Vanishing Bile Duct Syndrome as a Rare Complication of Classic Hodgkin's Lymphoma: A Case Report and Literature Review
Jody W Tai, Vivek D Shah, Rhett L Harmon, Shaun Chandna, Jessica Yan, Payman Fathizadeh, Simon Beaven, Deepthi Karunasiri, Phyllis Kim

TL;DR
A rare case of Vanishing Bile Duct Syndrome occurring alongside Hodgkin's Lymphoma is reported, highlighting the need for early treatment and collaboration between specialists.
Contribution
This case report adds to the limited literature on VBDS as a complication of classic Hodgkin's lymphoma.
Findings
A patient with classic Hodgkin's lymphoma developed Vanishing Bile Duct Syndrome.
Liver biopsy showed bile duct paucity without lymphoma involvement.
Partial liver recovery was observed with cHL-directed treatment.
Abstract
Vanishing bile duct syndrome (VBDS) is an acquired condition of progressive intrahepatic bile duct loss, resulting in severe cholestasis. Here, we present a case of VBDS in a patient with newly diagnosed classic Hodgkin's lymphoma (cHL). Our patient presented with cholestatic liver test elevations, including bilirubin and alkaline phosphatase. Liver biopsy confirmed the paucity of bile ducts and did not show involvement by lymphoma. Though the exact pathophysiology is unclear, it is postulated to be driven by cytokine release and T-lymphocyte cell dysregulation. Our patient has made a remarkable, albeit incomplete, liver recovery with cHL-directed treatment. Given the poor prognosis and higher mortality rate of VBDS, a multidisciplinary approach involving oncology, hepatology, and prompt initiation of dose-adjusted chemotherapy is imperative.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
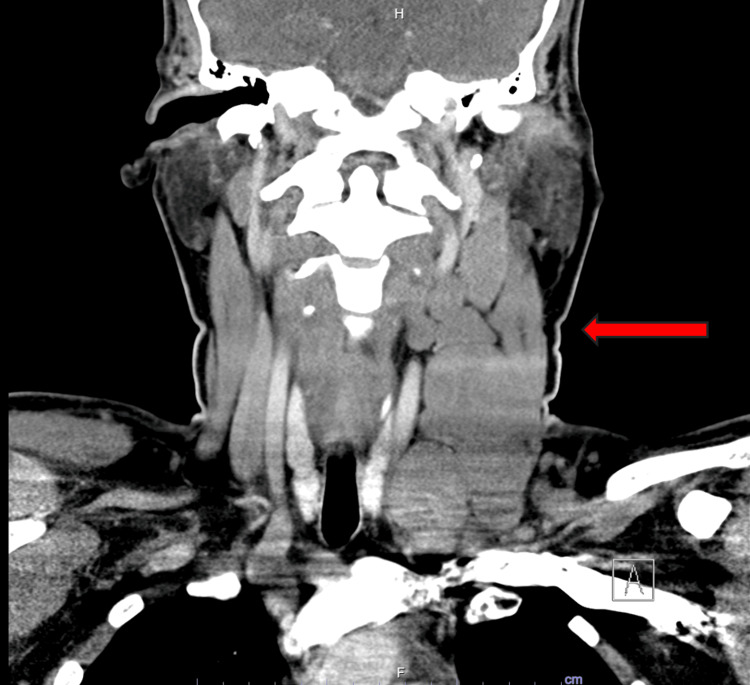 Figure 1
Figure 1 Figure 2
Figure 2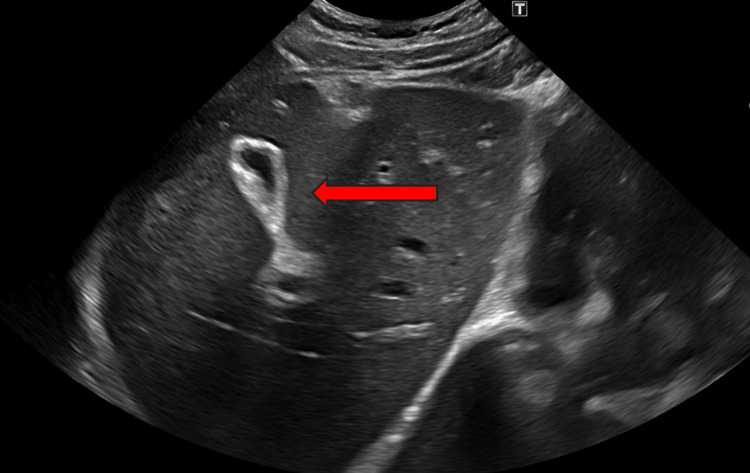 Figure 3
Figure 3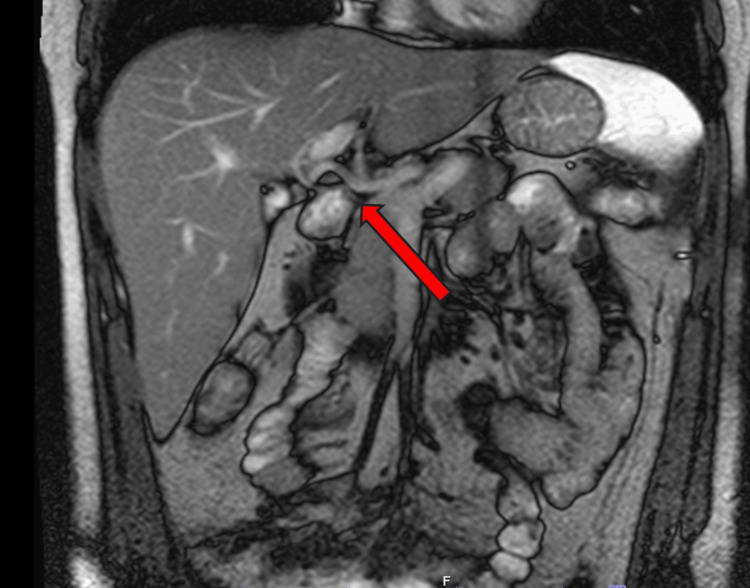 Figure 4
Figure 4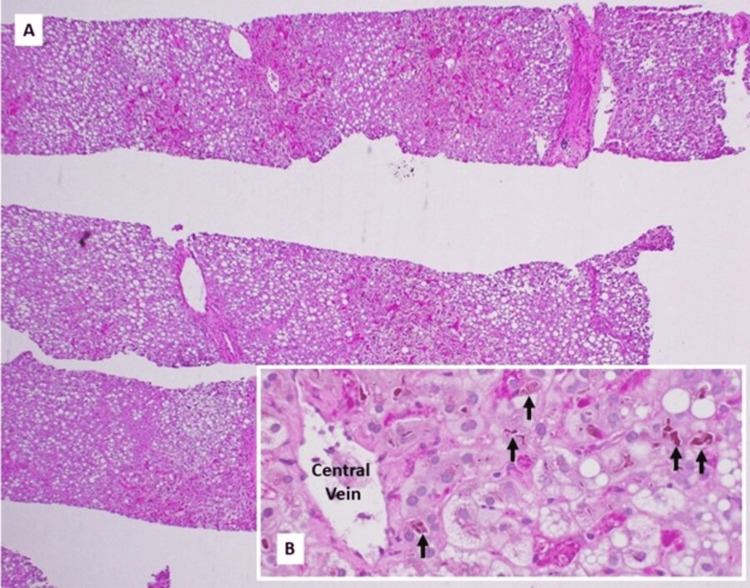 Figure 5
Figure 5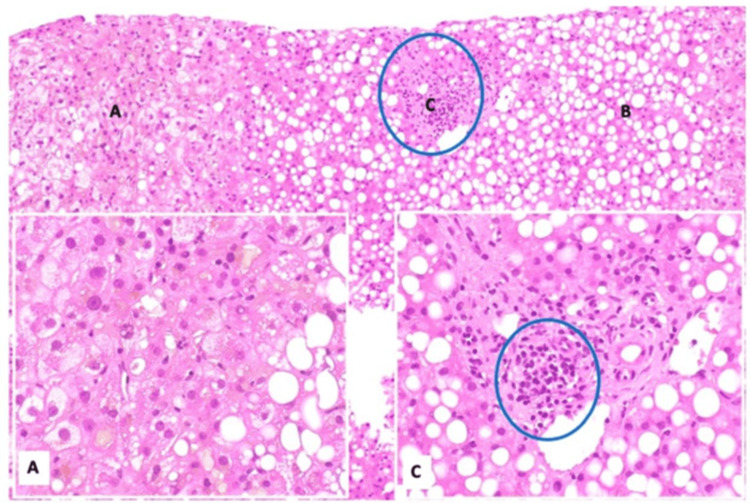 Figure 6
Figure 6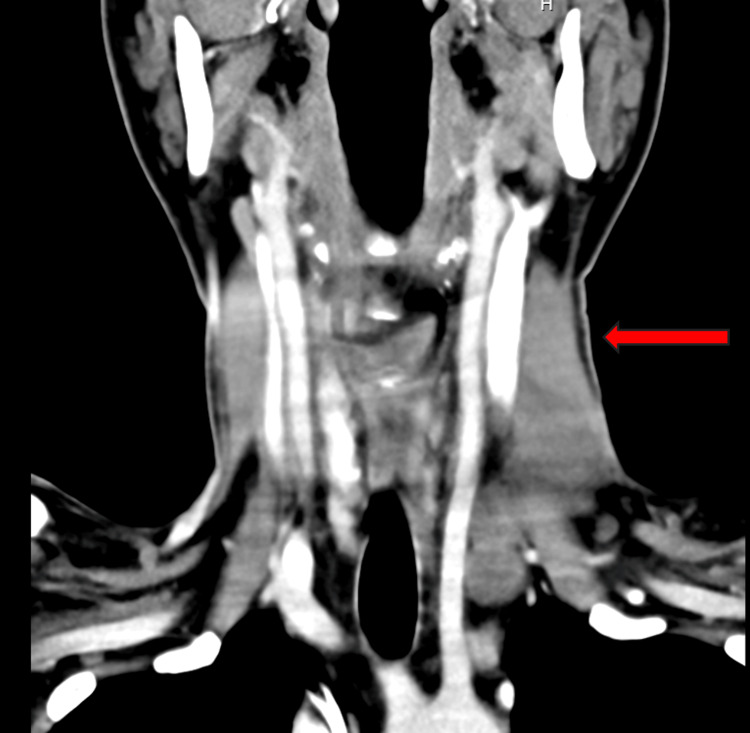 Figure 7
Figure 7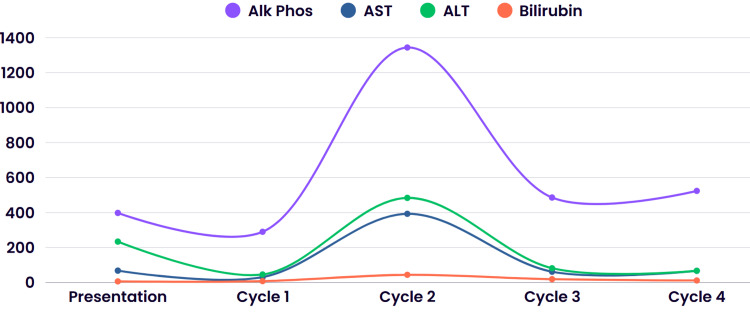 Figure 8
Figure 8| Test | Result | Reference Range |
| WBC | 4.3 K/cumm | 4.5-10.0 K/cumm |
| Hgb | 12.8 g/dL | 12.0-14.6 g/dL |
| Platelets | 64 K/cumm | 160-360 K/cumm |
| Alkaline phosphatase | 398 U/L | 38-126 U/L |
| AST | 68 U/L | 15-41 U/L |
| ALT | 234 U/L | 14-54 U/L |
| Total bilirubin | 6.4 mg/dL | 0.1-1.2 mg/dL |
| Direct bilirubin | 4.2 mg/dL | 0.1-0.4 mg/dL |
| GGT | 90 U/L | 7-50 U/L |
| HIV | Negative | Negative |
| Hepatitis B | Negative | Negative |
| Hepatitis C | Negative | Negative |
| Anti-mitochondrial antibody | Negative | Negative |
| Anti-smooth muscle antibody | Negative | Negative |
| Author | Year | Liver biopsy | HL treatment (chemotherapy and/or radiation) | Outcome/cause of death |
| Hasan F [ | 2024 | VBDS | Yes | Unknown |
| Patodiya B [ | 2023 | Lobular inflammation | Yes | Remission |
| Nano O [ | 2023 | VBDS | Yes | Remission |
| Shokri F [ | 2023 | VBDS | Yes | Death/hepatic and renal failure |
| Keramidas V [ | 2021 | VBDS | Yes | Remission |
| Papakonstantinou I [ | 2021 | IC | Yes | Remission |
| Ousley RJ [ | 2021 | VBDS | Yes | Remission |
| Greca RD [ | 2020 | VBDS | Yes | Unknown |
| Bakhit M [ | 2017 | VBDS | Yes | Unknown |
| Rota Scalabrini D [ | 2014 | VBDS | Yes | Remission |
| Nader K [ | 2013 | VBDS | Yes | Death/hepatic failure and sepsis |
| Aleem A [ | 2013 | VBDS | Yes | Death/hepatic failure |
| Wong KM [ | 2013 | VBDS | Yes | Remission |
| Umit H [ | 2009 | VBDS | Unknown | Unknown |
| Pass AK [ | 2008 | VBDS | Yes | Remission/awaiting liver transplant |
| Pass AK [ | 2008 | VBDS | Yes | Death/aspiration |
| Leeuwenburgh I [ | 2008 | VBDS | Yes | Remission |
| DeBenedet AT [ | 2008 | VBDS | Yes | Death/unknown |
| Ballonoff A [ | 2007 | VBDS | Yes | Remission |
| Barta SK [ | 2006 | IC | Yes | Remission |
| Schmitt A [ | 2006 | VBDS | No | Death/sepsis |
| Han WS [ | 2005 | VBDS | Unknown | Recurrent HL |
| Cordoba Iturriagagaitia A [ | 2005 | VBDS | Unknown | Remission |
| Guliter S [ | 2004 | VBDS | Yes | Death/sepsis |
| Liangpunsakul S [ | 2002 | Cholestatic hepatitis | Yes | Remission |
| Komurcu S [ | 2002 | VBDS | Yes | Death/hepatic failure |
| Ripoll C [ | 2002 | VBDS | Yes | Death/hepatic failure |
| Ripoll C [ | 2002 | VBDS | Yes | Remission |
| Ozkan A [ | 2001 | VBDS | Yes | Death/hepatic failure |
| Allory Y [ | 2000 | VBDS | Unknown | Unknown |
| Rossini MS [ | 2000 | VBDS | Yes | Death/hepatic failure |
| Yusuf MA [ | 2000 | VBDS | Yes | Death/hepatic failure |
| Dourakis SP [ | 1999 | Hepatocellular necrosis | Yes | Death/hepatic failure |
| Yalcin S [ | 1999 | IC | No | Death/sepsis |
| Yalcin S [ | 1999 | IC | Yes | Remission |
| De Medeiros BC [ | 1998 | VBDS | Yes | Death/hepatic failure |
| De Medeiros BC [ | 1998 | VBDS | Yes | Remission |
| Crosbie OM [ | 1997 | VBDS | Yes | Remission |
| Gottrand F [ | 1997 | VBDS | No | Death/hepatic failure |
| Warner AS [ | 1994 | IC | Yes | Remission |
| Jansen PLM [ | 1994 | IC | Yes | Death/variceal hemorrhage |
| Hubscher SG [ | 1993 | VBDS | Yes | Death/pneumonia |
| Hubscher SG [ | 1993 | VBDS | Yes | Death/unknown |
| Hubscher SG [ | 1993 | VBDS | Yes | Death/sepsis |
| Birrer MJ [ | 1987 | IC | Yes | Death/sepsis |
| Lieberman DA [ | 1986 | IC | No | Death/respiratory arrest |
| Trewby PN [ | 1979 | IC | Yes | Remission |
| Trewby PN [ | 1979 | Mild portal hepatitis | No | Death |
| Trewby PN [ | 1979 | Lymphoma infiltration | Yes | Death |
| Trewby PN [ | 1979 | Lymphoma infiltration | No | Death |
| Trewby PN [ | 1979 | Mixed inflammatory and atypical histiocytes | Yes | Remission |
| Trewby PN [ | 1979 | IC | Yes | Death/hepatic failure |
| Piken EP [ | 1979 | IC | Yes | Death/unknown |
| Perera DR [ | 1974 | IC | Yes | Death/hepatic failure |
| Perera DR [ | 1974 | IC | Yes | Remission |
| Perera DR [ | 1974 | IC | Yes | Remission |
| Groth C [ | 1972 | IC | Yes | Death/hepatic failure |
| Juniper K [ | 1963 | IC | Yes | Death/hepatic failure |
| Bouroncle B [ | 1962 | IC | Yes | Death/hepatic failure |
| Bouroncle B [ | 1962 | IC | Yes | Death/hepatic failure |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Diseases and Immunity · Hepatocellular Carcinoma Treatment and Prognosis · Bartonella species infections research
Introduction
Vanishing bile duct syndrome (VBDS) is a syndrome of progressive destruction and loss of intrahepatic bile ducts leading to cholestasis. Presentations can range from asymptomatic to fulminant liver failure. Most commonly, VBDS arises within one to six months after a drug-induced liver injury, most commonly with antibiotics such as amoxicillin/clavulanic acid, fluoroquinolones, or trimethoprim-sulfamethoxazole, among others [1]. In order to diagnose VBDS, alternate etiologies of biliary duct loss, such as primary biliary cholangitis, primary sclerosing cholangitis, and graft-versus-host disease, must be ruled out. The diagnosis is confirmed with a liver biopsy, which shows intralobular bile ductopenia with less than 50% of portal areas having a bile duct in an adequate biopsy specimen of at least 10 portal tracts [1]. A paucity of reports has described VBDS associated with classic Hodgkin's lymphoma (cHL), with no consensus in the literature review on its incidence. The pathobiology is poorly understood but likely to be driven by hepatotoxic cytokines and thymocyte-lymphocyte (T-lymphocyte) dysregulation, leading to immunogenic damage to biliary ducts. Due to impaired liver function due to VBDS, treatment of the underlying disease is often challenging. Dose modifications can lead to undertreatment of the cHL, which is a highly treatable and curable disease. Standard of care with chemotherapy and radiation has resulted in high cure rates, with a greater than 80% five-year overall survival [2]. In our patient, treatment adaptations have led to remarkable improvements in liver function in parallel with the response of the lymphoma. We add to the existing literature a case of cHL as the leading explanation for VBDS with ensuing cholestatic liver injury and provide a structured literature review to inform diagnostic and therapeutic decisions.
Case presentation
A 31-year-old male with no prior medical history presented to the emergency department for diffuse abdominal pain and diarrhea for one week. He reported one week of subjective fevers and three to four watery bowel movements daily. He also endorsed 20-pound weight loss and occasional night sweats over the prior six months and left-sided neck swelling over the prior four months. He denied any emesis, early satiety, dysphagia, odynophagia, melena, hematochezia, or dark-colored urine. There was no reported family history of liver disease. Social history was notable for working in construction and no tobacco, alcohol, or drug use.
Upon presentation, the patient’s temperature was 36.7 degrees Celsius, heart rate of 80 beats per minute, blood pressure of 112/66 millimeters of mercury (mmHg), and oxygen saturation of 99% on room air. Physical exam was significant for left-sided neck fullness without any palpable lymphadenopathy elsewhere. The patient was not noted to be jaundiced.
He was found to have leukopenia, thrombocytopenia, elevated liver tests, and coagulopathy. Laboratory investigations are summarized in Table 1. Other relevant studies included a stool polymerase chain reaction (PCR) panel for infectious causes of diarrhea, a stool ova and parasite exam, and a stool acid-fast bacillus (AFB) exam. Liver injury workup included negative anti-nuclear antibody, anti-smooth muscle antibody, hepatitis panel, alpha-1 antitrypsin, and normal iron stores. At presentation, the R factor was 1.8, suggestive of a cholestatic pattern of injury.
Computerized tomography (CT) of the neck was significant for enlarged, bulky cervical lymph nodes throughout the left, largest in the left neck measuring 5.2 x 2.7 x 4.1 centimeters (cm), as shown in Figure 1.
Coronal view of CT neckThe red arrow highlights the left cervical lymphadenopathy.
CT scan of the chest, abdomen, and pelvis revealed inflammatory changes in a section of the jejunum, as well as in the terminal ileum and colon, as seen in Figure 2.
CT scan of the chest, abdomen, and pelvis with inflammatory changes in a section of the jejunum, as well as in the terminal ileum and colonThe red arrow points towards an area of mucosal enhancement with increased wall thickness.
The right upper quadrant ultrasound was consistent with hepatomegaly and a contracted gallbladder, as seen in Figure 3.
Ultrasound of the liver from the long axis showing hepatomegalyThe red arrow points towards contracted gallbladder.
Magnetic resonance cholangiopancreatography (MRCP) demonstrated normal bile ducts and a patent biliary tree without evidence of strictures, masses, or biliary filling defects; there was no evidence of primary sclerosing cholangitis, as seen in Figure 4.
MRCP showing normal bile ducts and a red arrow pointing towards a patent biliary tree without evidence of strictures, masses, or biliary filling defectsMRCP: magnetic resonance cholangiopancreatography
Gastroenterology was consulted and performed an endoscopy with colonoscopy that revealed patchy colonic inflammation with ulcerations and erythema in the ascending and transverse colon, with biopsies showing active inflammation without granulomas or lymphomatous involvement. Enteroscopy demonstrated mild gastropathy and diffuse erythema, edema, and ulcerations throughout the duodenum and jejunum, which were biopsied to evaluate for *Helicobacter pylori *and rule out Crohn’s disease. Biopsies and staining were negative for cytomegalovirus (CMV) but positive for H. pylori, for which the patient was initiated on quadruple therapy involving tetracycline, metronidazole, bismuth salicylate, and pantoprazole. A biopsy of the left-sided neck mass revealed lymphoid tissue with Reed-Sternberg cells and positive CD15 and CD30 markers, confirming classic Hodgkin’s lymphoma of the nodular sclerosis type. A bone marrow biopsy was negative for malignant involvement.
The patient continued to decline with worsening cholestatic liver injury and physical signs of hepatic dysfunction, including jaundiced skin and sclera, despite empiric treatment with ursodiol. No other causes of liver injury, such as viral hepatitis, autoimmune hepatitis, primary biliary cholangitis, primary sclerosing cholangitis, or inherited conditions, were found on workup, including serologies and imaging. A liver biopsy was pursued, which showed bile duct injury accompanied by ductopenia affecting more than 50% of the portal tracts and severe macrovesicular steatosis without fibrosis, as seen in Figures 5-6. No histologic evidence of direct lymphomatous invasion was found.
Liver core biopsies demonstrating macrovesicular steatosis (A, periodic acid-Schiff stain with diastase, 40×) and marked canalicular-predominant cholestasis (B, arrow; periodic acid-Schiff stain with diastase, 400×)Credit: Payman Fathizadeh, MD
Liver core biopsies demonstrate canalicular cholestasis (A, hematoxylin and eosin stain, 400x), approximately 70% macrovesicular steatosis (B, hematoxylin and eosin stain, 100x), and significant bile duct loss (C, hematoxylin and eosin stain, 400x)The few remaining bile ducts exhibit evidence of injury and degenerative changes. These histologic findings are consistent with ductopenia/vanishing bile duct syndrome, which may be associated with drug-induced liver injury or the patient's documented history of Hodgkin lymphoma. The concurrent macrovesicular steatosis may also represent a manifestation of drug-related hepatotoxicity. No evidence of lymphomatous infiltration is identified. The histologic features do not suggest extrahepatic biliary obstruction.Credit: Payman Fathizadeh, MD
The patient denied any use of herbal remedies, over-the-counter drugs, or other culprit medication use that implicated concern for drug-induced liver injury. Given the absence of other identifiable etiologies, the findings of cholestatic liver injury and severe ductopenia on liver biopsy were thought to most likely represent VBDS as a paraneoplastic phenomenon in the setting of newly diagnosed Hodgkin's lymphoma (HL). At this juncture, given extremely poor liver function and dependence on hepatic metabolism for the use of most active agents in the treatment of cHL, we had an extensive discussion with the patient and his family. We shared that not treating the disease would likely result in fulminant liver failure. However, treatment of the disease with optimal therapy would likely result in severe treatment-related toxicities, amplifying known cytopenias, emetogenesis, cardiotoxicities, and more. The option of hospice was introduced to the patient, given worsening liver function tests, and he opted to continue with full care, given that he is the sole provider for his two children.
The patient was initiated on chemotherapy with cyclophosphamide, brentuximab vedotin, and dexamethasone. He received one cycle of inpatient and was discharged with ursodiol. Liver function improved with one dose of therapy, and treatment was accordingly continued with additional cHL-specific treatments, including brentuximab vedotin, vinblastine, and dacarbazine. These drugs were chosen due to their known efficacy and ability to modify the doses in the setting of impaired liver function. Doxorubicin and bleomycin were omitted due to the risk of severe toxicities, which could further augment mortality risk. At the time of writing this article, our patient has completed four cycles of chemotherapy with a peak in liver function tests around cycle 2 and subsequent downtrending with additional cycles of chemotherapy. Interval imaging with CT of his neck showed a marked decrease in the size of his left neck lymphadenopathy, as seen in Figure 7.
Interval imaging of the CT neck showing marked decrease in the size and number of left jugulodigastric chain adenopathy as labeled by the red arrow, largest measuring 13 mm x 24 mm x 38 mm
Figure 8 demonstrates the overall trend for the patient’s liver tests throughout his presentation.
Trend of alkaline phosphatase, AST, ALT, and bilirubin throughout the patient’s presentationCycle indicates when the patient received chemotherapy. Cycle 1: brentuximab, cyclophosphamide, dexamethasone; Cycle 2: cyclophosphamide, dexamethasone; Cycle 3 and Cycle 4: brentuximab, vinblastine, dacarbazineALT: alanine transaminase; AST: aspartate aminotransferase
The patient was not considered an orthotopic liver transplant candidate, given his active lymphoma and lack of adequate family or social support for post-transplant care. Transplant assessment remains on hold pending completion of Hodgkin's lymphoma treatment, and issues related to care planning, such as securing appropriate caregiver support, are resolved.
Discussion
The association between VBDS and HL was first described in 1993 by Hubscher et al. [3] and, since then, has been described in a number of published cases. We compiled a list of all published case reports through a search of the PubMed database, Science Direct, and Google Scholar, including both English and non-English cases, which is summarized in Table 2.
Among the 60 case reports listed above, remission was achieved in 36.67% of cases (n=22), not including those patients whose outcomes were unknown. Although liver function test abnormalities and hepatic involvement with HL can be seen in up to 50% of patients due to hemolysis, biliary obstruction from lymph node enlargement, and viral illness such as CMV, VBDS specifically is a rare manifestation of HL patients and overall can be a marker of poor prognosis [12]. Differentiating VBDS from HL involvement of the liver relies on liver biopsy showing histologic evidence of more than 50% interlobular bile duct loss in a specimen that includes at least 10 portal tracts [1]. In severe instances, a biopsy may show a total lack of bile ducts with complete ductopenia, having "burnt-out" portal tracts that are devoid of bile ducts [1]. Diagnosing VBDS can therefore be difficult due to its nonspecific symptoms and the necessity of a liver biopsy to confirm the absence of bile ducts.
The pathophysiology is complex and postulated to be multifactorial, involving autoimmune, inflammatory, and regenerative factors all playing a role in the destruction of bile ducts, though the precise mechanism is unclear [1]. The onset of VBDS is believed to be linked to the heightened apoptosis of biliary epithelial cells, which occurs in response to triggers such as death receptor activation, autoimmune disease, ischemia, oxidative stress, toxins, and viral pathogens. Some theories include cell-mediated immunologic reactions leading to ductopenia, auto-apoptosis of biliary epithelium, or cytokines released by lymphoma cells [1].
VBDS can occur as both an irreversible and a transient condition. While some cases progress to fibrosis, cirrhosis, and liver failure, others may improve over months to years. Liver transplantation is reserved for advanced or refractory cases when the condition leads to significant ductopenia, biliary cirrhosis, and liver failure. However, it is important to consider treatment of the underlying cause and the possibility of biliary regeneration [49-52]. Broadly speaking, VBDS of any origin can be considered for treatment with corticosteroids and ursodeoxycholic acid (UDCA) that may slow inflammation and stimulate bile secretion, preventing apoptosis of cholangiocytes. UDCA utilizes multiple strategies to defend cholangiocytes from the damaging impact of bile acids and to boost the function of impaired hepatobiliary secretion [53-55].
From an oncology perspective, treatment of HL-related VBDS is controversial due to the selection of agents, timing of initiation, and questions regarding liver transplantation referral and candidacy. It overall makes treating an otherwise curable malignancy quite challenging. This is because the standard-of-care treatment for HL is with the first-line regimen known as ABVD: doxorubicin, bleomycin, vinblastine, and dacarbazine. However, doxorubicin and vinblastine are both hepatically metabolized. Doxorubicin is contraindicated if bilirubin is higher than 5.0 mg/dL, and vinblastine is contraindicated if the AST/ALT are greater than three times the upper limit of normal. There is no consensus on first-line therapy in this setting. Whether the modified ABVD regimen should be given with dose adjustment, or if the second-line regimen GDP (gemcitabine 1,600 mg (1,000 mg/m^2^ IV infusion), dexamethasone 40 mg (once daily orally), and carboplatin 600 mg infusion (target AUC of 4-6 mg/mL/min)) should be used is unclear and provider-dependent [13]. Scalabrini et al. reported that only 12% of patients with VBDS who received an upfront reduced ABVD regimen had improved cholestasis and liver function impairment compared to 51% of patients receiving the full dose [13] and therefore advocate for normal dosing. However, it is important to note that these specific patients initially responded well clinically to high doses of UDCA and prednisone prior to receiving ABVD. Conventionally, most other clinicians will attempt modified or alternative regimens to treat the underlying HL until the hyperbilirubinemia normalizes enough to allow ABVD treatment, such as single-agent chemotherapy that is not hepatically metabolized or dose-reduction [6]. Literature review also shows favorable outcomes with the use of nivolumab (a programmed cell death protein or PD-1 receptor inhibitor that prevents T-cell silencing) and brentuximab (an antibody-drug conjugate that binds to cluster of differentiation or CD-30 antigen on cancer cells that disrupts microtubules and leads to cell apoptosis) [5,11,56]. For example, Gupta et al. reported a favorable outcome in patients first given single-agent brentuximab as bridging therapy [57]. Liver transplant was discussed in some of the reviewed case reports as last-line therapy for irreversible cirrhosis; however, active HL disease often precludes these patients from being on the transplant list.
Regarding our patient, he was started on chemotherapy with cyclophosphamide, dexamethasone, and brentuximab vedotin, a combination therapy modified to minimize hepatotoxicity [58] and the potential toxicities of impaired hepatic drug clearance. His labs showed stable liver tests after the first cycle of treatment. Though his liver tests continued to rise thereafter, at the time of writing this article, the patient has completed four cycles of treatment, and his liver tests are improving. He was evaluated by the liver transplant team at a nearby hospital, and a multidisciplinary decision was made to defer transplant until the cHL is completely treated. We posit that liver transplantation should be considered in cHL patients who achieve complete remission after systemic therapy, given the irreversible nature of bile duct loss.
Generally, active malignancy other than within the confines of specific exceptions for liver transplant (e.g., hepatocellular carcinoma, perihepatic cholangiocarcinoma, other emerging indications) precludes consideration for liver transplant for a two- to five-year period following treatment at many centers. Liver transplantation for VBDS in cHL is controversial and likely rare. To our knowledge, this may be one of the first cases in which an orthotopic liver transplant was being considered as treatment for VBDS in an active cHL patient. While these decisions are complex and need to be made in a multidisciplinary setting with the transplant team and oncology, taking into account potential benefits, risks of relapse/recurrence, and post-transplant immunosuppressive risks, we posit that liver transplantation may be a potential consideration in select cHL patients with VBDS that are not improving who achieve complete remission after systemic therapy given the irreversible nature of bile duct loss.
Although VBDS often portends a poor prognosis in HL patients due to the irreversible nature of bile duct loss leading to hepatic failure and death, recent case reports suggest a possibility of reversal or at least improved survival among patients who respond to cancer treatment. This ranges from complete remission with treatment of lymphoma with either total resolution in lab abnormalities or lingering mild isolated elevation in alkaline phosphatase levels without clinical symptoms [12].
Conclusions
VBDS is a rare paraneoplastic phenomenon of cHL whose pathophysiology is incompletely understood but thought to be related to lymphoma cytokine release or cell-mediated immunologic reactions causing ductopenia. Rarely, it can be reversible with treatment of cHL, but otherwise can progress to acute liver failure with high mortality rates. It is important to recognize VBDS related to cHL early to initiate treatment with careful consideration of the limiting factors and the potential need for early liver transplant evaluation, if clinically indicated. It is important to acknowledge that, while liver transplantation may be a potential consideration if the liver injury fails to improve in those achieving complete remission, the role of liver transplant in this setting remains limited, is controversial, and needs to be determined in a multidisciplinary transplant setting. Further steps include standardizing the treatment of cHL-related VBDS to optimize survival outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vanishing bile duct syndrome Liver Tox: Clinical and Research Information on Drug-Induced Liver Injury National Institute of Diabetes and Digestive and Kidney Diseases Bethesda, MD National Institute of Diabetes and Digestive and Kidney Diseases 2019 https://www.ncbi.nlm.nih.gov/books/NBK 548715/31643176 · pubmed ↗
- 2International prognostic score in advanced-stage Hodgkin’s lymphoma: altered utility in the modern era J Clin Oncol Moccia AA Donaldson J Chhanabhai M 338333883020122286988710.1200/JCO.2011.41.0910 · doi ↗ · pubmed ↗
- 3Vanishing bile duct syndrome: a possible mechanism for intrahepatic cholestasis in Hodgkin's lymphoma Hepatology Hubscher SG Lumley MA Elias E 7077171993 https://pubmed.ncbi.nlm.nih.gov/7678577/7678577 · pubmed ↗
- 4Vanishing bile duct syndrome in advanced Hodgkin’s lymphoma: a case report of diagnostic and therapeutic challenges Am J Gastroenterol Hasan F Garcia A Singh A Timsaal Y Alabd A Shah A 0201192024
- 5A rare presentation of vanishing bile duct syndrome in Hodgkin lymphoma: case report SAGE Open Med Case Rep Patodiya B Ramani VK Rao PN Sharma M Patodiya S Reddy DN 205031311202310.1177/2050313 X 231208968 PMC 1063715537954540 · doi ↗ · pubmed ↗
- 6Vanishing bile duct syndrome in a patient with recurrent Hodgkin lymphoma J Med Cases Nano O Ivanov S Kapoor T 1621681420233730396910.14740/jmc 4073 PMC 10251707 · doi ↗ · pubmed ↗
- 7Fatal vanishing bile duct syndrome in Iranian patient with Hodgkin's lymphoma Clin Case Rep Shokri F Shariati A Veisari AK 011202310.1002/ccr 3.7671 PMC 1035700237484745 · doi ↗ · pubmed ↗
- 8Vanishing bile duct syndrome and Hodgkin’s lymphoma: case report and thorough review of the literature Ann Hematol Oncol Keramidas V Tastanis C Tsirogianni K Hytiroglou P Papaioannou M 136582021 https://austinpublishinggroup.com/hematology/fulltext/hematology-v 8-id 1365.pdf