A Rare Case of Primary Nasal Tuberculosis
Khushboo G Malhotra, Ajeet K Khilnani, Ayush Tank, Aabha Parmar, Preet Hingrajiya

TL;DR
A rare case of nasal tuberculosis was diagnosed and successfully treated with standard anti-tubercular therapy.
Contribution
This paper presents a rare clinical case of primary nasal TB without pulmonary involvement.
Findings
Nasal endoscopy and biopsy confirmed primary nasal TB with caseating granulomas and acid-fast bacilli.
Standard anti-tubercular treatment resolved symptoms completely with no recurrence after one year.
Abstract
Primary nasal tuberculosis (TB) is an exceedingly rare form of extrapulmonary TB, often mimicking other granulomatous diseases and posing diagnostic challenges. We present a case of a 54-year-old female patient with persistent nasal obstruction and epistaxis, initially suspected to be chronic rhinosinusitis. Diagnostic evaluation, including nasal endoscopy and biopsy, revealed caseating granulomas with acid-fast bacilli (AFB), confirming primary nasal TB without pulmonary involvement. The patient was treated with a standard anti-tubercular regimen of two months of intensive phase (four drugs) and four months of continuation phase (three drugs), resulting in complete resolution of symptoms and no recurrence at one-year follow-up. This case underscores the importance of considering TB in atypical nasal presentations, especially in endemic regions, and highlights the efficacy of timely…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
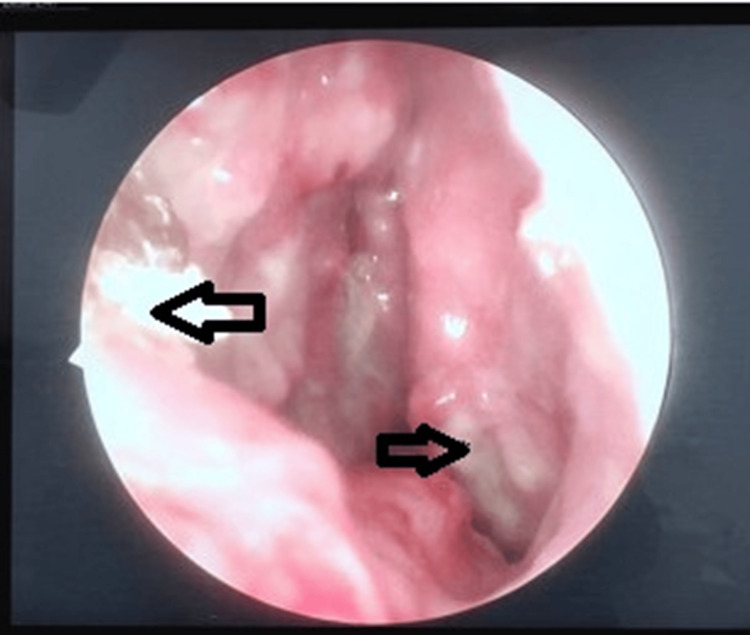 Figure 1
Figure 1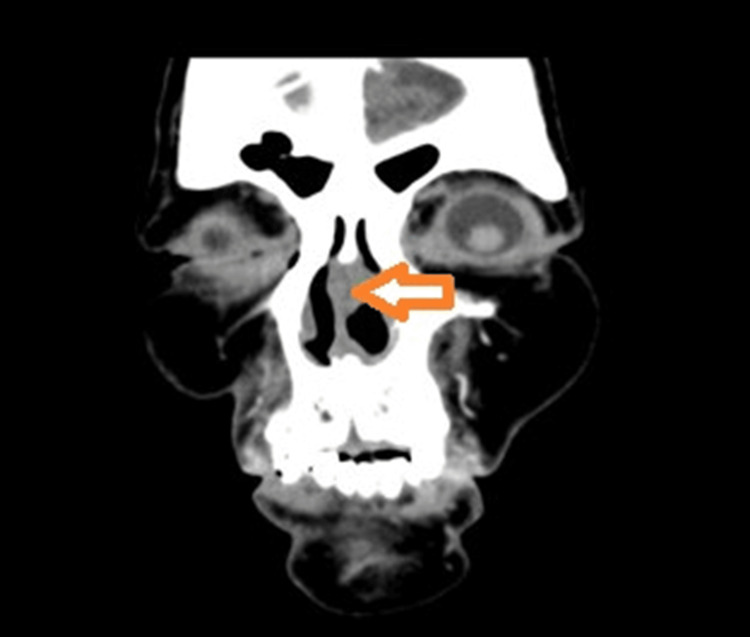 Figure 2
Figure 2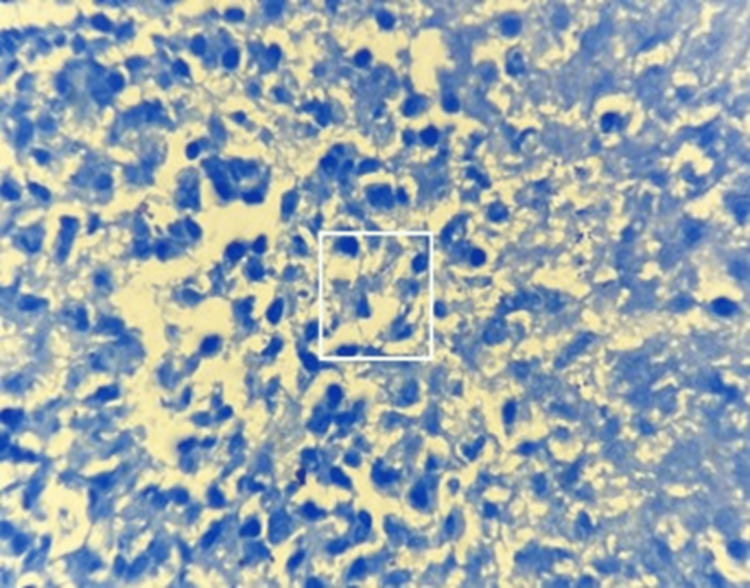 Figure 3
Figure 3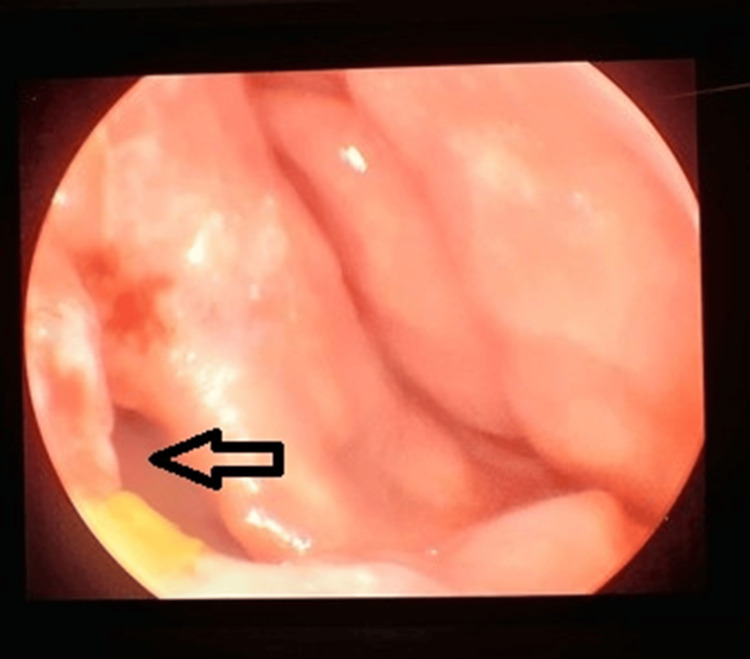 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Diseases and Tuberculosis · Sinusitis and nasal conditions · Tuberculosis Research and Epidemiology
Introduction
Tuberculosis (TB) remains a global health challenge, primarily affecting the lungs but capable of involving extrapulmonary sites in approximately 15-20% of cases. [1] Nasal TB, a subset of extrapulmonary TB, is exceptionally rare, accounting for less than 1% of all TB cases and even fewer as primary manifestations without evidence of lung disease [1]. The first documented case of nasal TB dates back to 1761, reported by Giovanni Morgagni during an autopsy [2]. People with low immunity, residing especially in the high-incidence areas, are vulnerable to primary upper respiratory TB [3]. The most common presenting symptom of nasal TB is nasal obstruction, followed by nasal discharge, nasal bleed, crusting, eye watering, postnasal discharge, recurrent nasal polyps, and ulceration, which can lead to misdiagnosis as conditions like granulomatosis with polyangiitis (GPA), sarcoidosis, or malignancy [4]. Diagnosis relies on histopathological evidence of granulomatous inflammation, acid-fast bacilli (AFB) staining, culture, or molecular tests like polymerase chain reaction (PCR) [5]. We report a rare case of primary nasal TB to illustrate its clinical features, diagnostic approach, and management.
Case presentation
A 54-year-old female patient presented to the otolaryngology clinic with a three-month history of progressive left-sided nasal obstruction, intermittent epistaxis, and mucopurulent nasal discharge. She denied fever, weight loss, cough, or night sweats, and had no history of TB exposure, immunodeficiency, or recent trauma. Her medical history was unremarkable, and she was a nonsmoker with no occupational risk factors.
Anterior rhinoscopy examination revealed a polypoidal mass in the left nasal cavity with edematous mucosa and whitish granulomatous patches on the nasal septum. There was no external nasal deformity, cervical lymphadenopathy, or ear involvement. The chest X-ray was normal, ruling out pulmonary TB.
Nasal endoscopic examination showed friable, ulcerated lesions on the left nasal septum and the inferior turbinate, with surrounding pale mucosa (Figure 1). The lesions were pale and painless and did not bleed on touch.
Left nasal endoscopic view showing ulcerative lesion over nasal septum and inferior turbinate (black arrows)
Computed tomography (CT) of the paranasal sinuses demonstrated soft tissue opacification involving the cartilaginous part of the left side of the nasal septum (Figure 2). The paranasal sinuses were not involved.
CT PNS showing soft tissue opacification of left side nasal septum (orange arrow)CT: computed tomography; PNS: paranasal sinuses
Biopsy of the nasal lesion was performed, and histopathological examination (HPE) revealed polypoidal nasal tissue comprising marked chronic inflammation, an area of necrosis, and necrotic debris. There was no evidence of granuloma or malignancy. Ziehl-Neelsen (ZN) staining demonstrated AFB (Figure 3).
ZN stain (x 100) showing acid fast bacilli (white square)ZN: Ziehl-Neelsen
Based on the above work-up, the patient was diagnosed with a case of primary nasal TB. Four-drug anti-tubercular treatment (isoniazid (INH), rifampicin (RIF), pyrazinamide (PZA), and ethambutol (EMB)) was started. The patient took the chemotherapy for six months (two months of intensive phase (four drugs) and four months of continuation phase (three drugs)), resulting in complete resolution of symptoms and no recurrence at one-year follow-up. The patient, however, had an asymptomatic nasal septal perforation (Figure 4).
Left nasal endoscopic view showing resolution of lesions and a septal perforation (black arrow)
Granulomatous disease, such as TB, affects the cartilaginous part of the nasal septum, whereas syphilis affects the bony part of the nasal septum. Septal perforation, a known sequela for TB, was found in our patient post completion of anti-tubercular treatment, but as the patient was asymptomatic, no further management was done for the same, and the patient is kept for regular follow-up.
Discussion
Primary TB of the nose is exceedingly rare, with fewer than 100 cases having been reported in the literature. There is a distinct female preponderance (female-to-male ratio is 3:1), and the mean age at diagnosis has been reported to be 40 years [6]. The nasal septum is more frequently involved than the lateral wall; if the latter is affected, the inferior turbinate is the most common location [7]. In endemic areas, the resurgence of extrapulmonary TB may be linked to factors like human immunodeficiency virus (HIV) co-infection or immunosuppressive therapies such as anti-tumor necrosis factor (TNF) agents, which can reactivate latent TB [1]. The diagnostic dilemma arises as the clinical features mimic other more common nasal pathologies [6]. For instance, GPA often presents with similar nasal crusting and ulceration but is distinguished by granuloma formation (a collection of histiocytes made up of modified macrophages/epithelioid cells), often surrounded by T lymphocytes and multinucleated giant cells [8]. Sarcoidosis features noncaseating granulomas, while fungal infections or malignancies require specific cultures or immunohistochemistry. In our patient, the absence of systemic symptoms and normal chest imaging supported a primary nasal focus, consistent with reported cases where pulmonary involvement is absent.
Treatment follows standard guidelines for extrapulmonary TB, typically involving a six- to nine-month regimen of INH, RIF, PZA, and EMB in the intensive phase, followed by INH, RIF, and EMB in the continuation phase [9]. In our case, the patient took the chemotherapy for six months (two months of intensive phase (four drugs) and four months of continuation phase (three drugs)), resulting in complete resolution of symptoms. Among the treatment options for nasal TB are drug therapy, surgical excision, diathermy, cautery, and radiotherapy [6]. Outcomes are favorable with early diagnosis, as evidenced by symptom resolution and low recurrence rates in follow-up [8].
Conclusions
This case highlights the need for a high index of suspicion for nasal TB in patients with chronic nasal symptoms unresponsive to conventional therapy. Prompt biopsy and microbiological confirmation are crucial to differentiate it from mimickers and initiate effective anti-tuberculous treatment, leading to an excellent prognosis. Increased awareness may reveal more cases, potentially indicating a resurgence rather than mere coincidence in reporting.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Extrapulmonary tuberculosis: an overview Am Fam Physician Golden MP Vikram HR 17611768722005 https://pubmed.ncbi.nlm.nih.gov/16300038/16300038 · pubmed ↗
- 2Nasal tuberculosis: a forgotten entity Laryngoscope Waldman SR Levine HL Sebek BA Parker W Tucker HM 1116911981745345710.1288/00005537-198101000-00003 · doi ↗ · pubmed ↗
- 3Primary nasal tuberculosis: a rare case report Ear Nose Throat J Zhang Z Ma Z Li Y Wang J Hou L 16104202510.1177/0145561323116224236891611 · doi ↗ · pubmed ↗
- 4Nasal tuberculosis in the 20th century Am J Med Sci Butt AA 3323353131997918614610.1097/00000441-199706000-00003 · doi ↗ · pubmed ↗
- 5Diagnosis and treatment of extrapulmonary tuberculosis Tuberc Respir Dis (Seoul) Lee JY 47557820152586133610.4046/trd.2015.78.2.47PMC 4388900 · doi ↗ · pubmed ↗
- 6Primary nasal tuberculosis-a rare clinical entity Ear Nose Throat J Lerra S Nazir T Mir Qadri S Kirmani M 0490201110.1177/01455613110900071221792783 · doi ↗ · pubmed ↗
- 7Nasal tuberculosis-an update of current clinical and laboratory investigation J Laryngol Otol Masterson L Srouji I Kent R Bath AP 21021312520112095563810.1017/S 0022215110002136 · doi ↗ · pubmed ↗
- 8Systematic identification and characterization of clinical and socio-economical correlates of granulomatous nasal and para-nasal sinuses: a large-scale study among patients of Odisha, India Heliyon Kar A Satapathy S Bepari K Panda S Kar A Satapathy S 08202210.1016/j.heliyon.2022.e 10741 PMC 951362536177245 · doi ↗ · pubmed ↗