Comprehensive cardiometabolic rehabilitation program for childhood obesity
Nicole González Concha, Litsbett Velásquez Fuentes, Denys Urrea Pereira, Jorge Díaz Olivares, Hugo Berríos-Arvey

TL;DR
A new program for childhood obesity in Chile is shown to be cost-effective and could improve health outcomes and reduce costs.
Contribution
The paper introduces a cost-effective Pediatric Cardiometabolic Rehabilitation program for childhood obesity in Chile.
Findings
The program has a positive Net Present Value and an Internal Rate of Return of 13%.
The interventions could be 49% cheaper than the current strategy.
The program could improve the Human Development Index by 0.585%.
Abstract
Obesity is a public health problem in Chile, with 31% of adults and 54% of children affected. Current public policies present gaps in prevention with 44% of obese children. In Penco-Lirquén, a comprehensive and personalized Pediatric Cardiometabolic Rehabilitation program is proposed. Analyze the cost-effectiveness of program. Characterization of supply and demand, together with a technical-financial study to determine viability and cost-effectiveness. The economic viability with a positive Net Present Value and an Internal Rate of Return of 13% estimates that the interventions could be 49% cheaper than the current strategy and improve the Human Development Index by 0.585%. The implementation of the program is proposed as a cost-effective strategy, promoting healthy habits and optimizing health resources. The prevention and treatment of obesity must be prioritized globally to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
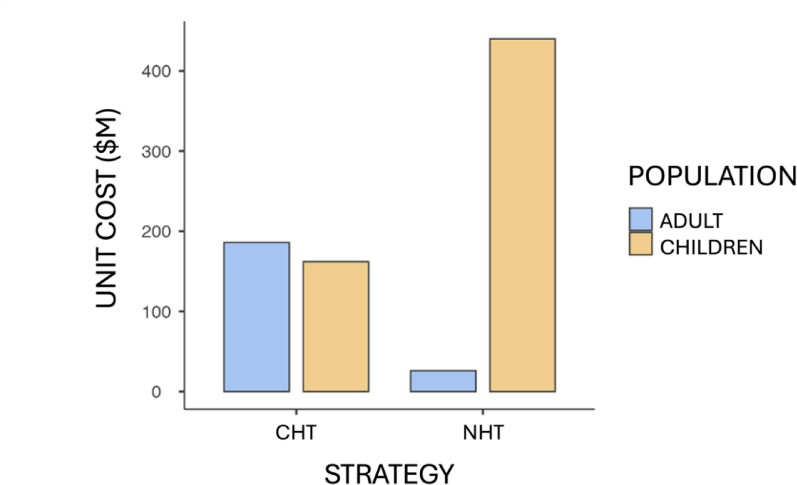 Figure 1
Figure 1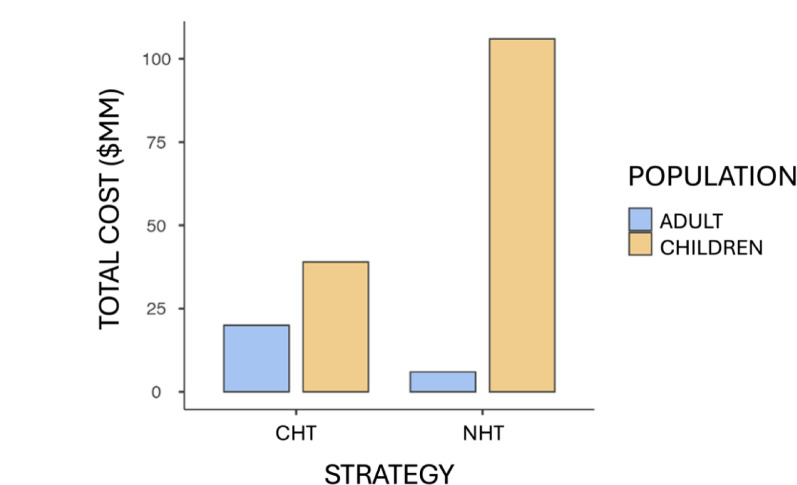 Figure 2
Figure 2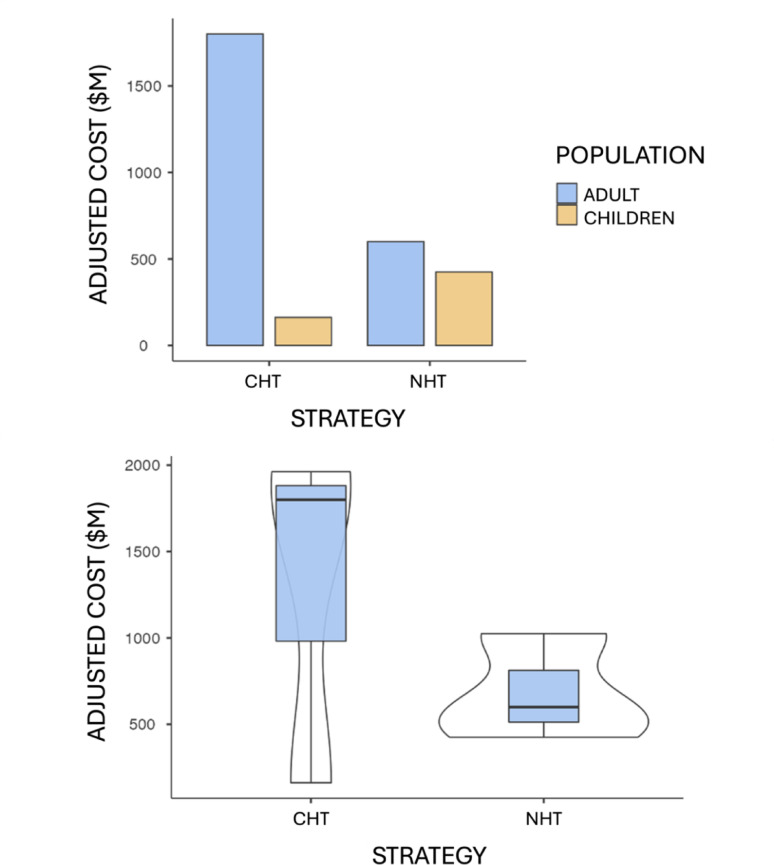 Figure 3
Figure 3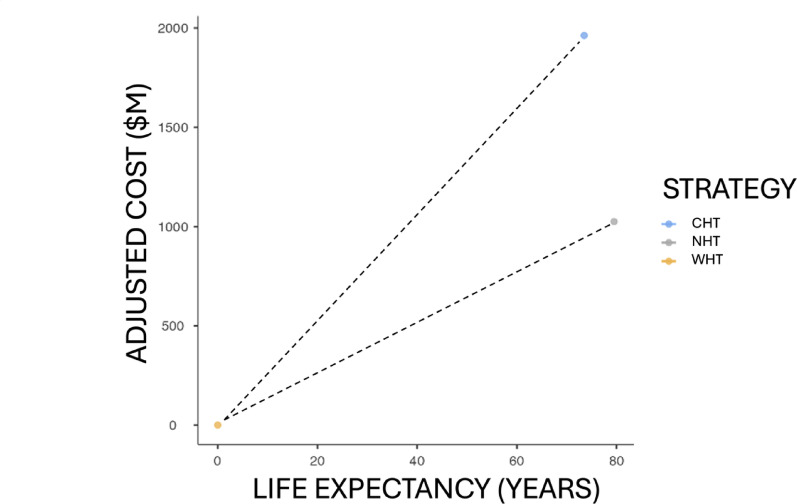 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsObesity, Physical Activity, Diet · Cardiovascular and exercise physiology · Pharmacology and Obesity Treatment
Background
Globally, obesity is a growing health problem, with a high prevalence in adults and children. In Chile, about 31% of adults are obese and 54% of children are overweight or obese, which leads to the development of unfavorable physical, psychological and social conditions [1, 2]. Associated multimorbidity is a matter of interest in public health, with overweight being a factor that increases the risk of developing it by 26%, while obesity almost doubles it, which is why state policies present intersectoral strategies for its intervention [3].
In terms of preventive medicine, the Child Health Control strategy aimed at children from 0 to 9 years old, allows for the evaluation of the environment, identification of risks and enhancement of parenting skills, including comprehensive development, biopsychosocial approach, family environment, nutritional condition and diagnosis of health problems [4]. For its part, the Comprehensive Health Control of Adolescents, aimed at adolescents from 10 to 19 years old, focuses on the evaluation of their health and development status through the early identification of protective and risk factors, in addition to the provision of integrated services and continuity of care [5]. Finally, the Choose Healthy Life Program focuses on preventing and reducing chronic non-communicable diseases and promoting healthy habits, considering specific criteria such as overweight and obesity, to provide effective treatments with a multidisciplinary team. In addition, the Preventive Medical Examination (PME) is a periodic, voluntary health evaluation free of charge for the user, [6] Aimed at beneficiaries of the National Health Fund and Health Insurance Institutions, whose main objective is the early detection of prevalent diseases in the country, allowing control and treatment measures to be implemented immediately [7]. This corresponds to Current Health Technology (CHT).
In addition to preventive interventions, for the monitoring of users who already have pathologies associated with their metabolic control, there is the Cardiovascular Health Plan (CHP) in Primary Health Care (PHC), to reduce the incidence of cardiovascular events and prevent premature morbidity and mortality [8]. In addition, and specifically, Type 2 Diabetes Mellitus (DM2) is covered by the Explicit Health Guarantees (EHG) regime, with guaranteed access to diagnostic confirmation within 30 days of suspicion and treatments within 24 h after diagnostic confirmation [9]. Meanwhile, Arterial Hypertension (AHT) is also included in EHG for beneficiaries aged 15 years with diagnostic confirmation within a maximum of 45 days from suspicion and treatment within 24 h after confirmation; [10] Meanwhile, dyslipidemia (DLP) can be detected in asymptomatic phases of atherosclerotic cardiovascular diseases, so universal screening is recommended from the age of 20, including a fasting lipid profile when the screening is positive; although this condition is not EHG, its detection is included in the PME [11].
Despite these strategies, in Chile the 2023 National Health Survey reports that 45% of households have a member with a chronic disease, where 56.4% have conditions associated with obesity and cardiovascular diseases and the records of the 2017 National Health Survey refer to 17.5% of the population living with five or more diseases, causing the costs associated with obesity, both direct such as medical care, and indirect such as loss of productivity, to be of great interest [1, 2].
Evidence indicates that obese individuals face approximately 30% higher medical costs than those of normal weight, with an estimated 1.9% to 4.7% of total health care costs attributed to obesity [12]. However, there is no robust evidence regarding the social costs of childhood obesity since the associated diseases generally manifest in adulthood, which complicates the assessment. However, it has been reported that the lifetime costs for a 4-year-old child with obesity amount to €75,000, or CLP$82,502,250 [13]. Considering this, it is noteworthy that the Biobío Region shows an obesity prevalence of 35.5%, exceeding the national average of 31.4% [2].
Organizations such as the World Health Organization (WHO), the United Nations Development Program (UNDP) and the Organization for Economic Cooperation and Development (OECD) have worked to reduce obesity in several countries, but in Chile, despite strategies aligned with these objectives, the obesity rate continues to increase [14]. The OECD has noted that implementing new, effective strategies could generate a positive impact on public health and the economy, with significant savings in health expenditure. In Chile, 2.9% of total health expenditure is allocated to obesity, representing 0.8% of the Gross Domestic Product (GDP), suggesting the need for economic evaluations of health strategies, which play a crucial role in transforming the way in which medical challenges are faced and improving the diagnosis and treatment of diseases, aligned with the National Health Strategy to achieve the Health Objectives by 2030 [15].
In terms of known interventions, the Active Brains clinical trial demonstrated that a 20-week exercise program improved cardiometabolic health in children with overweight or obesity [16] and a study by the Autonomous University of Chile concluded that physical activity alone does not reduce the Body Mass Index (BMI) in Latin American children and adolescents, [17] suggesting the need to combine it with dietary interventions. On the other hand, a Cochrane review in 2003 showed that multi-component interventions are beneficial in reducing BMI in children aged 6 to 11 years, [18] and the Bright Bodies Program at the Yale Pediatric Obesity Clinic showed positive results in obese children after 12 months of follow-up, with significant changes in anthropometric and metabolic parameters [19].
The limitations of the TSA support the creation of a new intervention program with a multidisciplinary approach, led by specialized health professionals and designed in a comprehensive and personalized manner, based on the preferences and needs of children and adolescents.
Research objective
Determine the cost-effectiveness of a Children’s Cardiometabolic Rehabilitation (CCMR) program applied in children and adolescents with obesity between 5 and 14 years of age in the commune of Penco-Lirquén.
Method
The efficiency evaluation of an CCMR program for children and adolescents with obesity was developed, aimed at beneficiary users of the Institutional Care Model in Family Health Centers of PHC, in the commune of Penco-Lirquén, Biobío, as a New Health Technology (NHT). A cost-effectiveness economic evaluation design was developed, the sequence of which considers characterizing the demand, defining the supply, carrying out a technical and financial study of the proposal for a five-year projection and evaluating viability based on Net Present Value (NPV) and Internal Rate of Return (IRR). Subsequently, structure, result and process indicators were defined with projections of marginal productivity that allow comparing the cost-effectiveness of the contrasted proposal with the current strategy.
The cost analysis of the current strategy, both for children and adults, considering the expenses involved in the treatment of chronic pathologies derived from obesity, was carried out with data obtained through the transparency law of government organizations, detailing costs by type of service for the population of the National Health Fund or Fondo Nacional de Salud (FONASA) in Chile. The most relevant interventions for the diagnosis and treatment of chronic diseases directly related to obesity in adults were included.
Demand characterization
The Penco-Lirquén commune, according to the 2017 census, has a population of 50,050 inhabitants, with 48.5% men and 51.5% women, and 99.0% urban. The poverty rate is 8.6% and childhood obesity affects 242 children between 5 and 14 years old. The health system includes the Penco and Lirquén Family Health Center (CESFAM), which in 2021 registered 387 admissions to the cardiovascular health program, representing an increase of 74.0% compared to the previous year. Table 1 shows the number of users with chronic pathologies associated with obesity.
Table 1. Users with pathology associated with obesity in Penco-LirquénDiagnosisTotalBoth sexesMenWomenHBP7,6892,9944,695DM23,6841,3902,294DLP3,8421,3582,484Absolute population values 2021
There is a high prevalence of obesity in children, with coverage poorly targeted towards this population. There is also a high incidence of chronic pathologies in adults and little evidence on financial analyses available, due to a low urgency of the problem in the coverage objectives of health teams. In addition, there is a lack of participation and commitment of the target population, the community and health care networks in the use of health technologies aimed at this problem. The current health approach focuses mainly on the treatment of chronic pathologies, without prioritizing prevention or early approach to obesity.
Therefore, a gap is observed in the fulfillment of health objectives with attention to the comprehensive scorecard that regulates the family health and preventive medicine model. Table 2 shows the cost of the current strategy aimed at children and adolescents, while Table 3 shows the costs associated with the benefits demanded by adult users with pathologies attributable to obesity and Table 4 shows the costs associated with the common care demand of healthy adults.
Table 2. Cost of benefits provided to users with pathologies associated with obesityCodeBenefitPrice () by MAI FONASA 2023 Coding
Table 3. Penco-Lirquén user demandDiseaseTypePrice ( UnitaryUsers) 2021
Table 4. Cost of benefits granted to users without pathology associated with obesityCodeBenefitPrice () by MAI FONASA 2023 Coding
The above shows an important difference in the State’s costs when intervening in users who already have pathologies associated with obesity, compared to the costs of common care for healthy users; In addition, the costs associated with the needs of children and adolescent users who access a comprehensive care program when they have risk factors for childhood obesity are considered [20]. This unit cost is like the unit cost of the sick adult population; however, since chronic demand does not occur, the total costs are significantly lower in early intervention.
Definition of the offer
The National Zero Obesity Strategy 2020, promoted by the Health’s Ministry, is based on the Five Circles of Healthy Living, a comprehensive approach that seeks to prevent and reverse obesity in the Chilean population.
These circles are:
- Promotion of healthy eating with access to nutritious foods, policies such as food labeling, educational campaigns and regulation of marketing aimed at children.
- Promotion of physical activity in daily life through community interventions, promotion of school sports and improvements in public infrastructure.
- Mental health care by promoting stress management, self-care and emotional support programs in primary care networks.
- Control of metabolic risk factors, promoting the timely diagnosis and management of metabolic conditions at the primary and secondary care levels.
- Creating healthy environments that facilitate healthy choices, such as access to fresh food, safe environments for recreation and active transportation.
The five pillars work in a coordinated manner to address the social and structural determinants of obesity, with a special focus on the early stages of the life cycle. It is proposed that the offer considered include key elements that address these fundamental pillars of comprehensive well-being and act on the main modifiable determinants of obesity and its comorbidities.
- Healthy eating through nutritional benefits, with a positive impact on weight and metabolic health through a balanced diet that reduces the risk of obesity and chronic diseases. In addition, eating habits are formed at early stages of life, so promoting healthy eating from childhood helps prevent future problems [21].
- Physical activity, which tends to regulate weight and where exercise helps maintain an adequate energy balance, essential to prevent imbalances [22]. The systematic benefits of physical activity go beyond weight control, as it improves cardiovascular health, reduces the risk of several types of cancer and strengthens the musculoskeletal system. Given the increasing sedentary lifestyle associated with office work, the use of technology and motorized transport, promoting movement is more crucial than ever [23].
- Mental health, with its bidirectional relationship with obesity, since it can contribute to the development of psychological disorders such as anxiety and depression, while these, in turn, can lead to unhealthy behaviors such as overeating or a sedentary lifestyle. Strengthening self-care and emotional well-being is essential to adopting and maintaining lifestyle changes. Programs that promote emotional resilience and stress management increase adherence to healthy lifestyles. However, social and economic challenges, such as poverty or job insecurity, can negatively influence health-related decision-making [24].
These three elements act in synergy, affecting not only body weight, but also quality of life and the prevention of various diseases. An Internal and External Factors Evaluation Matrix of the current strategy was carried out to identify key points susceptible to improvement, as shown in Table 5. Success factors include the availability of multidisciplinary professionals and a comprehensive care program, while factors influencing failure are low urgency and weak financial analysis in technological innovation. The Matrix was constructed through a SWOT analysis, where the weights and ratings of each factor were determined through the consensus of the research team, ensuring a systematic weighting based on the Hanlon model.
Table 5. Factor evaluation matrix for the current intervention strategy in obesityMatrixFactorWightQualificationWeighingExternalMultidisciplinary teams that exist in the community0.25010.250Gap in the design and implementation of new health projects0.07520.150Problem of interest in WHO strategic guidelines0.20040.800Resources for new health intervention strategies0.10010.100Sustained increase in the prevalence ofchronic diseases in the population0.07530.225Low sense of urgency of the problem within the coverage objectives0.10020.200Lack of participation and commitment of the target population0.12520.250Health approach aimed at treatment and not prevention0.07530.225InternalExistence of a health strategy and devices in the community0.25041.000Availability of updated literatureregarding the problem under study0.05030.150Public policies between sectors withprogressive development0.12540.500Increased social and political interest inquality of life of people0.25030.750High prevalence of children and adolescents with obesity in the commune0.10020.200Deficit in health technologies with a focus on the obese child population0.07510.075High prevalence of chronic pathologies in the adult population in the commune0.10010.100Weakness in financial analysisavailable with respect to the strategy0.05010.050The matrix originates from an analysis of current strengths, opportunities, weaknesses and threats
Therefore, it is proposed to evaluate the strategy considering the characteristics of the demand and the purpose of delivering an intervention plan that includes accessible and attractive tools to address obesity in children and adolescents, through comprehensive services from health professionals, including general practitioners, kinesiologists, nutritionists and psychologists, who will focus on the personalized approach to physical activity, [25] nutrition and behavior, [17] adapting to the individual needs and preferences of each user [26].
Feasibility study
The creation of a comprehensive program in the Penco-Lirquén commune is proposed, adapted to local needs and financed through Primary Care Reinforcement Programs. This program includes the implementation of a Comprehensive Treatment Center in a residential home that meets the necessary health requirements, focusing on children and adolescents from 5 to 14 years old and projected to 5 years according to recommendations of the Ministry of Health.
The technical study evaluated the necessary resources using data on the prevalence of childhood obesity in the region. Tangible and intangible assets essential for the operation of the center were identified, applying a Linear Depreciation method to estimate their value over 5 years and calculating the Commercial Residual Value of the fixed assets.
This feasibility study seeks to ensure the sustainability and efficiency of the center in the intervention of childhood obesity in the community. The analyses in Table 6 indicate a positive Net Present Value (NPV), which concludes that the project is economically viable, with an Internal Rate of Return (IRR) of 13%, thus recommending the execution of the project.
Table 6. Synthesis of the technical and financial study of the NHT proposalAssetsTotal Value ()Amortization ($)Fixed asset17,540,6512,280,824---Nominal asset289,200---289,200 Item
Amounts Investment ()108.828,862Variable cost ()646,440^1^6,269,534^2^6,440,656^3^6,436,402^4^6,527,034^5^Annual income ()106,496,940Expenses ()215,480^0^226,900^1^238,926^2^251,589^3^264,923^4^Accumulated depreciation ()6,136,531Scrap value commercial ()14,461,539 **Period** **T** ^**0**^ **T** ^**1**^ **T ** ^2^ **T** ^**3**^**T** ^**4**^**T** ^**5**^Flow ()−18,260,811−1,435,608−1,420,7052,792,4847,336,31126,820,787NPV$3,022,387IRR13%Superscript indicates the value applied to period T of the TSN project application
Organizational study
The organizational study focused on defining the team of professionals that will make up the Comprehensive Treatment Center, determining its administrative structure and the work plans necessary for its operation. It is considered for this:
- Fixed Cost: Remunerations, basic services, maintenance and supplies.
- Variable Cost: Training, replacement coverage and extra-programmatic activities.
- Income: Comes from the benefits included in the CCRM basket.
- Expenses: Related to the operation and production of services in the health center.
- Working Capital: Initially CLP$587,545 was calculated, with reinvestment projections.
- Pure Flow: Projection of income and expenses generated by the project over 5 years.
- Feasibility: The NPV is positive, and the IRR is estimated at 13%.
Finally, to identify the efficiency of the comprehensive RCMI program, the costs of the CHT and NHT were analyzed, adjusted to the characterization of the users of the commune of Penco-Lirquén. In addition, structure, process and result indicators were built with the objective of determining the effectiveness of the proposal presented.
According to the evidence collected, it is estimated that 44% of BGA with obesity will be obese adults prone to developing DM2, HBP and DLP; while the remaining 56% will eventually become a healthy adult whose care basket, unlike the obese group, will only incorporate PME. The health cost attributable to CHT and NHT available for both children and adults is shown in Table 7. The above can be analyzed considering the projection of the 44% probability of being an obese adult, representing the unit costs associated with each health technology, in adults and children, as shown in Fig. 1.
Table 7. Unit costs associated with healthcare demand for each strategyCHTNHTAdultDisease Cost ()25,70025,700BGATotal cost162,388440,070There is no cost associated with adults on NRT since the pathological condition is prevented
Fig. 1. Unit costs according to healthcare technology in CLPM = Thousands of Chilean pesos) for the adult population decrease while those for the child population increase when incorporating the new strategy proposed as a preventive intervention, which subsequently translates into long-term savings by avoiding chronic diseases in adulthood
In the commune of Penco-Lirquén the total number of children and adolescents diagnosed with obesity corresponds to 242 users, therefore, it is projected that 106 of them will become obese adults. When applying the costs to this population, the values are shown in Table 8 and represented in Fig. 2.
Table 8. Total costs associated with healthcare demand for each strategyCHTNHT Total TotalAdultDisease160,24410616,985,854---------PME25,7001363,495,20025,7002426,219,400BGACCMR162,38824239,297,896440,070242106,496,940Total ($)59,778,960There is no cost associated with adults on NRT since the pathological condition is prevented
Fig. 2. Total costs according to health technology in CLPMM = Millions of Chilean pesos) for the adult population decrease while those for the child population increase when incorporating the new strategy proposed as a preventive intervention, which implies long-term savings by avoiding chronic diseases in adulthood
Given the above, it is suggested that NHT has a higher cost than CHT, however it is necessary to relate other epidemiological data of the commune that guides regarding the impact of these costs sustained over time. In this sense, in the commune of Penco-Lirquén the largest expenditure for the treatment of chronic pathologies occurs when intervening on users with DM2, reaching an estimated value of CLP$267,178,956 annually. In addition to this, this disease constitutes a history that increases cardiovascular risk and is associated with multiple complications, significantly affecting the quality of life of those who suffer from it [27, 28].
Project indicators
The project included a series of indicators to evaluate the efficiency and impact of health technologies in the treatment of metabolic conditions and human development in the Penco-Lirquén commune.
Regarding the cost relationship of health technologies
Life expectancy in Chile, for people diagnosed with DM2 on average at age 47, is 79.5 years. Patients with DM2 have a life expectancy of 26.5 years after diagnosis, compared to 32.5 years for those without diabetes. When adjusting the costs of each TS according to life expectancy, it was found that NHT has a cost of 0.51 times that of CHT, indicating significant savings, as represented in Fig. 3, serving as a structure indicator.
Fig. 3. Unit costs adjusted according to health technology in CLPM represents thousands of Chilean pesos
Percentage of variation in the human development index (HDI)
The HDI, which evaluates health, education and standard of living, allows development in countries to be measured in a global comparison. Given that the effects of metabolic diseases associated with obesity decrease life expectancy, the application of NHT compared to CHT shows an increase of 0.585% in the HDI, evidencing an improvement in human development when implementing the new technology, serving as a result indicator as detailed in Table 9 and represented in Fig. 4.
Table 9. Calculation of HDI attributable to the intervened population for both strategiesVariablesCHTNHTLife expectancy78.979.6Expected years of schooling16.716.7Average years of schooling10.910.9GDP per capita PPP24,56324,563HDI0.8550.860The variation in schooling and productivity attributable to obesity has not been considered
Fig. 4. Projection of cost-effectiveness between both strategies. The cost-effectiveness analysis shows that, from the beginning without intervention on the sick population (WHT), CHT has almost double the cost than NHT, while achieving a lower life expectancy as an effect. The graph shows that NHT is more cost-effective than CHT
Percentage of referral of users to the program
This indicator is designed to evaluate the inclusion of users in the RRCM program; however, it has not yet been able to be calculated because the program has not been implemented. It is recommended to perform this calculation monthly once the program is in operation to record the derivations and propose improvements, so that it can be used as a process indicator.
These indicators will allow us to measure the impact of the Comprehensive Center on the health of the child and adult population, as well as its contribution to human development in the region. The details of the construction of the indicators are presented in Table 10.
Table 10. Proposed indicators for the evaluation of the strategyIndicator titleHT cost ratioPurposeDetermine the cost ratio achieved by projecting the years of life of users with DM2 in relation to the population without this morbidityTypeStructureFormula \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\frac{NHT\ Cost}{CHT\ Cost}$$\end{document} Data sourceNational Health Survey – Local Statistical RegistryThreshold>0PeriodicityAnnualMethodologyRandom samplingResponsibleDirector – Health Service ReferenceObservations---Indicator titlePercentage of HDI variationPurposeCompare the HDI without and with CCMR based on life expectancy due to early risk factor interventionTypeResultFormula \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\frac{(HDI\ NHT - HDI\ CHT)\times 100}{HDI\ CHT}$$\end{document} Data sourceNational Health Survey - Central BankThreshold>0%PeriodicityAnnualMethodologyRandom samplingResponsibleDirector – Health Service ReferenceObservations---Indicator titleReferral ratio of users entering NHTPurposeMeasure user referrals from PHC according to the criteria established in the programTypeProcessFormula \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\frac{BGA\ Number\ with\ entry\ criteria\ reffered\ to\ NHT}{Total\ Number\ BGA\ with\ admission\ criteria\ attended\ to\ in\ PHC}$$\end{document} Data sourceStatistics Department of the Ministry of HealthThreshold0,8PeriodicityMonthlyMethodologyPopulationResponsibleLiaison ManagerObservations---
Discussion
The results obtained in this research underscore the urgent need to address childhood obesity in Chile, whose prevalence exceeds the OECD average. The limited effectiveness of current health technologies, evidenced by an 8% adherence rate in 2022, highlights the demand for more personalized and preventative approaches. In this context, the intervention strategy based on New Health Technologies (NHT) emerges as an innovative proposal, with a comprehensive approach that incorporates the active participation of health professionals.
The economic viability of NHT, reflected in a positive Net Present Value and an Internal Rate of Return greater than 10%, justifies its implementation despite a higher initial cost. This model demonstrates that investment in prevention and personalization generates long-term economic and social benefits, such as a reduction in comorbidities, increased life expectancy, and a favorable impact on the Human Development Index (HDI). NHT differentiates itself from Legacy Health Technologies (LHT) by offering personalized sessions, complementary activities—such as workshops and excursions—and the active inclusion of the family in the cardiometabolic rehabilitation process, with the collaboration of a multidisciplinary team composed of physicians, physical therapists, nutritionists, and psychologists.
The projected impact of the NHT on the HDI and life expectancy highlights its transformative potential for public health, positioning Chile as a regional benchmark. However, to maximize these benefits, it is essential to ensure the strategy’s sustainability through robust public policies that ensure ongoing funding, professional training, and systematic monitoring of results.
Limitations
Among the main limitations of the study is the nature of the cost data, as publicly available data were used, without considering possible variations in market costs. Furthermore, the results depend on certain assumptions used in the projections, such as the estimate that 44% of children with obesity will remain obese into adulthood. There could also be an underestimation of indirect costs, for example, the productivity losses of parents when accompanying their children to appointments. Furthermore, the findings have limited generalizability to other municipalities or regions with different socioeconomic characteristics.
The study is also limited by the lack of longitudinal and actual follow-up data, given that the program has not yet been implemented. Furthermore, possible variations in financing or operating costs, as well as qualitative aspects such as user adherence or satisfaction, which could influence the program’s effectiveness, were not considered.
Conclusion
The economic evaluation of early intervention for childhood obesity in the Penco-Lirquén commune demonstrates the importance of urgently addressing this problem in Chile. The results confirm that implementing NRT is economically viable and has the potential to significantly improve the human development and life expectancy of the affected population.
The cost-effectiveness ratio, with NHT being superior to CHT, indicates that adopting NHT represents an efficient strategy for optimizing health system resources. Furthermore, the implementation of NHT has demonstrated a 0.585% increase in the HDI, reflecting improvements in health, education, and living standards indicators. This demonstrates that the fight against childhood obesity transcends the health sector to positively impact regional social and economic development.
The NHT-based strategy, which integrates the collaboration of physical therapists, nutritionists, and psychologists, emphasizes the importance of a comprehensive and personalized approach. This model not only focuses on treatment but also involves families and promotes sustainable behavioral changes, key factors for long-term effectiveness.
To optimize results, it is essential to ensure the sustainability of the model through public policies that guarantee ongoing funding, adequate professional training, and an effective monitoring system. Collaboration between the public and private sectors can strengthen this strategy and facilitate its successful implementation.
Finally, we recommend that future research evaluate the adaptability of NHT in various contexts and populations, as well as the relationship between family interventions and long-term adherence. These studies will allow for the strategy to be adjusted and strengthened, expanding its impact on public health both nationally and internationally.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1IPSOS CHILE. Encuesta Nacional de Salud 2023. Vol.1. Universidad Andrés Bello, 2023 https://www.ispandresbello.cl/wp-content/uploads/2023/10/encuesta-nacional-de-salud-2023-informe-general.pdf
- 2Subsecretaría de Salud Pública. Encuesta Nacional de Salud 2016–2017. Gobierno de Chile, 2017 https://www.minsal.cl/wp-content/uploads/2017/11/ENS-2016-17_PRIMEROS-RESULTADOS.pdf
- 3Strain H, Becerra C, Castillo C, Leyton B, Santander S. Norma Técnica para la supervisión de niños y niñas de 0 a 9 años en la Atención Primaria de Salud. 2014. https://www.minsal.cl/sites/default/files/files/2014_Norma%20T%C 3%A 9cnica%20para%20la%20supervisi%C 3%B 3n%20de%20ni%C 3%B 1os%20y%20ni%C 3%B 1as%20de%200%20a%209%20en%20APS_web(1).pdf.
- 4Ministerio de Salud. Orientaciones técnicas para el control de salud integral de adolescentes. 2021. https://diprece.minsal.cl/wp-content/uploads/2022/11/OT-Control-Adolescente-v 3.pdf
- 5Ministerio de Salud. Guía Examen Med Preventiva. Vol. 1. 2008. https://www.superdesalud.gob.cl/difusion/665/articles-974_guia.pdf
- 6Ministerio de Salud. Orientaciones técnicas Programa de Salud Cardiovascular. 2017. http://www.repositoriodigital.minsal.cl/bitstream/handle/2015/862/OT-PROGRAMA-DE-SALUD-CARDIOVASCULAR_05.pdf
- 7Ministerio de Salud. Guía Clínica Diabetes Mellitus Tipo 2. 2009. https://www.ssmso.cl/protocolos/Guia Diabetes II 2009.pdf
- 8Ministerio de Salud. Hipertensión Arterial Primaria o Esencial en personas de 15 años y más. 2006. https://www.ssmso.cl/protocolos/Guia HTA.pdf