Incidence of acute kidney injury among high-risk adult patients undergoing iso-osmolar contrasted computed tomography scans: a prospective cohort study
Miriam Nakku, Zeridah Muyinda, Valeria Nabbosa, Aloysius G Mubuuke, Joseph B Baluku, Deborah Babirye, Jonathan Walubembe, Diana O Angom, Kevina Nalwoga, Robert Kalyesubula

TL;DR
This study found a 9% incidence of kidney injury in high-risk patients after using iso-osmolar contrast for CT scans, with no clear risk factors identified.
Contribution
The study provides new empirical data on CIAKI incidence with iso-osmolar contrast in high-risk patients.
Findings
The cumulative incidence of CIAKI was 9% (20 out of 223 patients).
No factors were independently associated with CIAKI in the study population.
Abstract
The safety of iso-osmolar contrast media (IOCM) in patients at risk of contrast-induced kidney injury (CIAKI) is not well-established. To determine the incidence of CIAKI among high-risk adult patients undergoing iso-osmolar contrasted Computed Tomography (CT) scans. A prospective descriptive cohort study of patients at high risk of CIAKI was done. Questionnaires were used to collect clinical and examination findings. Blood samples were collected at baseline and at 48 hours post-administration of IOCM to assess changes in serum creatinine. Those found to have a ≥ 0.5mg/dl absolute increase in serum creatinine from the baseline within 48 hours of contrast administration were considered to have developed CIAKI. Pearson's Chi-square test was used to compare patients with and without CIAKI. Logistic regression models were used to determine associations of CIAKI. The cumulative incidence…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
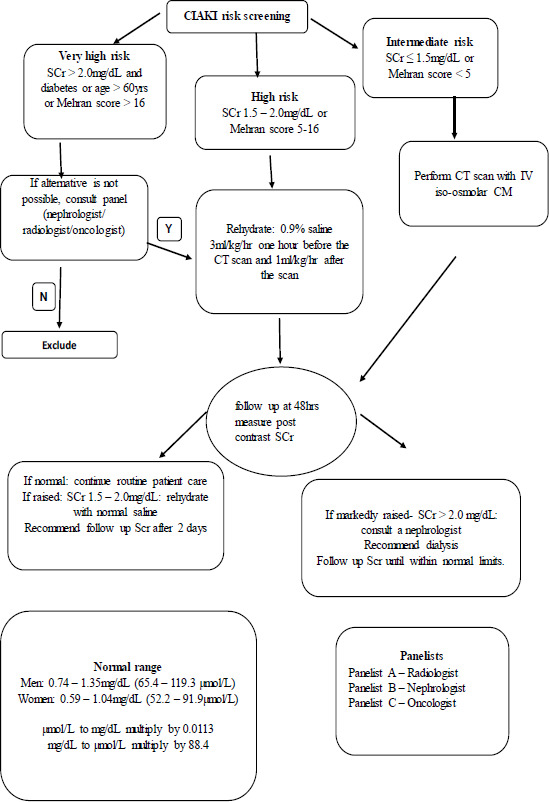 Figure 1
Figure 1| Total n (%) | Developed n (%) | CIAKI | P-value | ||
|---|---|---|---|---|---|
|
|
|
| |||
| Head | 28(12.6) | 26(92.9) | 2(7.1) | 0.925 | |
| Chest | 66(29.6) | 60(90.9) | 6(9.1) | ||
| Abdomen | 109(48.9) | 100(91.7) | 9(8.3) | ||
| Pelvic | 1(0.5) | 1(100) | 0(0) | ||
| Angiogram | 7(3.1) | 6(85.7) | 1(14.3) | ||
| Others | 12(5.4) | 10(83.3) | 2(16.7) | ||
|
| |||||
| No | 219(98.2) | 200(91.3) | 19(8.7) | 0.257 | |
| Yes | 4(1.8) | 3(75) | 1(25) | ||
|
| |||||
| No | 181(81.2) | 167(92.3) | 14(7.7) |
| |
| Yes | 42(18.8) | 36(85.7) | 6(14.3) | ||
|
| |||||
| No | 116(52.0) | 106(91.4) | 10(8.6) | 0.850 | |
| Yes | 107(48.0) | 97(90.7) | 10(9.3) | ||
|
| |||||
| No | 150(67.3) | 137(91.3) | 13(8.7) | 0.821 | |
| Yes | 73(32.7) | 66(90.4) | 7(9.6) | ||
|
| |||||
| No | 24(10.8) | 20(83.3) | 4(16.7) |
| |
| Yes | 199(89.2) | 183(92.0) | 16(8.0) | ||
|
| |||||
| No | 222(99.5) | 202(91.0) | 20(9.0) | 0.753 | |
| Yes | 1(0.5) | 1(100) | 0(0) | ||
|
| |||||
| No | 212(95.1) | 192(90.6) | 20(9.4) | 0.286 | |
| Yes | 11(4.9) | 11(100) | 0(0) |
| Total n (%) | Developed | CIAKI n (%) | P-value | ||
|---|---|---|---|---|---|
|
|
|
| |||
| Yes | 16(7.2) | 14(87.5) | 2(12.5) | 0.608 | |
| No | 207(92.8) | 189(91.3) | 18(8.7) | ||
|
| |||||
| <60 mL/min/1.73m2 | 28(12.6) | 25(89.3) | 3(10.7) | 0.730 | |
| ≥60 mL/min/1.73m2 | |||||
| 195(87.4) | 178(91.3) | 17(8.7) | |||
|
| |||||
| Above 35 – Safer | 176(78.9) | 162(92.1) | 14(7.9) | 0.305 | |
| Below 36 – At Risk | 47(21.1) | 41(87.2) | 6(12.8) | ||
|
| |||||
| Below 60ml – Safer | 89(39.9) | 82(92.1) | 7(7.9) | 0.638 | |
| Above 60ml – At Risk | 134(60.1) | 121(90.3) | 13(9.7) | ||
|
| |||||
| Less or Equal to 5 | 172(77.1) | 160(93) | 12(7) |
| |
| 6 – 10 | 43(19.3) | 37(86.1) | 6(13.9) | ||
| 11 – 16 | 8(3.6) | 6(75) | 2(25) | ||
|
| |||||
| Yes | 156(70.0) | 137(87.8) | 19(12.2) |
| |
| No | 67(30.0) | 66(98.5) | 1(1.5) | ||
|
| |||||
|
| |||||
| No Reaction | 80(35.9) | 77(96.3) | 3(3.7) |
| |
| Mild – No Treatment | 143(64.1) | 126(88.1) | 17(11.9) | ||
|
| |||||
| No Reaction | 220(98.6) | 200(90.9) | 20(9.1) | 0.584 | |
| Mild – No Treatment | 3(1.4) | 3(100) | 0(0) | ||
|
| |||||
| No Reaction | 190(85.2) | 174(91.6) | 16(8.4) | 0.492 | |
| Mild – No Treatment | 33(14.8) | 29(87.9) | 4(12.1) | ||
|
| |||||
| No Reaction | 173(77.6) | 162(93.6) | 11(6.4) |
| |
| Mild – No Treatment | 50(22.4) | 41(82) | 9(18) | ||
|
| |||||
| No Reaction | 208(93.3) | 192(92.3) | 16(7.7) |
| |
| Mild – No Treatment | 15(6.7) | 11(73.3) | 4(26.7) | ||
|
| |||||
| No Reaction | 188(84.3) | 172(91.5) | 16(8.5) | 0.790 | |
| Mild – No Treatment | 34(15.3) | 30(88.2) | 4(11.8) | ||
| Moderate – Treatment Necessary | 1(0.4) | 1(100) | 0(0) | ||
|
| |||||
| No Reaction | 221(99.1) | 201(90.9) | 20(9.1) | 0.656 | |
| Mild – No Treatment | 2(0.9) | 2(100) | 0(0) | ||
|
| |||||
| No Reaction | 219(98.2) | 199(90.9) | 20(9.1) | 0.818 | |
| Mild - No Treatment | 3(1.4) | 3(100) | 0(0) | ||
| Moderate – Treatment Necessary | 1(0.4) | 1(100) | 0(0) | ||
|
| |||||
| No Reaction | 216(96.9) | 197(91.2) | 19(8.8) | 0.617 | |
| Mild – No Treatment | 7(3.1) | 6(85.7) | 1(14.3) | ||
|
| |||||
|
| |||||
| Yes | 20(9.0) | 16(80) | 4(20) | 0.070 | |
| No | 203(91.0) | 187(92.1) | 16(7.9) |
| Outcome: Developed CIAKI | Adjusted Odds Ratios (95% CI) | P>z |
|---|---|---|
|
| ||
| Below 60 Years | 1.00 | |
| Above 60 Years | 1.17(0.34-3.98) | 0.798 |
|
| ||
| No | 1.00 | |
| Yes | 0.94(0.26-3.41) | 0.935 |
|
| ||
| No | 1.00 | |
| Yes | 0.3(0.06-1.5) | 0.143 |
|
| ||
| Yes | 1.00 | |
| No | 2.02(0.47-8.69) | 0.342 |
|
| ||
| 11 – 16 | 1.00 | |
| Less than or Equal 5 | 0.29(0.03-2.88) | 0.295 |
| 6 – 10 | 0.44(0.05-3.87) | 0.463 |
|
| ||
| No | 1.00 | |
| Yes | 10.43(0.79-136.64) | 0.074 |
|
| ||
| No Reaction | 1.00 | |
| Mild – No Treatment | 1.01(0.19-5.16) | 0.989 |
|
| ||
| No Reaction | 1.00 | |
| Mild – No Treatment | 1.87(0.63-5.55) | 0.256 |
|
| ||
| No Reaction | 1.00 | |
| Mild – No Treatment | 1.5(0.31-7.29) | 0.610 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Kidney Injury Research · Atrial Fibrillation Management and Outcomes · Chronic Kidney Disease and Diabetes
Background
The use of iodinated contrast media (CM) has increased globally1. This is because CM allows excellent visualization of structures, enabling clinicians to make proper diagnoses; improving patient management and quality of life2.
Despite the improved quality of CM, many adverse reactions like acute kidney injury (AKI) remain a major concern for clinicians3,4. These reactions may be mild, moderate or severe and can occur immediately or later post contrast administration1,5. Most of these adverse effects can be minimized or treated early when anticipated6.
The incidence of adverse effects is reported to be significantly reduced with the use of iso-osmolar contrasted media (IOCM)4,7. According to international guidelines, both iso-osmolar and low-osmolar CM are recommended for use in patients with increased risk of contrast-induced acute kidney injury (CIAKI)3,8-10.
Patients with co-morbidities like cancer, diabetes mellitus (DM) and renal impairment have a higher risk of acquiring adverse effects11,12. Therefore, care must be taken to prevent disease progression, reduced quality of life, increased hospital stay or even death by using appropriate CM2,13-16.
The incidence of CIAKI is reported to be as high as 50% in high-risk patients with majority of studies reporting ranges between 20-30%17. This has been attributed to the volumes and type of contrast media used. With the use of IOCM, the incidence is reported to be as low as 6.3%12 making it a safer contrast agent17,18.
The purpose of this study was to determine the incidence of acute kidney injury among high-risk adult patients undergoing iso-osmolar contrasted computed tomography (CT) scans.
This will provide a scientific guide on the safety profile of IOCM use among high-risk patients, allowing timely imaging, diagnosis and management, improving quality of life.
Materials and methods
Study aim, design, population and setting
This was a prospective descriptive cohort study aimed at determining the incidence of AKI among high-risk adult patients undergoing iso-osmolar contrasted CT scans at three centers in Kampala, Uganda. It was conducted at the Uganda Cancer Institute (UCI), St Francis Hospital Nsambya (SFHN) and Mulago National Referral Hospital (MNRH): all of which are tertiary institutions receiving patients from all over the country. The study population consisted of all consenting high-risk adult patients (chronic kidney disease (CKD), DM, cancer, hypertension, Human Immuno-deficiency Virus (HIV) or multiple co-morbidities) that presented for a contrasted CT scan.
A protocol for the purpose of renal protection (see figure 1 below) was developed by panelists including a radiologist, nephrologist and an oncologist prior to commencement of the study that was followed.
Protocol for contrasted CT risk according to American College of Radiology (ACR) criteria with modification. Goldfarb et al, 2009
We excluded very ill patients whose vitals could not be taken or who could not be well positioned for the CT scan, patients who had had a contrasted CT scan performed in the previous three weeks and those with a baseline serum creatinine (SCr) of > 2.0mg/dL that were considered unfit by the panel.
Data collection
Consecutive sampling was used. The independent variables were: age, sex, place of residence, occupation, level of education, marital status, type CT scan type, volume of CM, comorbidities like CKD, hypertension, DM, cancer, HIV, concurrent drug use and other therapies (Non-Steroidal Anti-Inflammatory Drugs, Highly Active Antiretroviral Therapy, chemotherapy, radiotherapy, oral anti-hyperglycemic agents, and anti-hypertension medication). The dependent variables were: CIAKI and adverse effects.
SCr levels were measured at baseline and at 48hours post contrasted CT scan using IOCM [Visipaque - iodixanol, General Electric Company (GE Healthcare)]. Patients found with an absolute increase of SCr ≥ 0.5 mg/dl from the baseline were considered to have developed CIAKI.
Data analysis
Data was electronically entered using Microsoft Access 2016, exported into Excel 2016 and analyzed using STATA version 17.0
Statistical analysis was done in 3 stages. In the univariate analysis, data was presented as frequencies, proportions, means and medians with their measures of dispersion. The cumulative incidence of CIAKI was measured as the proportion of patients that developed CIAKI at 48 hours.
At the bivariate stage, a Chi-square test was used to measure association between the dependent and independent variables. Independent factors with a Chi-square p-value ≤ 0.2 were considered to have a significant association with development of CIAKI and were further tested using logistic regression to check for the association with usage at the multivariate stage.
Results
223 participants were enrolled. The mean age was 56.5 (SD 14.5) years. 45.3% had a BMI of 18.5-24.9, 16.1% below 18.5, 23.8% between 25-29.9 and 14.8% above 30.
Cumulative incidence of CIAKI
The proportion of high-risk patients that developed CIAKI was 9% (20) (95% CI 5.8451-13.5215) out of the 223 participants. Characteristics of participants are shown in tables 2-3. The statistically significant factors (p < 0.2) among participants that developed CIAKI were age, diabetes, cancer, metformin use, reduced urine output, Mehran risk score and adverse effects: pain at injection site, nausea and vomiting.
Factors associated with development of CIAKI
As shown in table 4, there were no independent factors statistically significantly associated with CIAKI.
Discussion
The cumulative incidence of CIAKI was 9%. This is similar to many studies in high-risk patients with IOCM use where incidences of < 12% have been noted3,10,19. This is because IOCM is safer for use in high-risk patients compared to other CM agents where incidences as high as 20-30% have been reported10,17,20,21. The safety of IOCM has been attributed to its reduced cytotoxicity and nephrotoxicity19.
In a similar study carried out in Germany by Werner et al an incidence of 6.3% was registered. This study had a slightly higher incidence possibly because higher volumes of CM > 60mls were used compared to those (60mls) used in Germany12. The use of low doses of CM reduces the risk of CIAKI.
In another study conducted in Kenya by Kwasa et al using IOCM in patients with inflammation, the incidence of CIAKI was found to be 9.92%. Inflammation is however present in most of the risk factors predisposing to CIAKI and therefore these results were comparable to those in this study22.
In this study, there were no factors independently associated with development of CIAKI at the multivariate level. This could be due to the different ethnic population in which the study was carried out and the fact that IOCM is regarded safe among the high-risk groups3,10,17,19,20. Furthermore, the use of the reno-protective protocol developed in this study could have played a role.
Therefore, this study demonstrated that IOCM can be safely used among high-risk patients with minimal fear of developing CIAKI. The strength of the study lies in its sizable sample size representative of the high-risk patients drawn from three different centers. The findings generated from the study thus contribute to literature on the incidence of developing acute kidney injury following IOCM use among high-risk patients.
Limitation of the study was underestimating the incidence of CIAKI given the short duration of follow up. Despite the limitation, the findings are useful to guide on CM use in imaging high-risk patients who have always been approached with fear. We do recommend further research specifically looking at a longer follow up period.
Conclusion
The incidence of CIAKI among high-risk adult patients undergoing iso-osmolar contrasted CT scans in this study was 9%, which is relatively low compared to previously reported literature. IOCM can therefore be used among high-risk adult patients during their clinical management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bottinor W Polkampally P Jovin I Adverse reactions to iodinated contrast media The International Journal of Angiology: official publication of the International College of Angiology, Inc 20132231492443660210.1055/s-0033-1348885 PMC 3770975 · doi ↗ · pubmed ↗
- 2Andreucci M Solomon R Tasanarong A Side Effects of Radiographic Contrast Media: Pathogenesis, Risk Factors, and Prevention Bio Med Research International 201420147410182489560610.1155/2014/741018 PMC 4034507 · doi ↗ · pubmed ↗
- 3Zhao F Lei R Yang S-K Luo M Cheng W Xiao Y-Q Comparative effect of iso-osmolar versus low-osmolar contrast media on the incidence of contrast-induced acute kidney injury in diabetic patients: a systematic review and meta-analysis Cancer Imaging 2019191383121548810.1186/s 40644-019-0224-6PMC 6580528 · doi ↗ · pubmed ↗
- 4Mehran R Nikolsky E Contrast-induced nephropathy: definition, epidemiology, and patients at risk Kidney International 200669 S 11S 1510.1038/sj.ki.500036816612394 · doi ↗ · pubmed ↗
- 5Cochran ST Bomyea K Sayre JW Trends in adverse events after IV administration of contrast media American Journal of Roentgenology 20011766138513881137319710.2214/ajr.176.6.1761385 · doi ↗ · pubmed ↗
- 6Thomsen H Bush W Treatment of the adverse effects of contrast media Acta Radiologica 1998393212218957193110.1080/02841859809172182 · doi ↗ · pubmed ↗
- 7Onyambu CK Aywak AA Osiemo SK Mutala TM Anaphylactic Reactions in Radiology Procedures Recent Advances in Asthma Research and Treatments 2021 Intech Open
- 8Isola S Furci F Gangemi S The involvement of osmolarity in the safety of contrast media Clinical and Molecular Allergy 2018161193018604310.1186/s 12948-018-0097-4PMC 6120064 · doi ↗ · pubmed ↗