Serous Ovarian Cancer Following Opportunistic Bilateral Salpingectomy
Ramlogan Sowamber, Alice J. Mei, Paramdeep Kaur, Julianne McLeod, Emily McKay, Alex Lukey, Jamie Bakkum-Gamez, Natalia Buza, Paul A. Cohen, Kyle Devins, Rhonda Farrell, Christine Garcia, Blake Gilks, Ellen Goode, Anjelica Hodgson, Brooke Howitt, Pei Hui, Jutta Huvila

TL;DR
This study examines how opportunistic bilateral salpingectomy in Canada affects the risk of high-grade serous ovarian cancer.
Contribution
The study provides empirical evidence on the impact of salpingectomy on serous ovarian cancer risk in a Canadian cohort.
Findings
Opportunistic bilateral salpingectomy is associated with a reduced risk of high-grade serous carcinoma.
The procedure may serve as an effective preventive strategy for ovarian cancer in women undergoing pelvic surgery.
Abstract
This cohort study evaluates the reduction in risk of high-grade serous carcinoma among women undergoing opportunistic bilateral salpingectomy in Canada.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure
Figure| Factor | Participants, No. (%) | SMD | |
|---|---|---|---|
| Comparator surgery (n = 45 296) | OBS (n = 40 527) | ||
| Age at surgery, mean (SD) | 42.4 (12.6) | 40.7 (8.1) | 0.16 |
| Follow-up, median (IQR), y | 8.45 (6.07-11.51) | 4.72 (2.23-7.09) | 1.11 |
| Income quintile | |||
| 1 (lowest 20%) | 8709 (20.1) | 7191 (18.3) | 0.07 |
| 2 | 9163 (21.1) | 7856 (20.0) | |
| 3 | 8784 (20.3) | 7981 (20.3) | |
| 4 | 8591 (19.8) | 8416 (21.4) | |
| 5 (highest 20%) | 7470 (17.2) | 7533 (19.2) | |
| Missing | 656 (1.2) | 354 (0.90) | |
| Parity, live births, mean (SD) | 1.98 (1.1) | 1.91 (1.0) | 0.06 |
| No. of pregnancies, mean (SD) | 2.41 (1.5) | 2.32 (1.4) | 0.07 |
| OCP use | 21 665 (50.0) | 23 876 (60.7) | 0.22 |
| OCP duration, mean (SD), days | 1085 (1230) | 1322 (1465) | 0.18 |
| Endometriosis | 4460 (9.9) | 5251 (13.0) | 0.09 |
| Serous ovarian cancer | |||
| No. of person years | 370 133 | 189 101 | NA |
| Cancer events | 21 | ≤5 | NA |
| Breast | |||
| No. of person years | 368 138 | 188 418 | NA |
| Cancer events | 492 | 218 | NA |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOvarian cancer diagnosis and treatment · Menopause: Health Impacts and Treatments · Endometrial and Cervical Cancer Treatments
Introduction
Ovarian carcinoma is a heterogeneous disease with a 5-year survival rate below 50%.^1^ Primary prevention of the most common histotype of ovarian carcinoma (high-grade serous carcinoma [HGSC], 70% of ovarian carcinomas) is possible using opportunistic bilateral salpingectomy (OBS; the removal of the fallopian tubes during another pelvic surgery while conserving the ovaries). Significant data show that OBS is safe,^2^ it does not appear to reduce the age of onset of menopause,^3^ and it is cost-effective.^4^ Herein, this evidence base is expanded by (1) estimating the risk reduction for serous ovarian cancer afforded by OBS using population-based data; and (2) examining whether the histotype distribution of ovarian carcinomas in people without fallopian tubes significantly differs from the historical histotype distribution.
Methods
For the first aim, we conducted a population-based retrospective cohort study including all people who underwent a hysterectomy or tubal permanent contraception in British Columbia between 2008 and 2020 (eTable 1 and eTable 2 in Supplement 1), with approval from the University of British Columbia’s clinical research ethics board and a waiver of consent due to use of deidentified data. We followed Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines. Risk reduction for serous carcinomas from the population-based data was estimated using Cox proportional hazards models comparing individuals in the OBS group with individuals in the comparison surgery group (hysterectomy alone or tubal ligation). Low- and high-grade serous carcinomas were combined as our data did not specify histotype among serous carcinomas, but HGSC represent 95% of these carcinomas. We repeated the analysis with breast cancer as the outcome to examine the likelihood of selection bias on important unmeasurable differences between the groups (see eMethods in Supplement 1).
For the second aim, we asked international pathologists to enter anonymized data into a RedCap database for any ovarian carcinomas occurring in a patient without fallopian tubes (eTable 2 in Supplement 1). The histotype distribution of these cancers was compared with a historical histotype distribution using Fisher exact test.^5^ All P values were 2-sided, and statistical significance was defined as P < .05 for all analyses, which were performed in SAS version 9.4 (SAS Institute) and Stata version 19 (StataCorp) from April 2025 to October 2025.
Results
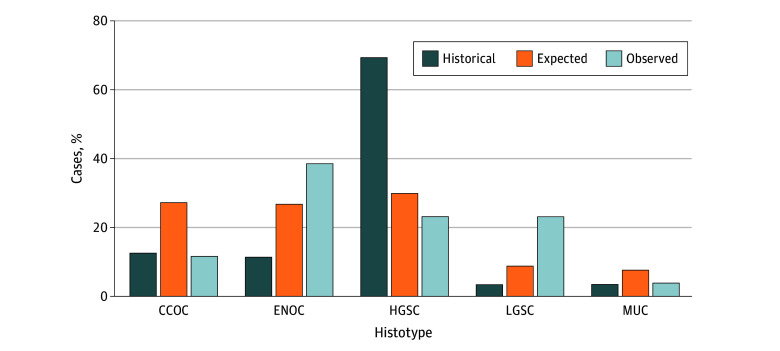
In aim 1, there were 85 823 patients who had surgical procedures of interest, 40 527 who underwent OBS (median [IQR] follow-up, 4.72 [2.23-7.09] years), and 45 296 who underwent a comparator surgery (median [IQR] follow-up, 8.45 [6.07-11.51] years). Compared with those who underwent OBS, individuals in the comparison group were older at the time of surgery (mean [SD] age, 42.4 [12.6] vs 40.7 [8.1] years) and had less use of oral contraceptive pills (21 665 individuals [50.0%] vs 23 876 [60.7%]; mean [SD] use, 1322 [1465] vs 1085 [1230] days) (Table). The crude hazard ratio for serous ovarian carcinoma was 0.22 (95% CI, 0.05-0.95); for breast cancer, it was 0.99 (95% CI, 0.84-1.17). For aim 2, 26 ovarian carcinomas were identified in individuals without fallopian tubes, with only 6 of 26 (23.1%) being HGSC compared with 642 of 942 (68.1%) in a historical cohort with fallopian tubes (Fisher exact test, P < .001) (Figure).^5^
Histotype Distribution Following a Bilateral Salpingectomy in the Cases Entered Into the RedCap DatabaseThe dark blue bars represent the historical distribution of ovarian cancers in women who have not had an opportunistic bilateral salpingectomy, as determined by Kobel et al.5 The orange bars represent the expected numbers of ovarian cancers following a hypothetical application of an 80% reduction to the high-grade serous carcinoma histotype. The light blue bars indicate the actual observed ovarian cancers from patients who had undergone bilateral salpingectomy. The high-grade serous carcinoma (HGSC) histotype was significantly decreased in the observed cohort (23.1% of ovarian cancer cases) following bilateral salpingectomy compared with the historical histotype distribution of HGSC (68.1% of all ovarian carcinoma cases). Fisher exact test, P < .001. CCOC indicates clear cell ovarian carcinoma; ENOC, endometrioid ovarian carcinoma; LGSC, low-grade serous carcinoma; MUC, mucinous ovarian cancer.
Discussion
In this expanded analysis of health care and cancer data from British Columbia, we add to preliminary evidence of effectiveness of OBS^6^ as individuals who underwent OBS were at nearly 80% reduced risk for serous ovarian cancers compared with those who had a hysterectomy alone or tubal ligation. Our second aim showed significantly fewer HGSCs in people without fallopian tubes compared with the historical histotype distribution for ovarian carcinoma.
Limitations include that many of these surgical procedures occurred in people well below the age of peak risk for HGSC, which resulted in a small number of ovarian carcinomas. This meant we could not control for all possible confounders in the Cox proportional hazards models. Nonetheless, these findings provide robust support for the effectiveness of OBS as a preventive intervention and underscore that broader implementation of OBS has the potential to significantly reduce the incidence and mortality of serous ovarian carcinoma.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cronin KA, Lake AJ, Scott S, . Annual report to the nation on the status of cancer, part I: national cancer statistics. Cancer. 2018;124(13):2785-2800. doi:10.1002/cncr.3155129786848 PMC 6033186 · doi ↗ · pubmed ↗
- 2Strandell A, Magarakis L, Sundfeldt K, Pålsson M, Liv P, Idahl A. Salpingectomy versus tubal occlusion in laparoscopic sterilisation (SALSTER): a national register-based randomised non-inferiority trial. Lancet Reg Health Eur. 2024;45:101026. doi:10.1016/j.lanepe.2024.10102639974774 PMC 11838100 · doi ↗ · pubmed ↗
- 3Hanley GE, Kwon JS, Mc Alpine JN, Huntsman DG, Finlayson SJ, Miller D. Examining indicators of early menopause following opportunistic salpingectomy: a cohort study from British Columbia, Canada. Am J Obstet Gynecol. 2020;223(2):221 e 1-221 e 11. doi:10.1016/j.ajog.2020.02.00532067967 · doi ↗ · pubmed ↗
- 4Kwon JS, Mc Alpine JN, Hanley GE, . Costs and benefits of opportunistic salpingectomy as an ovarian cancer prevention strategy. Obstet Gynecol. 2015;125(2):338-345. doi:10.1097/AOG.000000000000063025568991 · doi ↗ · pubmed ↗
- 5Köbel M, Kalloger SE, Huntsman DG, ; Cheryl Brown Ovarian Cancer Outcomes Unit of the British Columbia Cancer Agency, Vancouver BC. Differences in tumor type in low-stage versus high-stage ovarian carcinomas. Int J Gynecol Pathol. 2010;29(3):203-211. doi:10.1097/PGP.0b 013e 3181 c 042b 620407318 · doi ↗ · pubmed ↗
- 6Hanley GE, Pearce CL, Talhouk A, . Outcomes from opportunistic salpingectomy for ovarian cancer prevention. JAMA Netw Open. 2022;5(2):e 2147343. doi:10.1001/jamanetworkopen.2021.4734335138400 PMC 8829665 · doi ↗ · pubmed ↗