 13 and 17 years of quality-adjusted life years due to their illness^19^. Importantly, the global burden of cancer is growing^17^. As the number of cancer survivors in the United States continues to increase^20^, the identification of risk factors associated with cancer-related accelerated aging is essential to be able to compress morbidity, improve quality of life, and prevent the earlier onset of poor health outcomes in these individuals.Fig. 2. The healthspan lifespan gap in patients with cancer.The figure represents a widened or compressed healthspan lifespan gap in patients with cancer and survivors of cancer. The healthspan is the number of years lived in good health. The lifespan is the total number of years lived. The healthspan-lifespan gap is characterized by the presence of chronic conditions, persistent unrelieved symptoms, and poorer quality of life. Cancer-related accelerated aging is hypothesized to widen the gap between the healthspan and lifespan.
The identification of risk factors associated with cancer-related accelerated aging is hindered by several methodological and conceptual issues. In terms of methodological constraints, existing measures used to estimate biological and/or functional age require refinements^21,22^. In fact, no gold standard exists to estimate accelerated aging. As a result, various approaches are used across studies, making it difficult to compare and contrast findings^21,23^.
In terms of conceptual challenges, while clinical manifestations of accelerated aging in the general population have been described^21^, the cancer-related accelerated aging phenotype is not well characterized. For example, an interdisciplinary panel of experts proposed six clinical signs and symptoms (i.e., fatigue, poor sleep, depressed mood, lack of motivation, subjective memory complaints, poor exercise tolerance) that occur as a result of the biological mechanisms associated with cellular decline and accelerated aging in the general population^21^. However, in patients with cancer, distinct signs and symptoms warrant consideration. For example, the presence of frailty^24^ (i.e., sarcopenia, weakness, slow walking speed, low energy, fatigue, and exhaustion) and cancer-related symptoms (i.e., fatigue^25,26^, pain^26^, sleep disturbance^26^, peripheral neuropathy^27^, cognitive changes^26^, depression^26^, and anxiety^26^) are associated with accelerated aging. Without a clearly defined cancer-related accelerated aging phenotype, salient risk factors associated with its occurrence are not available to researchers and clinicians.
An equally challenging conceptual issue is the establishment of a standard for healthy aging. Most of the current approaches to determine usual versus pathologic aging take physiologic (e.g., inflammatory markers), omic (e.g., Deoxyribonucleic Acid (i.e., DNA) methylation), or deficit (e.g., number of comorbidities, functional decline) perspectives^15^. However, findings from studies of older adults suggest that healthy aging encompasses more than not having a certain number of accumulated chronic conditions. For example, older adults may self-report that they are “aging successfully” despite having chronic medical conditions or physical disability^28,29^. In contrast, poorer self-rated health is associated with increased accelerated aging^30,31^. Equally important, as noted in a review on the domains and measurements of healthy aging^32^, physiological wellness and social engagement are common standards by which healthy aging is assessed. Currently, research on the relationships between/among these various domains and cancer-related accelerated aging is limited.
Several theories of aging propose the mechanisms and factors that influence the heterogeneity in aging phenotypes among the general population. These aging theories primarily fall into programmed or non-programmed categories. According to the programmed theories (e.g., Gene Regulation Theory^33^, Cellular Senescence Telomere Theory^34–36^), the pace of aging depends on pre-programmed biological clocks that regulate human development through distinct stages (i.e., differentiation, growth, maturity, senescence). Non-programmed theories of aging (e.g., Mutation Accumulation Theory^37^, Error Catastrophe Theory^38^, Disposable Soma Theory^39^, and Free Radical Theory^40^) propose that aging is a consequence of unrepaired cellular damage and/or somatic mutations that accumulate from physiological wear and tear over time. Cellular and/or genetic damage that accumulates over time is thought to eventually exceed the body’s capacity to self-repair, leading to an increased risk for functional decline, chronic illnesses, and mortality^41^. Given the known genotoxic and cytotoxic effects of many cancer therapies, as well as the shared processes between aging and those that enable tumorigenesis (i.e., hallmarks of cancer^42^), cancer and its treatment(s) may act synergistically with biological processes involved in aging (i.e., hallmarks of aging^43^) to accelerate biological aging, increase vulnerability to age-related comorbidities, and exacerbate functional decline in patients with cancer.
In recent years, aging is understood to be a process that is shaped by numerous interrelated intrinsic, extrinsic, and stochastic factors that operate across various levels of biological organization^44^. This perspective has underpinnings in the Life Course Theory^45^, which conceptualizes human development as a lifelong process that is influenced by biological, psychological, and social factors. Building on the tenants of the Life Course Theory^45^, the Social Hallmarks of Aging framework suggests that social causes (e.g., low lifetime socioeconomic status, adversity in childhood and adulthood, being a member of a minority group, adverse health behaviors, adverse psychological states) contribute to inter-individual variability in age-related health outcomes^46^. Moreover, the weathering hypothesis offers a related explanation, proposing that an earlier onset of health deterioration results from the cumulative impact of repeated exposures to social and economic adversity and political marginalization^47^. These theories and associated hypothesis are supported by empiric evidence that suggests that demographic^48^, environmental^49^, behavioral^48^, and psychosocial^50^ factors play a role in driving molecular processes that result in accelerated aging phenotypes in patients with cancer.
Considering the breadth of the theoretical and empiric work done to date, cancer-related accelerated aging is likely to be a multifactorial process. A comprehensive model that includes the various determinants of cancer-related accelerated aging across the lifespan is needed to understand the broad range of potential risk factors and mechanisms that underlie variations in oncology patients’ age trajectories. An increased understanding of the determinants of cancer-related accelerated aging will provide directions for future research that aims to identify risk factors and their relative contribution to age-related health outcomes so that effective interventions can be developed and tested to prevent or treat cancer-related accelerated aging.
Previously, Carroll and colleagues proposed the model of biobehavioral modifiers of cancer and accelerated aging^51^. This model highlights the importance of considering treatment exposures and psychosocial and behavioral risk factors in research and clinical interventions aimed at inhibiting the acceleration of biological mechanisms associated with aging and cancer. While informative, this model is limited to modifiable patient-level behaviors (i.e., psychosocial stress, sleep quality, physical activity, weight management, and substance use). Given that patients with cancer live and interact within a broader historic and sociogeographic context, and evidence supports that these factors influence aging trajectories^49,52^, a more comprehensive model that includes a life course perspective is needed. In addition, including non-modifiable risk factors is important so that they can be accounted for when determining the relationships between and among risk factors related to cancer-related accelerated aging.
A life course perspective emphasizes that human development and aging are lifelong processes and that early-life conditions and experiences can have latent effects on health^53,54^. It highlights how life trajectories are shaped by individual choices, structural opportunities and constraints, and the historical time and place in which a person lives^55^. While Manelblatt and colleagues developed a framework that applies a life course perspective to biological aging in patients with cancer^56^, their model lacks these life course constructs.
Therefore, the purpose of this paper is to present the Multifactorial Model of Cancer-related Accelerated Aging (MMCRAA), a conceptual framework that is grounded in theory and supported by empiric evidence. A conceptual framework provides an orienting scheme that illustrates the relationships between and among concepts and a phenomenon of interest. The MMCRAA can inform future research by identifying key risk factors and their relationships with one or more health outcomes^57,58^.
Model development
Literature review
The MMCRAA was developed based on a literature review of the factors associated with cancer-related accelerated aging. The search was conducted in PubMed and Google Scholar using the following keywords and/or phrases: accelerated aging OR biological aging AND cancer OR oncology. The reference list of included studies was searched by hand to identify additional relevant studies. Given the paucity of studies on accelerated aging in patients with cancer, the literature review was expanded to include studies of the general population.
Conceptual organization of the MMCRAA
Once the factors associated with accelerated aging in patients with cancer were identified, they were organized into broader concepts. A concept represents a set of similar attributes and/or characteristics associated with the phenomenon of interest^57^. As illustrated in Fig. 3, cancer-related accelerated aging is the main construct, represented by the innermost circle in the model. Surrounding this central core is a concentric circle that is partitioned into several sections. Each section represents a distinct concept. The concepts are hypothesized to interact and contribute to cancer-related accelerated aging through complex multi-level pathways that may be unidirectional, bidirectional, or moderated. In addition, the relationships between/among the concepts are dynamic, shifting over time and across contexts to influence the aging process. The MMCRAA includes six key concepts: person factors, behavioral factors, biological factors, treatment factors, symptom factors, and life course factors. The evidence to support the association between each of these concepts and variations in accelerated aging in patients with cancer is synthesized and briefly described.Fig. 3. Multifactorial model of cancer-related accelerated aging.Cancer-related accelerated aging is the main construct, represented by the innermost circle in the model. Surrounding this central core is a concentric circle that is partitioned into several sections. Each section represents a distinct concept. The concepts are hypothesized to interact and contribute to cancer-related accelerated aging through complex multi-level pathways that may be unidirectional, bidirectional, or moderated.
Assumptions of the MMCRAA
The underlying assumptions of the model are: (1) human development is a lifelong process influenced by biological, psychological, and social factors; (2) the heterogeneity in the health outcomes of oncology patients with the same chronological age reflects differences in their biological/functional age; and (3) the causes and consequences of cancer-related accelerated aging are multifactorial.
Operational definition of cancer-related accelerated aging
An operational definition describes the procedures and/or outcome(s) that measure a construct^57^. Aging is a universal phenomenon defined as a time-dependent decline in functional capacity and the ability to engage in allostasis or maintain homeostasis^43,59^. Cancer-related accelerated aging refers to a faster rate of decline, such that, compared to the general population, oncology patients exhibit health outcomes associated with aging earlier than expected^60^.
Accelerated aging is operationalized using either clinical measures that estimate functional age (e.g., activities of daily living^61^, Karnofsky Performance Status scale^62^, Functional Assessment of Cancer Therapy–Cognitive)^63^, Deficit Accumulation Index (DAI)^64^, Frailty Index^65^) or biomarkers of aging (e.g., epigenetic clocks^66^, inflammatory markers^67^, proteomic aging clock^68^, neuroimaging^69^) to estimate biological age^23^. Changes in these biological and functional measures correlate with mortality and age-related outcomes in oncology patients and capture inter-individual variability in the underlying biological processes (i.e., hallmarks of aging) associated with aging^70,71^.
Model components
In the sections that follow, the rationale for the inclusion of each of the concepts in the MMCRAA is briefly summarized. For each of the concepts, specific components within the concepts are illustrated in boxes in Fig. 3.
Person factors
Oncology patients come to the cancer experience with a unique set of underlying attributes that impact how they respond to their treatment and influence their risk for accelerated aging. Person factors included in the MMCRAA are sex, minoritized status, multimorbidity, psychological traits, and stress.
Sex
Evidence suggests that compared to men, women have a longer life expectancy^72,73^. These findings may be related to sex differences in their rate of aging. For example, in a meta-analysis^49^, male sex was associated with increased biologic age estimated using epigenetic clocks trained to predict chronological age (i.e., Hannum, Horvath). However, compared to men, women have a higher prevalence of frailty^74^ and are more likely to experience adverse effects^75^ and a higher symptom burden^76,77^ from their cancer treatment. The resulting male-female health-survival paradox^78^, may be related to sex-chromosomal linked mechanisms^73^, sex-hormonal effects^73^, differences in lifestyles^79^, and/or the biological processes that underlie aging^73,80^. Given the evidence for sex differences in biological aging and health outcomes associated with aging and cancer treatment, it is important that differences in sex are examined when evaluating the relationships between various risk factors and cancer-related accelerated aging.
Minoritized status
Minoritized status refers to a patient belonging to a group that holds less social, political, or economic power compared to the dominant or majority group^81^. Minoritized status is related to various characteristics, including race and ethnicity, religion, immigration status, language, sexual orientation, gender identity, disability status, and age. Perceived discrimination based on these characteristics is associated with increased psychosocial stress^82^ and accelerated biological aging. For example, in a study that used growth mixture modeling to characterize distinct subgroups of African American adolescents based on their level of perceived discrimination^83^, membership in the high and stable discrimination group was associated with a higher epigenetic age. Of note, for every one-unit increase in perceived discrimination score, epigenetic age increased by 1.5 years. The authors suggested that repeated experiences of discrimination were likely to trigger the activation of stress response systems.
Studies that evaluated the relationship between discrimination based on minoritized status characteristics and accelerated aging among patients with cancer are limited. In one study that evaluated the relationship between discrimination and the DAI score in African American patients with cancer^84^, as the number of discriminatory events increased, the DAI score increased. These findings suggest that a higher level of perceived discrimination is associated with frailty, a key phenotype of aging.
Given that cancer-related accelerated aging is associated with an earlier onset of functional and cognitive decline and sensory impairment, discrimination based on disability (i.e., ableism) is likely to contribute to increases in both stress and accelerated aging. Evidence to support this hypothesis comes from a national poll that found that adults with disabilities were more likely to report that discrimination was a somewhat or significant source of their stress^82^. Since research that examines the effects of discrimination on biological aging among patients with cancer is limited to one study of African American race^84^, additional studies are needed to validate these findings and evaluate other minoritized characteristics. In addition, studies are needed that evaluate whether multiple intersecting minoritized characteristics contribute to increased psychosocial stress and accelerated aging among patients with cancer.
Multimorbidity
In the general population, having a greater number of chronic illnesses is associated with increased accelerated biological aging^85^. For example, for every 7-year increase in the Levine epigenetic clock^85^, the rate of multimorbidity accumulation increased by 6%. In addition, as reported in a meta-analysis^49^, having a higher body mass index, a mental health illness (i.e., depression, schizophrenia), and/or a diagnosis of diabetes, chronic obstructive pulmonary disease, or cardiovascular disease were associated with increased biological age estimated using one or more epigenetic clocks.
While studies demonstrate that a greater number of chronic conditions is associated with increased biological aging in the general population, less is known about these relationships in patients with cancer. In one study that dichotomized patients based on their history of any cancer^48^, a dose-response relationship was observed between increases in the number of co-morbidities and increases in biological aging in both groups, regardless of cancer history. In another study that examined whether biologic age acceleration was associated with an increased risk of developing a chronic health condition over time^27^, compared to patients with cancer in the lowest tertile of biologic age acceleration, patients in the highest tertile had an increased risk of developing hypertension, obesity, myocardial infarction, lung disease, and/or peripheral motor neuropathy. Additional research is needed to determine whether the presence of specific chronic conditions and/or the accumulation of comorbidities as a result of cancer and its treatment increases cancer-related accelerated aging. This research is important because multimorbidity may predispose oncology patients to an accelerated aging trajectory.
Psychological characteristics
Psychological characteristics, such as an oncology patient’s level of resilience, perception of well-being, self-perceived health, and personality traits (e.g., conscientiousness, neuroticism), can alleviate or exacerbate stress^86^, inflammatory^87^, and/or multi-omic^88^ mechanisms that contribute to aging. In addition, these moderators influence health behaviors (e.g., smoking, diet) that affect aging^89^.
Psychological resilience
Psychological resilience is the ability to adapt to adversity, maintain emotional stability, and thrive in response to difficult or challenging circumstances^90^. In the general population, higher psychological resilience is associated with greater longevity^91^ and slower epigenetic age acceleration^92^. For example, in a study of the general population^86^, higher levels of resilience-related factors (i.e., emotional regulation, self-control) moderated the relationship between higher cumulative stress and increased accelerated biological aging estimated using the GrimAge epigenetic clock. In a study of oncology patients^93^, a decrease in biologic age was significantly correlated with an increase in resilience scores after the completion of a 12-week exercise program. These studies provide some evidence to suggest a relationship between resilience and biological aging. In addition, since lower psychological resilience is associated with higher symptom severity scores and higher cancer-related distress in patients with cancer^94^, resilience may moderate the relationship between symptom severity and distress in patients with cancer and influence cancer-related accelerated aging.
Psychological well-being
Psychological well-being encompasses dimensions that describe an individual’s overall level of emotional functioning (e.g., autonomy, environmental mastery, personal growth, purpose in life, and self-acceptance)^95^. In a study of older adults that evaluated the relationships between dimensions of well-being and aging^96^, higher purpose in life was associated with reduced biologic age using four epigenetic clocks (i.e., PhenoAge, GrimAge, Zhang, and Dunedin PoAm). In another study of the general population^97^, among individuals with lower psychological well-being, higher cumulative life stress was associated with increased biological age estimated using the GrimAge2 epigenetic clock. In addition, among individuals with higher psychological well-being, higher levels of cumulative stress did not affect their biological aging. Therefore, because the effect of stress on biological aging may be influenced by perceptions of psychological well-being, these relationships warrant evaluation in patients with cancer.
Self-perceived health
Self-perceived health is a patient’s assessment of their overall health and is associated with mortality^98^, psychological well-being^99^, objective measures of physical function^100^, and mechanisms associated with aging (i.e., inflammation)^101^. Because perceived health reflects indicators of health (e.g., physical conditions, emotional states, and symptoms) that are meaningful to an individual^102^, it may reflect aspects of health that are not routinely captured by standard clinical assessments. Discrepancies between oncology patients’ expectations of and perceived declines in health indicators that they deem meaningful may increase stress and negatively impact aging-related outcomes.
A limited body of research evaluated the relationships between self-perceived health and biological aging^30,31,48,103^. For example, in a study of patients with cancer^31^, lower self-reported physical health was associated with accelerated aging estimated using a proteomic aging clock. For every 5-year increase in biological age, self-reported physical health decreased by nearly two points. In another study of the general population^30^, compared to individuals who rated their health as excellent, those who rated their health as poor had a significantly faster pace of biological aging estimated by the DunedinPACE clock. Additional studies are needed to determine whether poor self-perceived health contributes to cancer-related accelerated aging.
Personality traits
A large body of research identified specific personality traits associated with poorer health outcomes (i.e., cardiovascular disease, diabetes^104^) and increased mortality risk^105,106^. As noted in a meta-analysis^105^, individuals with scores in the lowest tertile for the conscientiousness personality trait (i.e., low persistence, poor self-control, poor long-term planning) had a 37% increased risk of death compared to those in the top two tertiles. This finding suggests that lower levels of the conscientiousness personality trait may increase the risk for accelerated aging.
Limited evidence suggests that personality traits may influence the aging process by mediating the negative health effects of stress. For example, in a study of the general population^86^, higher cumulative life stress was associated with increased biological age in individuals with higher levels of neuroticism (i.e., the predisposition to experience negative emotions such as anxiety, sadness, worry, and anger). This finding suggests that higher levels of neuroticism contribute to increased vulnerability to the pathologic aging effects of stress. Future studies should evaluate the mediating/moderating effects of personality traits on the relationships between stress and aging in patients with cancer.
Stress
The relationship between increased levels of psychological stress and the biological mechanisms associated with aging was reviewed extensively^107–111^. Psychological stress refers to the emotional strain or pressure that results from a stressor(s), namely: an experience that an individual perceives as challenging, threatening, or overwhelming. Exposure to a stressor(s) that exceeds an individual’s ability to adapt activates the sympathetic nervous system, inflammatory pathways, and stress axes (e.g., hypothalamic pituitary adrenal axis, sympathetic-adreno-medullary axis) and results in elevated levels of catecholamines, proinflammatory cytokines, and glucocorticoids. These hormones can influence the rate of aging through alterations in epigenetic regulation and chronic inflammation^112^.
A growing body of research demonstrates an association between increased levels of stress and accelerated biological aging in the general population. For example, findings across studies suggest that experiencing stress related to a traumatic event(s) is associated with accelerated biological aging^113–116^. In addition, a diagnosis of post-traumatic stress syndrome is associated with accelerated biological aging^117^. Given that a cancer diagnosis is often a traumatic event in a person’s life and that cancer-related stress can reach the threshold for post-traumatic stress syndrome^118^, an examination of the relationship between stress and accelerated aging in patients with cancer is warranted.
Behavioral factors
Lifestyle
The association between lifestyle behaviors (e.g., poor dietary nutrient intake^71,119,120^, smoking^49,121^, physical inactivity^71^) and accelerated aging is well supported by studies of the general population. However, the evidence linking lifestyle behaviors and accelerated aging in patients with cancer is limited. For example, in one study of oncology patients that evaluated the relationship between five suboptimal health behaviors (i.e., low physical activity, low weight bearing activity, smoking, lack of adherence with a healthy diet, risky drinking) and accelerated aging^27^, compared with cancer survivors with favorable health behaviors, among those with intermediate or unfavorable health behaviors, biologic age was significantly higher. In another study of oncology patients^122^, compared to never smokers, having a history of tobacco use and fewer smoking cessation years was associated with a higher biologic age. Smoking is associated with predictable changes in DNA methylation patterns consistent with accelerated aging^123^. Additional research is needed to validate these findings and investigate interventions aimed at improving lifestyle behaviors and their effect on cancer-related accelerated aging.
Coping
Coping strategies are the cognitive, emotional, and/or behavioral efforts that individuals use to respond to and adapt to stress. Coping strategies can be categorized as either engagement or disengagement behaviors. In oncology patients, compared to engagement coping, disengagement coping was associated with a higher symptom burden^124^ and higher levels of stress^125^. While no studies evaluated the relationships between differences in coping behaviors and cancer-related accelerated aging, in a study of African Americans who experienced racial discrimination, compared to individuals who sought social support (i.e., an engagement type coping behavior)^126^, individuals who did not seek out social support were biologically older estimated using an epigenetic clock. In addition, greater use of social support mitigated the effects of discrimination on accelerated aging. Additional research is needed to evaluate the relationships between various types of engagement and disengagement coping behaviors and cancer-related accelerated aging.
Biological factors
Evidence from animal and human studies identified twelve interrelated biological processes, known as the hallmarks of aging (i.e., genomic instability, telomere attrition, epigenetic alterations, loss of proteostasis, disabled macroautophagy, deregulated nutrient-sensing, mitochondrial dysfunction, cellular senescence, stem cell exhaustion, altered intercellular communication, chronic inflammation, dysbiosis)^43^, that underlie pathological aging. Findings from these studies suggest that when these processes are perturbed or alleviated by experimental interventions^127–129^, they influence the trajectory of aging. Several of the hallmarks of aging are implicated in cancer development and progression^42,130^ and biological markers of their occurrence are observed at disproportionately higher rates in patients receiving cytotoxic treatments^11,131,132^. Therefore, the hallmarks of aging may interact synergistically with the mechanisms that promote tumorigenesis (i.e., hallmarks of cancer^130^) and the pharmacokinetic pathways through which cancer treatments exert their effect(s) to accelerate aging.
The twelve hallmarks of aging and their relationship with cancer were extensively reviewed^133,134^. In the sections that follow, as described previously^43^, each hallmark of aging is categorized as a primary, antagonistic, or integrative factor. Its relationship to accelerated aging is briefly discussed, either in the context of oncology or, when evidence is lacking, in findings from the general population.
Primary hallmarks
The primary hallmarks, that include genomic instability, telomere attrition, epigenetic alterations, loss of proteostasis, and loss of macroautophagy, arise from a decline in the efficiency of repair mechanisms and the accumulation of damage caused by various internal and external stressors over time^43^.
Genomic instability
Genomic instability refers to a broad range of insults to the structural integrity of genetic material^135^. Genomic instability is a hallmark of both aging^135,136^ and cancer^42,130^. Specifically, DNA damage (e.g., strand breaks, crosslinks) and somatic mutations play distinct roles in aging and cancer. DNA damage represents physicochemical alterations to the DNA molecule. Somatic mutations are stable sequence changes that often arise from replication errors from damaged DNA. While mutations are central to cancer development^137^, persistent DNA damage and transcriptional dysregulation are emerging as primary mechanistic contributors to aging^138,139^.
With advancing age, DNA damage accumulates, resulting in less efficient repair mechanisms, replication errors, and reduced transcriptional output^43,138,139^. This transcriptional suppression effects diverse cellular processes and contributes to multiple hallmarks of aging^138,139^. For example, inherited defects in genomic repair mechanisms are associated with premature aging syndromes (e.g., Werner syndrome^140^, Cockayne syndrome^141^). In addition, mutations arising from errors in the repair process of DNA lesions result in permanent changes to the DNA sequence that contribute to oncogenesis by activating proto-oncogenes, inactivating tumor suppressors, and enabling uncontrolled cell proliferation^42,130^.
In addition, the contribution of DNA damage to aging is reflected in the mechanisms of many cancer treatments. For example, alkylating agents (e.g., cyclophosphamide), commonly used to treat a variety of cancers, inhibit cell division by inducing cross-links between guanine bases on DNA strands^142^. Another class of drugs, poly ADP-ribose polymerase inhibitors^143^, block enzymes involved in DNA repair processes.
Telomere attrition
Telomeres, protective caps at the end of chromosomes, progressively shorten with each cell division^144^. Upon reaching a critically reduced length, telomeres trigger cellular responses that lead to apoptosis or cell cycle arrest^144^. Genetic defects that result in the reduction of telomerase, an enzyme that maintains the structural integrity of telomeres, are associated with cancer and degenerative diseases (e.g., Dyskeratosis congenita)^145^.
As noted in one review^146^, the relationships between cancer treatments and changes in telomere length are inconsistent. The authors concluded that the reasons for these inconsistent findings may be related to differences in cancer types and treatment(s). For example, mitotic inhibitors (e.g., taxanes^147^) may cause telomere deprotection (i.e., uncapping) while hematopoietic growth factors (e.g., granulocyte colony-stimulating factor^148^) may upregulate telomerase and result in telomere elongation. In addition, the upregulation of telomerase is one way that cancer cells evade mortality^42^, and the amount of telomerase upregulation varies by cancer type. For example, telomerase reverse transcriptase gene promoter mutations are most common among patients with bladder cancer and least common among patients with colorectal cancer^149^. Equally important, because changes in telomere length are associated with lifestyle factors (e.g., exercise, diet) and stress^150^, these factors may contribute to variations in telomere length among oncology patients. While findings regarding the effects of cancer treatment on telomere length are inconclusive, telomere attrition appears to be a risk factor for accelerated aging^151^.
Epigenetic modifications
Epigenetic modifications (i.e., DNA methylation, histone modification, chromatin remodeling, non-coding ribonucleic acid (i.e., RNA) dysfunction) contribute to genomic instability, and these alterations are observed in both aging^43^ and cancer^130^. For example, increasing age is associated with global hypomethylation, loss of heterochromatin, and changes in histone acetylation and microRNA expression^43^. These epigenetic alterations contribute to the transcriptional silencing of genes involved in DNA repair and maintenance, as well as the upregulation of genes involved in proinflammatory pathways^43^. In addition, variations in the epigenome are associated with external factors (e.g., toxins, diet, exercise, substance use, and stress)^152^.
While evidence from epigenome-wide association studies suggests predictable patterns of epigenetic modification across the lifespan^43,152^, changes in DNA methylation patterns are the most widely studied and predictive of chronologic age^60,153^, mortality^154^, and aging phenotypes^71^. Epigenetic clocks estimate biological age using DNA methylation patterns^66^. These estimates are correlated with cancer risk and survival^155^, mortality^156^, and diseases associated with aging^157,158^. In addition, studies of oncology patients demonstrate that epigenetic age increases from pre- to post-treatment^25,122,159,160^.
Loss of proteostasis and macroautophagy
Loss of proteostasis (i.e., the mechanisms by which proteins are stabilized or degraded)^161^ and loss of macroautophagy (i.e., the processes by which cells break down and recycle damaged cellular material)^162^ are associated with advancing chronological age^162^ and neurodegenerative conditions associated with aging (e.g., Alzheimer’s disease^162^). In addition, cancer cells^163^ and cancer treatments^164,165^ disrupt protein folding homeostasis by inducing genomic instability and/or disabling macroautophagy. Loss of these critical processes leads to the accumulation of damaged macromolecules (e.g., misfolded proteins, dysfunctional organelles) and contributes to chronic inflammation^161^. Proteomic aging, estimated using patterns of plasma protein expression to predict biological age^166^, is associated with increased risk for multimorbidity, frailty, and mortality in the general population^68^. In addition, in a study of oncology patients^166^, a one standard deviation increase in proteomic aging was associated with a 56% increased risk of all-cause mortality.
Antagonistic hallmarks
The antagonistic hallmarks are the systemic consequences of the primary hallmarks and include cellular senescence, mitochondrial dysfunction, and deregulated nutrient-sensing.
Cellular senescence
Cellular senescence is a permanent state of cell cycle arrest that can be triggered by the primary factors^43^. Senescent cells remain metabolically active and secrete proinflammatory cytokines, chemokines, extracellular matrix fragments, and degrading enzymes, described as the senescence-associated secretory phenotype (i.e., SASP)^167^. SASPs can induce senescence in surrounding cells^168^. A large body of research demonstrates that the p16 cyclin-dependent kinase inhibitor 2 A protein (i.e., p16 INK4a), a biological marker of cellular senescence, increases with increasing chronological age^169^ and after cancer treatment (e.g., stem cell transplant^170,171^, chemotherapy^170,172,173^). Across these studies, the difference in p16 INK4a expression from pre- to post-treatment levels represented a 14^173^ to 35^172^ year age acceleration.
Deregulated nutrient sensing
Alterations in metabolism, as a result of deregulated nutrient sensing, are implicated in aging^174^ and cancer progression^175,176^. The nutrient-sensing network responds to the availability of nutrients through complex cellular signaling pathways to mediate metabolism (i.e., anabolism, catabolism). Deregulated nutrient sensing is associated with increased epigenetic age in human cells^177^. In addition, pharmaceuticals (e.g., rapamycin, metformin) that inhibit key nutrient-sensing pathways (e.g., Insulin-like Growth Factor 1, mechanistic Target of Rapamycin Complex 1) are associated with a longer lifespan in animal models^174^. In human studies^174^, centenarians were more likely to carry loss-of-function genetic variants in Insulin-like Growth Factor/Insulin signaling nutrient-sensing pathways.
Mitochondrial dysfunction
Similarly, mitochondrial dysfunction is associated with metabolic alterations (e.g., impaired energy production). Dysfunctional mitochondria can result from oxidative stress^178^ and/or the accumulation of mutations in mitochondrial DNA^179^. Damaged mitochondria release increased levels of reactive oxygen species (i.e., ROS)^178^. This increase in the production of ROS disrupts redox homeostasis, resulting in cellular dysfunction and/or cell cycle arrest (i.e., senescence)^180^. Cancer cells produce high levels of ROS due to their rapid proliferation^181^. Many chemotherapeutics (e.g., doxorubicin^182^ cisplatin^183^) exert their anti-neoplastic effects by increasing oxidative stress beyond the cancer cells’ ability to function. In a mouse model^184^, compared to controls, doxorubicin-induced cardiotoxicity was associated with a significant increase in mitochondrial damage and markers of senescence immediately after treatment. In addition, these increased markers of senescence persisted after treatment. Furthermore, a study that compared cardiac function in patients who were and were not exposed to doxorubicin found that exposed patients had changes in cardiac function comparable to older adults^185^.
Integrative hallmarks
The integrative hallmarks (i.e., chronic inflammation, dysbiosis, stem cell exhaustion, altered intercellular communication) refer to the cumulative effects of the primary and antagonistic hallmarks^43^. For example, senescence can be triggered by many of the primary hallmarks^167,186^ and results in a chronic inflammatory state (i.e., inflammaging)^187^. Elevated levels of inflammatory markers (e.g., C-reactive protein, interleukin-6) were observed in oncology patients undergoing radiation^25^ and chemotherapy treatment^188^. These increases were associated with increases in accelerated biological aging^25,188^.
Dysbiosis
Chronic inflammation is further exacerbated by an imbalance or disruption in the composition of the intestinal microbiota (i.e., dysbiosis)^189^, which can be a risk factor for cancer^190^ and can occur as a result of aging^191^ and/or cancer treatment(s)^192^. Cancer treatments can damage the intestinal mucosa, making it more permeable to toxic substances. While direct evidence linking dysbiosis to cancer-related accelerated aging is not available, changes in the composition of intestinal microbiota are associated with frailty^193^, cognitive decline^194,195^, and the hallmarks of aging (i.e., altered nutrient sensing, cellular senescence) in the general population^43^. In addition, emerging evidence suggests that distinct microbiome signatures are correlated with increased accelerated biological aging in the general population^196,197^ and in patients with Human Immunodeficiency Virus^198^.
Stem cell exhaustion
Stem cells are essential for tissue renewal and repair. Aging, chronic inflammation, and genomic instability are associated with a decline in the number and function of stem cells^43^. In contrast, proliferative signaling by oncogenes is associated with stem cell maintenance and tumorigenesis^42^. Cancer treatments contribute to the depletion or dysfunction of hematopoietic stem cells. For example, in a study of patients with hematologic malignancies treated with Cluster of Differentiation 19 Chimeric Antigen Receptor T (i.e., CD19 CAR-T) cells^199^, 16% of patients experienced persistent cytopenias that lasted for at least 1 year after treatment.
Altered cellular communication
Alterations in cellular communication are a consequence of both the hallmarks of aging^43^ and cancer and its treatment(s)^42^. For example, the accumulation of senescent cells and misfolded proteins that occur with increasing age is known to contribute to dysregulated paracrine and autocrine signaling^168^. In addition, cancer cells may evade immune surveillance by altering receptors involved in immune recognition. Emerging immunotherapies (e.g., immune checkpoint inhibitors, CAR T-cell therapy) exploit these alterations to promote active immunity against cancer cells. While effective, immunotherapies are associated with overactivation of the immune system, chronic inflammation, and hematologic toxicity^200^, which may contribute the cancer-related accelerated aging.
Treatment factors
As discussed in the previous section, cancer treatments impact multiple hallmarks of aging through diverse mechanisms. Several factors, such as the type(s), number of treatments (i.e., combination, recurrent), and intensity (i.e., duration, number of cycles, length of time between cycles/treatments) of the treatment regimen(s), contribute to cancer-related accelerated aging.
Type(s)
The aging effects of cancer treatments largely depend on their mechanism(s) of action and adverse effects. Chemotherapy and radiation, due to their nonspecific genotoxic and cytotoxic effects, disrupt nearly all of the hallmarks of aging. These therapies contribute to the accumulation of replicative senescence that results in a chronic inflammatory state (i.e., inflammaging). Similarly, surgical interventions trigger the activation of the inflammatory cascade^123^ and are associated with increases in SAPS^201^. Hormone therapies (e.g., tamoxifen, aromatase inhibitors) may modulate nutrient-sensing networks^202^. Targeted therapies (e.g., kinase inhibitors, monoclonal antibodies) and immunotherapies (e.g., immune checkpoint inhibitors) alter proteostasis, epigenetic regulation, and intracellular signaling networks, which in turn can accelerate aging^203^.
Number of treatment(s)
Many oncology patients receive multiple treatments either in combination, succession, or to treat secondary cancers during the course of their illness. In several studies, the receipt of more than one type of cancer treatment was associated with an increased incidence of severe toxicity^204^, poorer health outcomes (i.e., multimorbidity^205^), and increases in accelerated aging^206^.
Intensity
Most cancer treatments are administered in successive cycles (e.g., chemotherapy) or fractions (e.g., radiation therapy), which consist of a treatment period followed by a rest period. Increased dose intensity (e.g., higher dose, shorter time between rest periods, longer duration of treatment cycles) contributes to an increase in the toxicity of the treatment regimen. For example, cardiotoxicity following anthracycline treatment demonstrates a dose-dependent, stepwise increase in incidence with increasing cumulative exposure^207^. Increased treatment toxicity is hypothesized to increase the risk of cancer-related accelerated aging^131,208^.
Symptom factors
On average, oncology patients report 10^209^ to 15^210^ unrelieved symptoms associated with their cancer and its treatment. Higher symptom burden in oncology patients is associated with increased stress^94^, multimorbidity^211^, functional decline^212^, and decrements in quality of life^213^. Commonly assessed dimensions of the symptom experience include patient-reported levels of severity and distress^214^. Findings from a limited number of studies of patients with cancer report that higher levels of fatigue^25,160^, pain^160^, sleep disturbance^160^, peripheral motor neuropathy^27^, cognitive impairment^160^, depression^160^, and anxiety^160^ were associated with increased biologic aging estimated using epigenetic clocks. In addition, in oncology patients, higher levels of common cancer-related symptoms (e.g., fatigue) were associated with the occurrence of clinical frailty^215^, increased levels of inflammatory markers^25^, and variations in microbiome composition (i.e., dysbiosis)^216^. Symptoms may interact with aging-related biological mechanisms in a way that amplifies or modifies their impact on pathologic aging in patients with cancer. More research is needed to understand how cancer-related symptoms, including how severe or distressing they are, are linked to faster aging caused by cancer.
Importantly, symptoms in patients with cancer often co-occur in clusters^217^. Multiple co-occurring symptoms are associated with increased risk for mortality in patients with cancer^218^. In one study of oncology patients^122^, a higher severity of a head and neck treatment-related symptom cluster was associated with increased biologic aging. Given the paucity of research on associations between symptoms, symptom clusters, and cancer-related age acceleration, additional studies are needed.
In addition to symptoms related to cancer and its treatment, a positive relationship was found between post-traumatic stress symptoms (e.g., intrusive thoughts, avoidance, hypervigilance) and increases in biologic aging in non-cancer cohorts^117,219^. Since a higher symptom burden in patients with cancer is associated with an increased prevalence of post-traumatic stress symptoms, (LM, SW, CR, MW, Cooper, B., Hammer, M., Conley, Y., Steven, P., Levine, J., CM, in review) an evaluation of the relationship between post-traumatic stress symptoms and accelerated biological aging is warranted in patients with cancer.
Life course factors
The Life Course Theory is a multidisciplinary framework that describes how various factors, including individual characteristics, social structures, environmental influences, and historic contexts, interact to shape people’s lives over time^45^. The Life Course Theory evolved from longitudinal studies of childhood development that examined the relationships between experiencing a disruptive societal event (e.g., war, economic downturn) and health and socioeconomic outcomes^45^. These studies revealed that health and aging are influenced by social pathways and several core principles (i.e., lifespan development, human agency, time and place, linked lives). Differences in social pathways contribute to the accumulation of advantages and/or disadvantages over time. As shown in Fig. 4, the Life Course Theory can be applied to oncology research to describe the heterogeneity in aging trajectories observed among patients with cancer.Fig. 4. Application of the Life Course Theory to the Multifactorial Model of Cancer-Related Accelerated Aging.
Social pathways
A social pathway refers to the trajectories and transitions of roles that are followed by groups of people across time. Successful management of life transitions is associated with greater psychological well-being^220^. Social pathways are shaped by social institutions and cultural norms, and expectations. A turning point, such as a cancer diagnosis, is a significant and often stressful life event that contributes to transitions in an oncology patient’s role (e.g., occupational, social, and family). Other significant turning points in oncology patients’ lives are adverse childhood experiences and stressful life events. As noted in several reviews^50,52,221,222^, adverse social exposures across the lifespan result in accelerated aging in the general population. Additional research is warranted that examines the relationships between stressful life events and cancer-related stress on cancer-related accelerated aging.
Lifespan development
The principle of lifespan development emphasizes that people continue to grow, change, and adapt throughout their lives. Each stage of life builds upon prior experiences and impacts future developments. While age-related patterns exist, people can change at any point in life, especially in response to a significant event. For example, transitions, such as becoming a patient and dealing with a cancer diagnosis, affect later stages of life. In addition, some patients may experience poor role functioning as a result of their cancer diagnosis and its treatment. Among oncology patients, poor role functioning (i.e., the inability to fulfill their expected roles in various aspects of life) is associated with increased stress^223^, increased mortality^224^, and decrements in quality of life^223^ and may accelerate aging in oncology patients. Future research is needed that examines the relationship between oncology patients’ role functioning and cancer-related accelerated aging.
Agency
The principle of agency recognizes that, within the opportunities and constraints of their circumstances, individuals make decisions and exert control over their life course trajectory. Agency in oncology patients is exercised through their decision to adhere to or deviate from treatment plans^225^ and/or health-promoting behaviors^226^. In addition, oncology patients may utilize either engagement or disengagement coping strategies to respond and adapt to their cancer diagnosis and treatment^124^. While patients act independently, their decisions, values, and preferences are influenced by their environment and social context^226^. For example, the developmental psychology literature suggests that when individuals are faced with a chronic or uncontrollable stressor(s) (e.g., poverty, violence, and family conflict), they are more likely to use disengagement type coping strategies (e.g., substance use, avoidance, and distraction) because these strategies provide immediate relief from the stressor and/or allow for adaptive functioning within challenging environments^227,228^. While important for survival in certain contexts, disengagement coping is associated with poorer health outcomes^229^ and engagement coping strategies (e.g., seeking support^126^) are protective against accelerated aging.
Time and place
The principle of time and place refers to shifts in the meaning of a life event (i.e., transition, turning point) depending on the developmental stage and social geographic context of the individual^45^. For example, compared to older adults, younger adults experience higher levels of distress as a result of their cancer diagnosis and/or treatment(s)^118,230,231^ and shifts in their role functioning^231^. These differences may be related to changes in emotional regulation^231^, coping^232^, life roles^233^, and psychological resilience^234,235^ across the different developmental stages of life. In terms of self-perceived health, indicators of health that patients deem as meaningful may change over time^236^ and are shaped by previous health experiences^237^ and cultural factors^238^. In addition, evidence suggests that levels of resilience^234^ and coping behaviors^239^ change with age. Therefore, psychological characteristics and behavioral factors may be influenced by the principle of time and place and are hypothesized to contribute to increased cancer-related accelerated aging.
Another aspect of the principle of time is the concept of a critical or sensitive period through which the effects of an event or exposure have an increased impact on a health outcome^240^. In oncology patients, evidence suggests that the rate of accelerated aging varies depending on the chronological age of the patient at the time of their cancer diagnosis. For example, compared to healthy controls^241^, survivors of childhood cancer were estimated to be between 5.2 and 15.9 years older using epigenetic clocks. In another study^242^, compared to healthy controls, older breast cancer survivors were estimated to be between 1.04 and 2.22 years older using epigenetic clocks. Additional research is needed to understand the impact of the timing of the cancer diagnosis, as well as various stressors on accelerated aging trajectories.
Within the principles of time and place, place refers to a patient’s physical, social, and cultural environment. Past injustices experienced by minoritized communities (e.g., discrimination, intergenerational cultural trauma^243^) can affect how patients perceive and respond to their care. Cultural beliefs and values that conflict with the views of the dominant healthcare system can increase psychosocial stress and contribute to poorer health outcomes^244^. In addition, neighborhood characteristics (e.g., social cohesion, exposure to crime) contribute to levels of stress and aging trajectories^245,246^. Additional research is needed to explore the relationships between the principle of time and place and cancer-related accelerated aging.
Linked lives
The principle of linked lives highlights how life course trajectories are interdependent on others within their sociocultural network. For example, patients may rely on the help of an informal (i.e., unpaid) caregiver to assist with their health care needs or to provide emotional support. As noted in two reviews^247,248^, when the responsibilities of caregiving surpass their capacity to cope, being an informal caregiver is associated with poor health outcomes (i.e., depression, multimorbidity, frailty). Importantly, a bidirectional relationship exists between the emotional and physical well-being of informal caregivers and the health outcomes of patients with cancer^249^. For example, oncology patients, whose informal caregiver reported higher levels of depressive symptoms or poorer self-rated health, had an increased odds (i.e., 1.06 and 3.76, respectively) of reporting poorer quality of life^250^. Given that a lower quality of life among oncology patients is associated with a higher risk for mortality^251^ and accelerated aging^122^, the relationship between the patient and informal caregiver is an important focus of future research so that interventions can be developed to support the needs of both of them.
Cumulative advantages and disadvantages
It is well documented that life expectancy and health outcomes vary widely across demographic groups^252^. These disparities are shaped by the conditions into which people are born, live, work and age as well as their access to resources. In addition, differences in how patients adapt to life transitions and turning points, and the timing of these events with respect to their stage of development, contribute to the accumulation of advantages and/or disadvantages over time. For example, having a lower socioeconomic status^49^, lower income^48^, lower educational attainment^48,49,222^, higher neighborhood deprivation^221^, and/or increased exposure to air pollution^49^ were associated with accelerated aging. In a study of oncology patients^48^, those individuals with unmet health-related social needs (e.g., higher food insecurity, lack of insurance coverage) were accelerated in their age estimated using the PhenoAge epigenetic clock.
Life Course Theory posits that these exposures, disparities, and/or experiences become “embodied” or “inscribed” in the physiological processes that influence aging through “chains of risk” ^240^. Chains of risk models describe how an initial event increases the likelihood of a subsequent event(s) and how these accumulated events can either compound disease risk over time or exert independent effects on health^240^.
Future directions for clinical practice and research
The identification of risk factors associated with cancer-related accelerated aging has important implications for clinical practice. The ability to identify patients who are most vulnerable to increased cancer-related accelerated aging can help guide treatment decisions, facilitate discussions about the effects of treatments on life expectancy and quality of life, and inform supportive care strategies. Oncology patients and clinicians can use this information to develop personalized treatment plans that align with the patients’ priorities, such as preserving functional status or extending the healthspan.
As summarized in Table 1, several recommendations for future research should be prioritized. Future research is needed to characterize the cancer-related accelerated aging phenotype using a life course perspective. Importantly, a need exists to develop a consensus on a standardized, valid, and feasible measure of accelerated aging in patients with cancer that can be used in clinical and research settings. In addition, a need exists to create a comprehensive, multidimensional index of cancer-related accelerated aging that integrates person, behavioral, biological, treatment, symptom, and life course factors. Determining the relative contribution of each factor in the MMCRAA will improve the predictive accuracy of tools used to estimate biological aging in oncology populations. Future work must define clinically meaningful changes in accelerated aging and determine how these changes relate to outcomes such as symptom burden, functional decline, and quality of life.Table 1. Recommendations for future research on cancer-related accelerated agingResearch TopicRecommendationConceptual■ Determine the relative contribution of each of the MMCRAA factors in predicting cancer-related accelerated aging.■ Develop a multidimensional composite index of cancer-related accelerated aging that includes a broad range of predictors (i.e., person factors, behavioral factors, biological factors, treatment factors, symptom factors, and life course factors) and validate this index using biologic and functional estimates of aging.Methodological■ Determine the clinically meaningful change associated with increases in cancer-related accelerated aging and differences in symptom burden and quality of life.■ Achieve consensus among clinicians and researchers on which clinical and biological measures are most feasible, reliable, and valid to use to estimate accelerated aging in patients with cancer.Person factorsSex■ Evaluate sex differences in cancer-related accelerated aging.■ Evaluate for differences in underlying sex-linked mechanisms (e.g., sex-chromosomal linked, hormonal) that may contribute to sex differences in cancer-related accelerated aging.Minoritized status■ Evaluate the relationship between discrimination based on diverse minoritized characteristics and cancer-related accelerated aging.■ Determine whether multiple intersecting minoritized characteristics increase stress and impact cancer-related accelerated aging.Multimorbidity■ Evaluate the impact of the various types of chronic conditions and the number of co-morbidities on cancer-related accelerated aging.Psychological characteristics■ Evaluate the role of psychological characteristics (i.e., resilience, well-being, self-perceived health status, personality traits) in mediating/moderating the relationship between cancer-related accelerated aging and other risk factors (e.g., symptoms, stress).■ Investigate the associations between differences in psychological traits (i.e., resilience, well-being, self-perceived health status, personality traits) and the hallmarks of aging.■ Determine whether interventions aimed at enhancing resilience, well-being, and/or self-perceived health status alleviated increases in cancer-related accelerated aging.Stress■ Investigate the relationships among cumulative life stress, traumatic stress, cancer-related stress, and cancer-related accelerated aging.Behavioral factorsLifestyle■ Evaluate the associations between lifestyle behaviors (e.g., diet, activity) and cancer-related accelerated aging.■ Evaluate the effect of interventions aimed at improving lifestyle behaviors on cancer-related accelerated aging.Coping■ Evaluate the relationships between various types of engagement and disengagement coping behaviors and cancer-related accelerated aging.■ Determine whether enhancing the use of engagement type coping behaviors is related to decreases in cancer-related accelerated aging.Biological factors■ Investigate the associations between the hallmarks of aging and MMCRAA factors.■ Determine whether primary, antagonist, or integrative biological factors have a stronger effect on accelerated aging.Treatment factors■ Investigate the relationships between various types of treatment/combination treatments and their impact on cancer-related accelerated aging.■ Evaluate the relationships between treatment intensity and cancer-related accelerated aging.Symptom factors■ Investigate the relationships between symptoms (i.e., cancer-related symptoms, post-traumatic stress symptoms, symptom clusters) and cancer-related accelerated aging.■ Evaluate the impact of different dimensions of the symptom experience (i.e., severity, distress) on cancer-related accelerated aging.Life course factors■ Incorporate variables that measure the principles of human agency and time and place variables in studies that evaluate the relationships between behavioral factors (diet, activity, coping) and psychological traits (resilience, wellbeing, self-perceived health) and cancer-related accelerated aging.■ Incorporate variables that measure the principles of time and place to evaluate the relationships between discrimination based on minoritized status and cancer-related accelerated aging.■ Incorporate variables that measure the principles of time and place to evaluate the relationships between the timing of the cancer diagnosis and/or life stressors on accelerated aging trajectories.■ Incorporate variables that measure the principles of linked lives to evaluate the relationships between informal caregivers’ characteristics (e.g., stress, coping) and oncology patients’ cancer-related accelerated aging.
Conclusion
The MMCRAA provides a holistic framework that can be used by clinicians and researchers to improve personalized cancer care and reduce the deleterious effects of cancer and its treatment on accelerated aging and quality of life. By conceptualizing health as a multidimensional phenomenon, future studies can more accurately identify deviations from expected aging processes in patients with cancer. Advances in characterizing and estimating cancer-related accelerated aging will enable the development of targeted interventions. Incorporating life course principles, such as human agency, time and place, and linked lives, will provide an increased understanding of how social context and timing shape aging trajectories in patients with cancer.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kerstens, C. et al. A systematic review on the potential acceleration of neurocognitive aging in older cancer survivors. Cancers 15, 10.3390/cancers 15041215 (2023).10.3390/cancers 15041215 PMC 995446736831557 · doi ↗ · pubmed ↗
- 2Fries, J. F. in Handbook of the Biology of Aging (eds Masoro, E. J. & Austad, S. N.) 507–524 (Elsevier Inc, 2016).
- 3Yang, G. S. et al. Exploring the relationship between DNA methylation age measures and psychoneurological symptoms in women with early-stage breast cancer. Support. Care in Cancer 31, 10.1007/s 00520-022-07519-z (2023).10.1007/s 00520-022-07519-z 36538110 · doi ↗ · pubmed ↗
- 4Solomon, M. et al. Cross-sectional associations of proteomic age acceleration with self-reported physical and mental health and depression symptoms among those with and without cancer. J. Cancer Surviv.10.1007/s 11764-025-01803-7 (2025).10.1007/s 11764-025-01803-740304866 · doi ↗ · pubmed ↗
- 5Medawar, P. B. An unsolved problem of biology. (H K Lewis & CO, 1952).
- 6Geronimus, A. T. The weathering hypothesis and the health of African-American women and infants: evidence and speculations. Ethn. Dis.2, 207–221 (1992).1467758 · pubmed ↗
- 7Kuh, D., Cooper, R., Hardy, R., Richards, M. & Ben-Shlomo, Y. A life course approach to healthy ageing. (OUP Oxford, 2013).
- 8Bengtson, V. L., Elder, G. H. & Putney, N. M. in The Cambridge Handbook of Age and Ageing Cambridge Handbooks in Psychology (ed. Malcolm, L. J.) 493–501 (Cambridge University Press, 2005).