Early experience with pericardiectomy for constrictive pericarditis in Ile-Ife, Nigeria: a retrospective analysis
Olugbenga O Ojo, Uvie U Onakpoya, Oluwaseun R Akanbi, Abayomi E Oguns, Mathias O Ikokoh

TL;DR
This paper reports on pericardiectomy outcomes in Nigeria, showing most patients improved after surgery for constrictive pericarditis.
Contribution
The study provides early experience and outcomes of pericardiectomy in a Nigerian tertiary hospital setting.
Findings
Thirteen patients underwent pericardiectomy with a median ICU stay of 2 days and 1 mortality.
Over 90% of surviving patients showed significant improvement in heart function at 12 months.
Common symptoms included dyspnea and ascites, with most patients in advanced NYHA classes pre-surgery.
Abstract
Constrictive pericarditis is a rare but important cause of diastolic heart failure. Its uniqueness lies in the fact that surgery (pericardiectomy) remains the mainstay of treatment. Globally, the leading causes of constrictive pericarditis include idiopathic, mediastinal irradiation, post cardiac surgery and tuberculosis. Patients who underwent pericardiectomy at our tertiary hospital between January 2019 and December 2024 were retrospectively studied with the aim of discussing our experience with the procedure and its outcomes. Data including baseline demographics, preoperative conditions, intraoperative details, and postoperative outcomes were collected from clinical records and analysed. Thirteen patients had total pericardiectomy during the period under review. The median age was 28 years with dyspnoea and ascites being the most common symptoms. Most patients (61.6%) presented in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
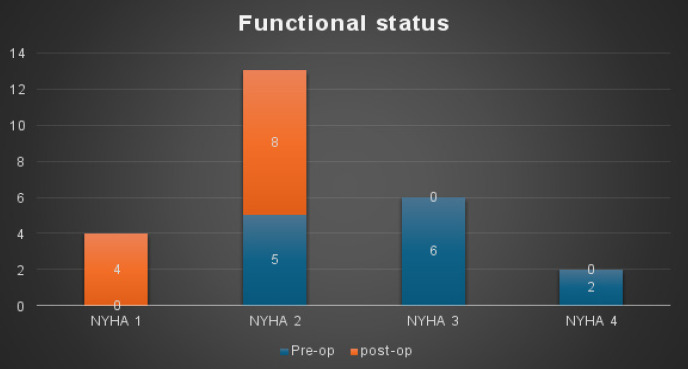 Figure 1
Figure 1| Characteristic/Variable | Value n (%) |
|---|---|
|
| |
| Median | 28 years |
| | 18 years |
| <18years | 3 (23.1%) |
| >18years | 10(76.9%) |
|
| |
| Male | 7(53.8%) |
| Female | 6(46.2%) |
|
| |
| Dyspnoea | 13(100%) |
| Orthopnoea | 8(61.5%) |
| Jugular venous distension | 10(76.9%) |
| Hepatomegaly | 9(69.2%) |
| Ascites | 12(92.3%) |
| Right pleural effusion | 4(30.8%) |
| Bilateral pleural effusion | 6(46.2%) |
|
| |
| Echo alone | 5(38.5%) |
| Echo + chest CT | 8(61.5%) |
|
| |
| No < 14days | 9(69.2%) |
| Yes > 14days | 4(30.8%) |
|
| |
| Fibrous constrictive | 7(53.8%) |
| Effusive constrictive | 6(46.2%) |
| Characteristic/Variable | Value n (%) |
|---|---|
| Median | 302 |
| | 229.5 to 330 mins |
| Median | 450 |
| IQR | 300 to 1,250 mins |
| Median | 2 days |
| IQR | 2 to 21 |
|
| |
| Yes | 3(23.1) |
| No | 10(76.9) |
|
| |
| | 4(30.7%) |
| Coagulopathy | 1(7.7%) |
| Inadvertent cardiotomy | 1(7.7%) |
| Prolonged pleural effusion | 1(7.7%) |
|
| |
| Tuberculous pericarditis | 5(38.5%) |
| Nonspecific chronic inflammation (Probably Tuberculous) | 8(61.5%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPericarditis and Cardiac Tamponade · Intraperitoneal and Appendiceal Malignancies · Adrenal and Paraganglionic Tumors
Introduction
Constrictive pericarditis (CP) is one of the surgically correctable causes of heart failure. It results from chronic inflammation and fibrosis of the pericardium leading to impairment of diastolic filling and right heart failure1,2. The aetiology of constrictive pericarditis is diverse, with viral or idiopathic causes and post cardiotomy irritation being the leading causes in Western population. In developing countries, tuberculosis remains the main aetiology for chronic inflammation leading to constrictive pericarditis3.
Early diagnosis of CP and referral for pericardiectomy has been shown to improve outcomes and chances of achieving post operative normal cardiac functions4,5. Though pericardiectomy with its various modifications and surgical approaches remains the mainstay of treatment for constrictive pericarditis, several reports show that post operative hemodynamics have varied from normal findings making several researchers to arrive at the conclusion that restoration of normal cardiac function rarely occurs after a pericardiectomy6–8.
Although medical therapy for heart failure with or without treatment for tuberculosis is usually commenced by the referring physicians, this should not necessarily delay the referral and performance of a pericardiectomy in patients who are fit. The aim of this study is to review the early experience with pericardiectomy in the treatment of constrictive pericarditis in Ile-Ife.
Materials and Methods
All patients who had clinical, echocardiographic, radiological and pathological post-resection confirmation of constrictive pericarditis and who underwent pericardiectomy for constrictive pericarditis at the Obafemi Awolowo University Teaching Hospitals Complex (OAUTHC) Ile-Ife between January 2019 and December 2024 were retrospectively reviewed. Data was obtained from hospital medical records using a predesigned proforma. Patients who had concomitant pericardiectomy while undergoing repair of congenital or acquired heart diseases were excluded. The procedure performed in all patients was a total pericardiectomy, from phrenic to phrenic and from great vessels to diaphragm ensuring that, the caval vessels were also free of constriction.
The data included, demographic characteristics, presenting complaints, preoperative functional status, intraoperative details, and postoperative outcome. In-hospital mortality was defined as death occurring within 30 days of operation or within the hospitalization period of the operation.
Statistical analysis
Data obtained was analysed with the SPSS statistical package (version 27). Categorical variables were expressed as percentages and proportions while continuous variables were expressed as mean and standard deviations. Association between variables were analysed by the fisher exact test for categorical variables and the student's t-test for continuous variables. A p-value of ≤0.05 was considered statistically significant.
Ethical approval was obtained from the ethics and research committee of the Obafemi Awolowo University Teaching Hospital (OAUTHC) Ile-Ife.
Results
Thirteen patients had pericardiectomy during the period comprising 7 males (53.8%) and 6 females (46.2%) with a male/female ratio of 1/1 in the study population. The median age was 28 years (IQR:18-39;) and three (23.1%) patients were less than 18 years old. The most common presenting complaints were dyspnoea and ascites (Table 1). Most patients (61.6%) presented in New York Heart Association (NYHA) functional class III or IV and were above ASA II classification at the time of surgery. The median duration of symptoms before diagnosis was 8 months (IQR: 2.5-30) and all patients had echocardiography done while 8 patients (61.5%) had computerized tomography scan in addition to echocardiographic diagnosis. Six cases (46.2%) were effusive constrictive pericarditis and seven (53.8%) were non-effusive (fibrous constrictive) pericarditis. All cases were done without the use of cardiopulmonary bypass, and the median duration of surgery was 302minutes (IQR: 229-330). The, median post operative blood loss was 450 mL (IQR:300-1250) and only one patient required re-sternotomy due to excessive mediastinal bleeding. All patients were extubated on table and transferred to the intensive care unit (ICU) with a median ICU stay of 2days:(IQR: 2-2) (Table 2).
Low cardiac output state was the commonest complication seen in this study occurring in 4(30.8%) patients with 3 of them requiring post operative inotropic support (Table 2). There was one in-hospital mortality in a patient with COVID-19 infection who developed a coagulopathy on post operative day 1. At 12 months follow-up period 4 (33.3%) out of the surviving patients were in NYHA functional class I, while 8 (66.7%) patients were in NYHA class II. Histopathological examination of specimen taken at pericardiectomy confirmed tuberculous pericarditis as the aetiology in 5(38.5%) and nonspecific chronic inflammation possibly due to tuberculosis in the remaining 8(61.5%) cases.
Discussion
Constrictive pericarditis is a relatively rare but notable cause of diastolic heart failure. Even in centres where large series have been published, there are fewer than twelve cases annually9–13.
This study presents early findings from a major referral tertiary institution in southwest Nigeria and demonstrates that many patients in this environment present late, with 61.6% of them being classified as New York Heart Association (NYHA) functional class III and IV upon presentation. Our finding is contrary to other studies9,11,14 where most patients were in NYHA class II or III. Biçer et al. found 76% of patients and Peset et al. found 67% in these classes14,15. The difference in NYHA functional class at presentation between our study and previous studies may be attributed to variations in health-seeking behaviour among patients in different environments. Similar studies from Kumasi and Accra in Ghana also found that most patients presented in NYHA functional class III and IV16,17. Dyspnoea was the most prevalent symptom observed in our study, consistent with the findings of Biçer et al.
The median age in this study was 28 years, with an interquartile age range of 18 to 39 years which is similar to other publications in the West African subregion16,17 In the study conducted by Tettey et al16., the average age of participants was 33 years and,. Lin et al11,. also demonstrated comparable findings in their research.
Diagnosis of constrictive pericarditis was made in less than 14 days in 69.2% of the patients. Constrictive pericarditis was diagnosed using transthoracic echocardiography in 5 patients (38.5%) and a combination of echocardiography and chest CT scan in 8 patients (61.5%).
Consistent with the findings of numerous studies conducted in developing countries,7,16,17,18 this study identified tuberculosis as the most prevalent cause of constrictive pericarditis in treated patients.
All the pericardiectomies in this study were done via a full median sternotomy without the use of cardiopulmonary bypass and NYHA functional status improved to at least NYHA class II. Figure 1.
Pre and post-operative functional status
Chowdhury et al.,7 found that total pericardiectomy (phrenic to phrenic) via a median sternotomy resulted in early normalization of hemodynamic parameters and improved long-term survival, without the routine use of cardiopulmonary bypass being necessary. Similarly, Biçer et al., demonstrated an improvement in functional status by at least one NYHA class in 80% of their patients14.
Low cardiac output syndrome (LCOS) was the most common complication, consistent with previous studies7,16,18. However, three out of the four patients with postoperative LCOS needed inotropic support, and all showed improved cardiac function within a week. No mortality was observed among patients with postoperative low cardiac output syndrome (LCOS), and all exhibited improvement in their functional status.
In-hospital mortality occurred in 1 (7.7%) patient, aligning with studies reporting 6-10% mortality rates. More recent studies by Welch et al. and Biçer et al. found rates below 5%4,14.
A larger study from sub-Saharan Africa reported a 16% in-hospital mortality rate due to procedures performed in an earlier decade, with low output cardiac failure being the major cause.18 In our study, in-hospital mortality occurred in a patient with COVID-19 infection who was operated upon within 2 weeks of a negative PCR (polymerase chain reaction) test result and who experienced significant mediastinal bleeding and required re-sternotomy, where no surgical bleed was found. The haemorrhage and subsequent demise were attributed to disseminated intravascular coagulopathy likely caused by COVID-19 infection.
At a twelve-month follow-up, over 90% of surviving patients were classified as NYHA class I or II. In agreement with the findings of Tettey et al.,16 it is believed that this outcome can generally be achieved by ensuring the adequate removal of the thickened pericardium over the right atrium and the superior and inferior vena cavae as part of the procedure. Chowdhury et al.,7 have demonstrated that this can only be accomplished via a full median sternotomy with or without cardiopulmonary bypass.
Conclusion
Our initial experience with pericardiectomy for constrictive pericarditis shows promising results, comparable to larger studies globally and demonstrates that total pericardiectomy can safely be performed without cardiopulmonary bypass in most cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Miranda WR Oh JK Constrictive Pericarditis: A Practical Clinical Approach Prog Cardiovasc Dis 20175943693792806226710.1016/j.pcad.2016.12.008 · doi ↗ · pubmed ↗
- 2Murashita T Schaff H V Daly RC Oh JK Dearani JA Stulak JM Experience with pericardiectomy for constrictive pericarditis over eight decades Ann Thorac Surg 201710437427502876046810.1016/j.athoracsur.2017.05.063 · doi ↗ · pubmed ↗
- 3Huang JB Tang YT Pericardiectomy for Constrictive Pericarditis with or without Cardiopulmonary Bypass Vasc Health Risk Manag 2024203946 Pub Med 3834840410.2147/VHRM.S 439292 PMC 10860389 · doi ↗ · pubmed ↗
- 4Welch TD Constrictive pericarditis: diagnosis, management and clinical outcomes Heart 20181049725731 Pub Med 2917597810.1136/heartjnl-2017-311683 · doi ↗ · pubmed ↗
- 5Moss R Ali AM Mahgerefteh J Panesar LE Pastuszko P Murthy R Pericardiectomy for Successful Treatment of Constrictive Pericarditis in a Pediatric Patient JACC Case Rep 2023 Oct 42310.1016/j.jaccas.2023.102009 PMC 1063586637954955 · doi ↗ · pubmed ↗
- 6Senni M Redfield MM Ling LH Danielson GK Tajik AJ Oh JK Left ventricular systolic and diastolic function after pericardiectomy in patients with constrictive pericarditis: Doppler echocardiographic findings and correlation with clinical status J Am Coll Cardiol 199933511821188 Pub Med 1019371410.1016/s 0735-1097(98)00693-7 · doi ↗ · pubmed ↗
- 7Chowdhury UK Subramaniam GK Kumar AS Airan B Singh R Talwar S Pericardiectomy for constrictive pericarditis: A clinical, echocardiographic, and hemodynamic evaluation of two surgical techniques Annals of Thoracic Surgery 20068125225291642784310.1016/j.athoracsur.2005.08.009 · doi ↗ · pubmed ↗
- 8Kusunose K Dahiya A PopovićZB Motoki H Alraies MC Zurick AO Biventricular mechanics in constrictive pericarditis comparison with restrictive cardiomyopathy and impact of pericardiectomy Circ Cardiovasc Imaging 2013633994062353250810.1161/CIRCIMAGING.112.000078 · doi ↗ · pubmed ↗