Adjuvant radiotherapy for patients with clinical T3–4 oral and oropharyngeal cancer who achieved major pathologic response after neoadjuvant immunochemotherapy and surgery: a propensity score-matched retrospective study
Menghua Li, Shiyan Yang, Lili Liu, Wanming Hu, Shida Yan, Yani Zhang, Mingyuan Du, Xianlu Gao, Chulin Yang, Liji Zheng, Chunyan Chen, Jian Zhou, Jiabin Lu, Ming Song, Shuwei Chen

TL;DR
This study finds that skipping adjuvant radiotherapy after surgery and treatment for advanced oral and oropharyngeal cancer leads to worse outcomes.
Contribution
The study uses propensity score matching to show that adjuvant radiotherapy improves survival outcomes in patients with major pathologic response.
Findings
Adjuvant radiotherapy significantly improved local and locoregional recurrence-free survival.
Omitting radiotherapy did not improve distant metastasis-free or overall survival.
Benefits of radiotherapy were maintained in patients with ypT0–2 tumors.
Abstract
Neoadjuvant chemotherapy combined with immunotherapy results in high pathologic response rates in locally advanced oral and oropharyngeal cancer (OC/OPC). It is unclear if patients with clinical T3-4 (cT3-4) OC/OPC at initial diagnosis can safely omit adjuvant radiotherapy (ART) after significant pathological downstaging. This retrospective cohort study included cT3–4 OC/OPC patients who achieved a major pathologic response (MPR) after neoadjuvant immunochemotherapy between July 2019 and May 2024. Patients were categorized by whether they received ART. Propensity score matching was used to balance baseline characteristics. Local recurrence-free survival (LRFS), locoregional recurrence-free survival (LRRFS), distant metastasis-free survival (DMFS), and overall survival (OS) were compared between cohorts. A total of 247 patients were eligible, with a median follow-up of 31 months (IQR,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
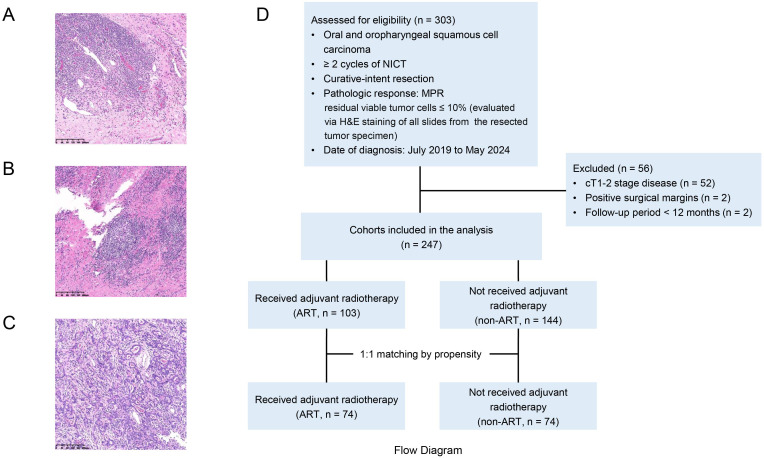 Figure 1
Figure 1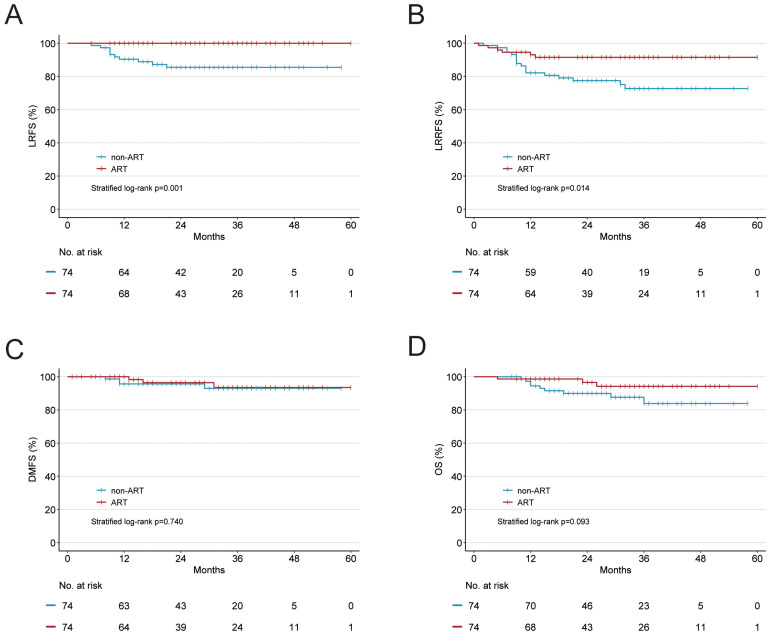 Figure 2
Figure 2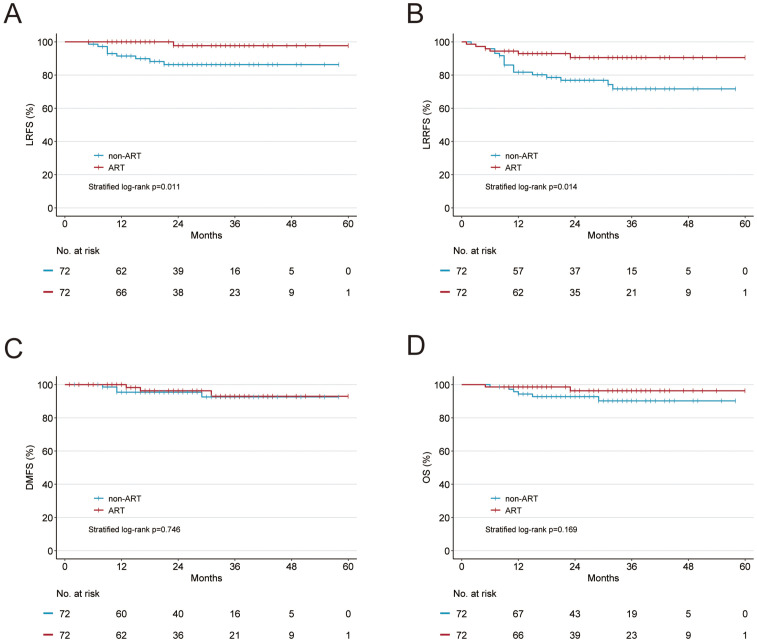 Figure 3
Figure 3| Characteristic | Before PSM | After PSM | ||||||
|---|---|---|---|---|---|---|---|---|
| Overall, n=247 | Non-ART, n=144 | ART, n=103 |
| Overall, n=148 | Non-ART, n=74 | ART, n=74 |
| |
| Sex, No. (%) | 0.739 | 0.834 | ||||||
| Male | 202 (81.8) | 119 (82.6) | 83 (80.6) | 120 (81.1) | 61 (82.4) | 59 (79.7) | ||
| Female | 45 (18.2) | 25 (17.4) | 20 (19.4) | 28 (18.9) | 13 (17.6) | 15 (20.3) | ||
| Age, years | 0.015 | 0.82 | ||||||
| Median (IQR) | 54 (46-64) | 57 (48-64) | 51 (44-60) | 53 (45-60) | 53 (45-60) | 52 (45-61) | ||
| Tobacco use, No. (%) | 0.330 | 0.718 | ||||||
| No | 171 (69.2) | 96 (66.7) | 75 (72.8) | 105 (70.9) | 51 (68.9) | 54 (73.0) | ||
| Yes | 76 (30.8) | 48 (33.3) | 28 (27.2) | 43 (29.1) | 23 (31.1) | 20 (27.0) | ||
| Tumor site, No. (%) | 0.739 | 1 | ||||||
| Oral cavity | 185 (74.9) | 106 (73.6) | 79 (76.7) | 112 (75.7) | 56 (75.7) | 56 (75.7) | ||
| p16- Oropharynx | 25 (10.1) | 16 (11.1) | 9 (8.7) | 13 (8.8) | 6 (8.1) | 7 (9.5) | ||
| p16+ Oropharynx | 37 (15.0) | 22 (15.3) | 15 (14.6) | 23 (15.5) | 12 (16.2) | 11 (14.9) | ||
| Histologic grade, No. (%) | 0.301 | 0.503 | ||||||
| Poor | 57 (23.1) | 31 (21.5) | 26 (25.2) | 33 (22.3) | 19 (25.7) | 14 (18.9) | ||
| Moderate | 112 (45.3) | 62 (43.1) | 50 (48.5) | 76 (51.4) | 38 (51.4) | 38 (51.4) | ||
| Well | 78 (31.6) | 51 (35.4) | 27 (26.2) | 39 (26.4) | 17 (23.0) | 22 (29.7) | ||
| cT, No. (%) | 0.897 | 0.322 | ||||||
| T3 | 108 (43.7) | 62 (43.1) | 46 (44.7) | 67 (45.3) | 30 (40.5) | 37 (50.0) | ||
| T4a | 139 (56.3) | 82 (56.9) | 57 (55.3) | 81 (54.7) | 44 (59.5) | 37 (50.0) | ||
| cN, No. (%) | 0.001 | 0.225 | ||||||
| N0 | 119 (48.2) | 80 (55.6) | 39 (37.9) | 79 (53.4) | 42 (56.8) | 37 (50.0) | ||
| N1 | 29 (11.7) | 21 (14.6) | 8 (7.8) | 17 (11.5) | 10 (13.5) | 7 (9.5) | ||
| N2 | 95 (38.5) | 42 (29.2) | 53 (51.5) | 49 (33.1) | 22 (29.7) | 27 (36.5) | ||
| N3 | 4 (1.6) | 1 (0.7) | 3 (2.9) | 3 (2.0) | 0 (0) | 3 (4.1) | ||
| ypT, No. (%) | 0.284 | 1 | ||||||
| T0 | 168 (68.0) | 99 (68.8) | 69 (67.0) | 106 (71.6) | 53 (71.6) | 53 (71.6) | ||
| T1 | 56 (22.7) | 33 (22.9) | 23 (22.3) | 32 (21.6) | 16 (21.6) | 16 (21.6) | ||
| T2 | 17 (6.9) | 11 (7.6) | 6 (5.8) | 8 (5.4) | 4 (5.4) | 4 (5.4) | ||
| T3 | 3 (1.2) | 1 (0.7) | 2 (1.9) | 2 (1.4) | 1 (1.4) | 1 (1.4) | ||
| T4 | 3 (1.2) | 0 (0.0) | 3 (2.9) | |||||
| ypN, No. (%) | < 0.001 | 1 | ||||||
| N0 | 186 (75.3) | 127 (88.2) | 59 (57.3) | 117 (79.1) | 59 (79.7) | 58 (78.4) | ||
| N1 | 35 (14.2) | 12 (8.3) | 23 (22.3) | 23 (15.5) | 11 (14.9) | 12 (16.2) | ||
| N2 | 24 (9.7) | 5 (3.5) | 19 (18.4) | 8 (5.4) | 4 (5.4) | 4 (5.4) | ||
| N3 | 2 (0.8) | 0 (0.0) | 2 (1.9) | |||||
| NICT cycles, No. (%) | 0.471 | 0.499 | ||||||
| 2 cycles | 65 (26.3) | 42 (29.2) | 23 (22.3) | 36 (24.3) | 21 (28.4) | 15 (20.3) | ||
| 3 cycles | 158 (64.0) | 88 (61.1) | 70 (68.0) | 92 (62.2) | 43 (58.1) | 49 (66.2) | ||
| ≥4 cycles | 24 (9.7) | 14 (9.7) | 10 (9.7) | 20 (13.5) | 10 (13.5) | 10 (13.5) | ||
| Pathologic response, No. (%) | 0.680 | 1 | ||||||
| PCR | 169 (68.4) | 100 (69.4) | 69 (67.0) | 106 (71.6) | 53 (71.6) | 53 (71.6) | ||
| Non-PCR | 78 (31.6) | 44 (30.6) | 34 (33.0) | 42 (28.4) | 21 (28.4) | 21 (28.4) | ||
| PNI, No. (%) | 0.164 | 1 | ||||||
| No | 242 (98.0) | 143 (99.3) | 99 (96.1) | 147 (99.3) | 74 (100) | 73 (98.6) | ||
| Yes | 5 (2.0) | 1 (0.7) | 4 (3.9) | 1 (0.7) | 0 (0) | 1 (1.4) | ||
| LVI, No. (%) | 0.417 | 1 | ||||||
| No | 246 (99.6) | 144 (100) | 102 (99.0) | 148 (100) | 74 (100) | 74 (100) | ||
| Yes | 1 (0.4) | 0 (0.0) | 1 (1.0) | 0 | 0 | 0 | ||
| LNY, No. (%) | 0.216 | 1 | ||||||
| ≤ 18 | 78 (31.6) | 50 (34.7) | 28 (27.2) | 53 (35.8) | 27 (36.5) | 26 (35.1) | ||
| > 18 | 169 (68.4) | 94 (65.3) | 75 (72.8) | 95 (64.2) | 47 (63.5) | 48 (64.9) | ||
| Adjuvant therapy, No. (%) | ||||||||
| non-ART | 144 (58.3) | 74 (50.0) | ||||||
| PD-1 maintenance | 31 (12.6) | 18 (12.2) | ||||||
| ART | 103 (41.7) | 74 (50.0) | ||||||
| Variable | Non-ART | ART |
|
|---|---|---|---|
| Whole cohort | |||
| 2-year LRFS | 91.8 | 97.4 | 0.140 |
| 2-year LRRFS | 83.3 | 87.4 | 0.227 |
| 2-year DMFS | 96.7 | 93.8 | 0.240 |
| 2-year OS | 92.7 | 93.4 | 0.963 |
| PSM cohort | |||
| 2-year LRFS | 85.5 | 100 | 0.001 |
| 2-year LRRFS | 77.5 | 91.5 | 0.014 |
| 2-year DMFS | 95.6 | 96.4 | 0.740 |
| 2-year OS | 90 | 96.5 | 0.093 |
| ypT0–2 PSM cohort | |||
| 2-year LRFS | 86.3 | 97.7 | 0.011 |
| 2-year LRRFS | 76.9 | 90.5 | 0.014 |
| 2-year DMFS | 95.5 | 96.3 | 0.746 |
| 2-year OS | 92.8 | 96.3 | 0.169 |
| Late adverse effect | ART (n = 103) | ||
|---|---|---|---|
| Grade 3 | Grade 4 | Grade 5 | |
| Skin | 3 | 1 | 0 |
| Mucous membrane | 7 | 1 | 0 |
| Subcutaneous tissue | 2 | 0 | 0 |
| Salivary gland | 2 | 0 | 0 |
| Pharynx/esophagus | 4 | 0 | 0 |
| Larynx | 0 | 0 | 0 |
| Lung | 0 | 0 | 1 |
| Spinal cord | 0 | 0 | 0 |
| Bone | 1 | 1 | 0 |
| Joint | 0 | 0 | 0 |
| Brain | 0 | 0 | 0 |
| Other neurologic | 1 | 0 | 0 |
| Hematologic | 0 | 1 | 0 |
| Renal | 0 | 0 | 0 |
| Total | 20 (19.4) | 4 (3.9) | 1 (1.0) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHead and Neck Cancer Studies · Esophageal Cancer Research and Treatment · Gastric Cancer Management and Outcomes
Introduction
About two-thirds of patients with head and neck squamous cell carcinoma (HNSCC) have locally advanced disease, requiring multimodal management (1, 2). Adjuvant radiotherapy (ART) reduces the risk of locoregional recurrence, distant metastasis, and mortality in patients with locally advanced oral and oropharyngeal squamous cell carcinoma (OC/OPC) after radical surgical resection (3). These benefits are most pronounced in patients with two or more regional lymph nodes (LNs) involved, extracapsular spread of disease, positive surgical margins, perineural invasion (PNI), lymphovascular invasion (LVI), and T3–4 disease (4–6).
Neoadjuvant therapy reduces tumor burden and may enable organ preservation. Prospective clinical trials have shown that neoadjuvant chemotherapy, particularly when combined with immunotherapy, yields favorable efficacy (7–9). The potential benefits include less extensive surgery and improved survival outcomes for a subset of patients exhibiting a favorable response (10, 11). Major pathologic response (MPR) is a surrogate marker for satisfactory survival and may facilitate treatment de-escalation to improve quality of life (12–15).
With the increasing use of neoadjuvant immunochemotherapy, many patients with initial cT3–4 OC/OPC may achieve significant pathologic downstaging. Currently, no prospective data support the benefits of ART for these patients, leading to clinical uncertainty and variability in practice. This study retrospectively analyzes the benefits of ART for cT3–4 OC/OPC patients who achieved MPR following neoadjuvant immunochemotherapy and surgery. The purpose of this study is to evaluate whether ART to the head or neck can be safely omitted.
Patients and methods
Study population and eligibility criteria
We retrospectively collected clinicopathologic data from patients with cT3–4 OC/OPC treated with neoadjuvant immunochemotherapy followed by radical surgery at Sun Yat-sen University Cancer Center from July 2019 to May 2024. This study was approved by the hospital’s Institutional Review Board (approval number B2025-644-01), and the ethics committee review specifically waived the need for informed consent.
Inclusion criteria included: (1) patients with cT3-4a OC/OPC according to the eighth edition of American Joint Committee on Cancer (AJCC), (2) at least two cycles of neoadjuvant immunochemotherapy before surgery, (3) surgical resection with curative intent, and (4) MPR (≤ 10% residual viable tumor cells) of primary tumor.
Exclusion criteria included: (1) concurrent distant metastasis at diagnosis, (2) positive surgical margins, and (3) follow up period less than 12 months.
Data collection
Clinical and pathologic data were collected from the institutional HNSCC database. Pretreatment staging was assessed using high-resolution MRI, CT, and neck ultrasound. The chemotherapy regimen comprised albumin-bound paclitaxel (260 mg/m²) combined with either cisplatin (60 mg/m²) or lobaplatin (30 mg/m²), administered in three-week per cycle. Immunotherapy consisted of anti-PD-1 agents, including pembrolizumab (200 mg per cycle), nivolumab (3 mg/kg per cycle), tislelizumab (200 mg per cycle), camrelizumab (200 mg per cycle), sintilimab (200 mg per cycle), and toripalimab (240 mg per cycle).
Pathologic tumor staging and response evaluation were conducted by two certified pathologists. The response to neoadjuvant therapy was assessed using the resected tumor specimen, with residual viable tumor cells evaluated via H&E staining of all slides. The pathologists were blinded to patient groupings.
ART was delivered using intensity modulated radiotherapy techniques. Doses were 60–66 Gy in 28–33 fractions for the high-risk clinical target volume (CTV) and 54–56 Gy in 28–33 fractions for the low-risk CTV.
Statistical analysis
Nonparametric data were analyzed with the Wilcoxon rank-sum test, while categorical data were summarized by frequency and compared using the chi-square test for proportions. The outcomes of interest included local recurrence-free survival (LRFS), locoregional recurrence-free survival (LRRFS), distant metastasis-free survival (DMFS), and overall survival (OS). LRFS was defined as the duration from surgery to the occurrence of primary tumor recurrence. LRRFS was defined as the duration from surgery to the occurrence of primary tumor recurrence or LN metastasis. DMFS was defined as the duration from surgery to the occurrence of distant metastasis. OS was defined as the duration from surgery to death. Follow-up time was calculated from surgery to the last follow-up, hospitalization, or death.
Propensity score 1:1 matching was conducted using logistic regression with a caliper width of 0.02 to balance covariates related to treatment selection, including sex, age, tobacco use, alcohol use, primary tumor site, histologic grade, pathologic response, pathologic T stage (ypT, AJCC eighth), pathologic N stage (ypN, AJCC eighth), PNI, LVI, and lymph node yield (LNY). The Matching package in R (version 4.4.2) was used for matching. Clinical outcomes and the efficacy of ART were analyzed with Kaplan-Meier survival curves and the log-rank test, adjusted for propensity score matching (PSM).
Statistical analyses were conducted using SPSS software (version 27) and R software (version 4.4.2), with a p value of < 0.05 considered significant.
Results
Patient characteristics
A total of 247 patients were eligible (Figure 1). Their clinicopathologic characteristics are summarized in Table 1. The median age at diagnosis was 54 years (IQR, 46-64). Of the patients, 103 (41.7%) received ART while 144 (58.3%) did not (non-ART). Of note, 31 patients (12.6%) in the non-ART cohort received adjuvant anti-PD-1 maintenance therapy, with a median of 8 cycles (range: 5–35). Patients in the ART cohort tended to be younger (p = 0.008) and more likely to have LN metastasis (p < 0.001). No significant differences were found between cohorts in the distribution of sex, tobacco use, alcohol use, primary tumor site, histologic grade, number of neoadjuvant immunochemotherapy cycles, pathologic response, ypT stage, PNI, and LNY (p>0.05). After PSM, characteristics were balanced (p > 0.05), with 74 patients in each cohort.
Representative hematoxylin-and-eosin stained slide image of (A) complete pathologic response (no viable tumor), (B) major pathologic response (5% viable tumor), (C) unfavorable pathologic response (40% viable tumor), and (D) Flow Diagram.
Role of ART in the whole cohort and matched cohort
The median follow-up for the whole cohort was 31 months (IQR, 20-41). Fourty-three patients (17.4%) experienced failure events. Local recurrence occurred in 14 patients (5.7%), including 11 in the non-ART cohort and 3 in the ART cohort. Locoregional recurrence was noted in 36 patients (14.6%), including 25 in the non-ART cohort and 11 in the ART cohort. Thirteen patients (5.3%) developed distant metastasis, with 6 in the non-ART cohort and 7 in the ART cohort. The estimated 2-year LRFS, LRRFS, DMFS, and OS for the whole cohort were 93.4%, 85.0%, 95.6%, and 93.0%, respectively.
After adjusting for PSM, the median follow-up for the ART and non-ART cohorts were 30.5 months (IQR, 21-40) and 31.5 months (IQR, 16-42), respectively. In the non-ART cohort, 10 patients (13.5%) experienced local recurrence, 18 patients (24.3%) had locoregional recurrence, and 4 patients (5.4%) developed distant metastasis. In contrast, the ART cohort had 0 patients with local recurrence, 6 patients (8.1%) with locoregional recurrence, and 3 patients (4.1%) with distant metastasis. ART was associated with statistically significant improvements in LRFS by 14.5%, LRRFS by 14.0%, but not in DMFS and OS. The survival outcomes in the ART and non-ART cohorts were 100% versus 85.5% for LRFS (p = 0.001; Figure 2A), 91.5% versus 77.5% for LRRFS (p = 0.014; Figure 2B), 96.4% versus 95.6% for DMFS (p = 0.740; Figure 2C), and 96.5% versus 90% (p = 0.093; Figure 2D), respectively.
Kaplan-Meier curves of (A) local recurrence-free survival (LRFS), (B) locoregional recurrence-free survival (LRRFS), (C) distant metastasis-free survival (DMFS), and (D) overall survival (OS) in the propensity score–matched cohort.
Given that pT3–4 disease constitutes a high-risk factor for radiotherapy, we subsequently performed an analysis excluding patients with ypT3–4 disease from the entire cohort. After PSM, each cohort comprised 72 patients. The baseline characteristics are presented in Supplementary Table S1. ART continued to demonstrate significant improvements in LRFS (97.7% vs. 86.3%, p = 0.011; Figure 3A), LRRFS (90.5% vs. 76.9%, p = 0.014; Figure 3B), but not in DMFS (96.3% vs. 95.5%, p = 0.746; Figure 3C), and in OS (96.3% vs. 92.8%, p = 0.169; Figure 3D). The detailed survival outcomes are presented in Table 2.
Kaplan-Meier curves of (A) local recurrence-free survival (LRFS), (B) locoregional recurrence-free survival (LRRFS), (C) distant metastasis-free survival (DMFS), and (D) overall survival (OS) in patients with ypT0–2 tumor after propensity score–matching.
Adverse events
Of the 103 patients who received ART, 25 (24.3%) experienced late adverse effects of grade 3 or higher, including one death due to lung complications (Table 3). Four had grade 4 effects (skin, mucosa, bone, hematologic), while 20 patients (19.4%) had grade 3 effects, primarily in mucosa (7 cases), pharynx/esophagus (4 cases), skin (3 cases), subcutaneous tissue (2 cases), salivary gland (2 cases), bone (1 case), and other neurologic (1 case).
Discussion
It is uncertain if patients with cT3–4 OC/OPC at initial diagnosis can safely omit ART after achieving MPR following neoadjuvant immunochemotherapy. Our study findings demonstrate that omission of ART significantly compromises survival outcomes, leading to reduced LRFS and LRRFS, while DMFS, and OS are not significantly affected. These reductions remain statistically significant among patients with ypT0–2 tumors.
Neoadjuvant therapy is an essential approach in the treatment of many solid tumors. However, two phase 3 trials failed to show a survival benefit of neoadjuvant chemotherapy with TPF regime in HNSCC (16, 17). The addition of immune checkpoint inhibitors to neoadjuvant chemotherapy has shown significant pathologic responses, but survival outcomes are rarely reported. The recent KEYNOTE-689 trial demonstrated that perioperative administration of PD-1 inhibitors significantly improves event-free survival (EFS) in patients with locally advanced HNSCC, increasing the 3-year EFS rate from 46.4% to 57.6% (18). The most notable benefit was observed in reducing distant disease progression, while no significant effect was seen on local disease control. However, the study was unable to distinguish the specific benefits attributable to adjuvant therapy. Additionally, the low pathologic response rate to anti-PD-1 monotherapy limited the potential for further subgroup analyses, particularly concerning MPR. In our cohort of OC/OPC patients who achieved MPR to neoadjuvant therapy, outcomes were satisfying, with a 2-year LRFS of 91.8%, 2-year LRRFS of 83.3%, 2-year DMFS of 96.7%, and 2-year OS of 92.7%. These results are comparable to a study of 26 patients with HNSCC who received ART after neoadjuvant immunochemotherapy and surgery, which reported a 2-year PFS of 85.1% and OS of 89% (19). Our findings indicate that patients exhibiting MPR may have survival benefits, consistent with a prior research (13). Further study is needed to confirm long-term benefits.
The satisfying efficacy of neoadjuvant immunochemotherapy suggests the potienal of treatment de-escalation in the adjuvant setting. One possible approach may be that omit ART for favorable responders. In a pilot study of 23 patients with resectable HNSCC, 11 patients did not receive ART after neoadjuvant therapy. All patients remain disease-free at a median follow-up of 7.3 months, but long-term outcomes are not yet available (20). A study also found that omitting ART after neoadjuvant chemotherapy and surgery for oropharyngeal squamous cell carcinoma led to excellent locoregional control (21). Ju et al. reported no significant differences in OS or LRRFS between patients with and without ART (22). However, a substantial discrepancy was observed in 10-year OS between the ART and non-ART cohorts (58.9% versus 44.1%). In contrast, the findings of our study diverge from these results. Specifically, omission of ART was associated with a significant compromise in local and locoregional control. Notably, our data suggest that ART should not be avoided in OC/OPC patients after achieving MPR following neoadjuvant therapy, despite their generally favorable outcomes. This disadvantage may be related to the extent of surgery performed following significant tumor downstaging. Currently, there is no consensus on the appropriate extent of resection following neoadjuvant therapy. In this study, patients underwent extended surgery with resection margins exceeding 1 cm, determined by their response to neoadjuvant immunochemotherapy. Consequently, a considerable proportion of patients might have undergone less extensive surgery if the procedure had been based solely on the initial clinical stage. Although previous studies have reported satisfactory survival outcomes following de-escalated surgery after neoadjuvant therapy (23, 24), our study suggests caution.It indicates that reducing the extent of surgery after significant pathologic downstaging may compromise radical oncologic control and may necessitate ART. Therefore, the optimal extent of surgical resection requires further investigation.
Reducing the extent of ART for favorable responders may constitute a viable strategy. In a phase II trial (NCT05476965), patients who achieved a MPR to neoadjuvant immunochemotherapy and surgery received a de-escalated dose of radiotherapy (less than 54 Gy/25 fractions). Ten patients received low-dose ART, and 12 received full-dose. At a median follow-up of 23 months, there were no relapses in the low-dose group (25). The OPTIMAL trial showed that induction chemotherapy with dose and volume de-escalated definitive radiotherapy for HPV-positive oropharyngeal squamous cell carcinoma leads to favorable oncologic outcomes and reduced toxicity (26). And The OPTIMAL II trial found that single-modality radiotherapy or transoral robotic surgery after a favorable response to neoadjuvant immunochemotherapy resulted in excellent survival and functional outcomes (27). Similarly, the DEPEND trial indicated that de-escalated definitive radiotherapy after favorable responses to neoadjuvant immunochemotherapy in HPV-negative HNSCC improved survival with fewer acute toxic effects (28). The efficacy of reducing the radiotherapy dose or volume in ART for favorable pathologic responders may represent a promising de-escalation treatment.
Outcomes among patients with OC/OPC with favorable pathologic response to neoadjuvant therapy may probably continue to improve due to advancements in systemic therapy, particularly the use of immune checkpoint inhibitors. These developments may allow more patients to transition from advanced to early-stage tumors, making the findings from the present study applicable to more patients in the future.
Our study has several limitations. First, we only reported early oncological outcomes, requiring further long-term follow-up. Second, we did not analyze the impact of concomitant regimens during ART. Finally, as a retrospective study, it may have potential biases.
Conclusions
Patients with cT3–4 OC/OPC who achieved favorable pathologic response after neoadjuvant immunochemotherapy and surgery benefit from ART. Further research is needed to optimize adaptive de-escalation strategies for this population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chow LQM . Head and neck cancer. New Engl J Med. (2020) 382:60–72. doi: 10.1056/NEJ Mra 1715715, PMID: 31893516 · doi ↗ · pubmed ↗
- 2National Comprehensive Cancer Network . Head and Neck Cancers (Version 3.2024). (2024). Available online at: https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf.
- 3Awan M Akakpo KE Shukla M Graboyes EM Pipkorn P Puram SV . The substantial omission of indicated postoperative radiotherapy in patients with advanced-stage oral cancer in the US-A call to action. JAMA Otolaryngology-Head Neck Surg. (2021) 147:907–9. doi: 10.1001/jamaoto.2021.1744, PMID: 34383035 PMC 8517743 · doi ↗ · pubmed ↗
- 4Bernier J Domenge C Ozsahin M Matuszewska K Lefèbvre JL Greiner RH . Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. New Engl J Med. (2004) 350:1945–52. doi: 10.1056/NEJ Moa 032641, PMID: 15128894 · doi ↗ · pubmed ↗
- 5Cooper JS Pajak TF Forastiere AA Jacobs J Campbell BH Saxman SB . Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. New Engl J Med. (2004) 350:1937–44. doi: 10.1056/NEJ Moa 032646, PMID: 15128893 · doi ↗ · pubmed ↗
- 6Bernier J Cooper JS Pajak TF van Glabbeke M Bourhis J Forastiere A . Defining risk levels in locally advanced head and neck cancers:: A comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (22931) and RTOG (9501). Head Neck-Journal Sci Specialties Head Neck. (2005) 27:843–50. doi: 10.1002/hed.20279, PMID: 16161069 · doi ↗ · pubmed ↗
- 7Masarwy R Kampel L Horowitz G Gutfeld O Muhanna N . Neoadjuvant PD-1/PD-L 1 inhibitors for resectable head and neck cancer A systematic review and meta-analysis. JAMA Otolaryngology-Head Neck Surg. (2021) 147:871–8. doi: 10.1001/jamaoto.2021.2191, PMID: 34473219 PMC 8414366 · doi ↗ · pubmed ↗
- 8Wise-Draper TM Gulati S Palackdharry S Hinrichs BH Worden FP Old MO . Phase II clinical trial of neoadjuvant and adjuvant pembrolizumab in resectable local-regionally for advanced head and neck squamous cell carcinoma. Clin Cancer Res. (2022) 28:1345–52. doi: 10.1158/1078-0432.CCR-21-3351, PMID: 35338369 PMC 8976828 · doi ↗ · pubmed ↗