Recurrent Hematuria Unmasking a Rare Case of Bladder Schistosomiasis in a Child Living in a Non-endemic Country: A Case Report
Hany M Elkordy, Mohamed Elkordi, Greta Peciulyte, Saad Mina

TL;DR
A child in the UAE with recurring blood in urine was diagnosed with a rare bladder parasite infection typically found in other regions.
Contribution
This case report highlights schistosomiasis as a rare but possible cause of hematuria in non-endemic regions.
Findings
An 11-year-old girl in UAE presented with painless hematuria and was diagnosed with bladder schistosomiasis.
Treatment with praziquantel led to full clinical and radiological recovery.
The case emphasizes the need to consider parasitic infections in hematuria differential diagnosis in non-endemic areas.
Abstract
Bladder schistosomiasis is a parasitic infection rarely encountered in non-endemic regions. We report the case of an 11-year-old girl living in the United Arab Emirates (UAE) who presented with recurrent, painless gross hematuria. Urine cytology revealed Schistosoma haematobium eggs, and imaging demonstrated bladder wall calcifications. Cystoscopy showed extensive sandy patches, and histopathology confirmed the diagnosis. The patient was treated with praziquantel and achieved complete clinical and radiological resolution. This case highlights the importance of considering schistosomiasis in the differential diagnosis of unexplained hematuria, even in non-endemic regions, particularly in patients with relevant travel history. It underscores the need for heightened awareness of parasitic causes of hematuria in the context of global migration and travel.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
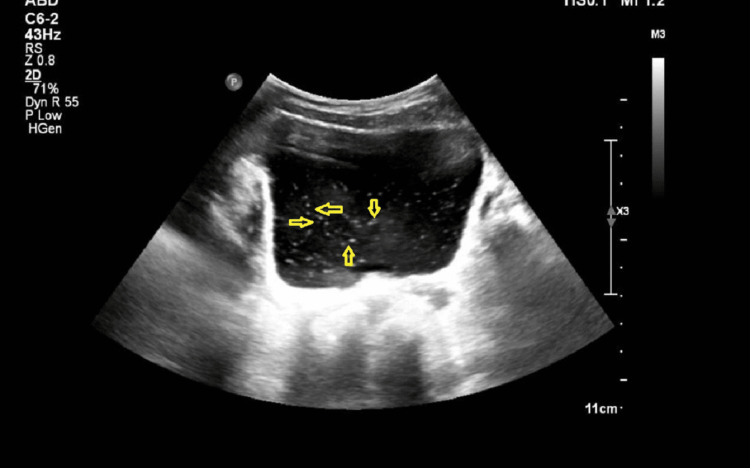 Figure 1
Figure 1 Figure 2
Figure 2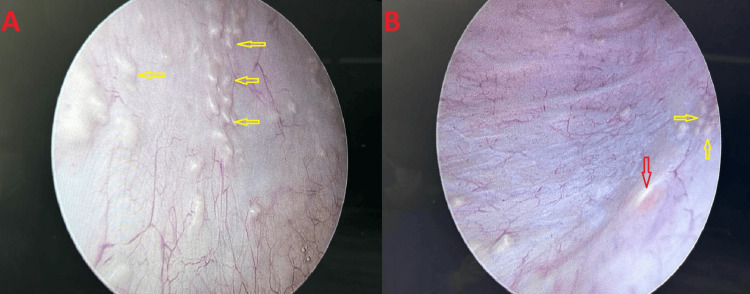 Figure 3
Figure 3| Laboratory parameter | Result | Reference range | Unit |
| Hemoglobin | 11.5 | 10.8–15.6 | g/dL |
| White blood cell (WBC) count | 5.77 | 5.0–13.0 | ×10⁹/L |
| Platelet count | 279 | 170–450 | ×10⁹/L |
| Eosinophils | 4.5 | 1–8 | % |
| Serum creatinine | 0.47 | 0.4–0.7 | mg/dL |
| Serum urea | 20 | 15–38 | mg/dL |
| Serum sodium | 138 | 136–146 | mmol/L |
| Serum potassium | 4.0 | 3.5–5.1 | mmol/L |
| Urine WBCs | 11–15 | < 5 | cells/HPF |
| Urine red blood cells (RBCs) | >100 | < 3 | cells/HPF |
| Laboratory parameter | Result | Reference range | Unit |
| Hemoglobin | 11.2 | 10.8–15.6 | g/dL |
| White blood cell (WBC) count | 8.7 | 5.0–13.0 | ×10⁹/L |
| Platelet count | 271 | 170–450 | ×10⁹/L |
| Eosinophils | 0.8 | 1–8 | % |
| Serum creatinine | 0.44 | 0.4–0.7 | mg/dL |
| Serum urea | 24 | 15–38 | mg/dL |
| Urine WBCs | 0–2 | < 5 | cells/HPF |
| Urine red blood cells (RBCs) | 0–2 | < 3 | cells/HPF |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasites and Host Interactions · Ureteral procedures and complications · Amoebic Infections and Treatments
Introduction
Schistosomiasis is a neglected tropical disease caused by parasitic flatworms of the *Schistosoma *species, affecting individuals primarily in endemic regions. It is classified into urogenital and intestinal forms depending on the infecting species. Schistosoma haematobium is the predominant cause of urogenital schistosomiasis, affecting the bladder and urinary tract, and may lead to hematuria, chronic inflammation, fibrosis, bladder wall calcification, and even malignancy [1]. According to the World Health Organization, more than 200 million individuals are infected worldwide [2], although urogenital schistosomiasis has become exceedingly rare in the Arabian Peninsula due to improved sanitation and eradication programs. In non-endemic settings such as the United Arab Emirates (UAE), imported cases are typically seen in expatriate workers or travelers returning from endemic regions. Delayed diagnosis can result in unnecessary antibiotic use and progression to irreversible bladder damage. This report describes the case of an 11-year-old girl diagnosed with bladder schistosomiasis in the UAE, emphasizing the importance of travel history and early recognition in the diagnostic process [3].
Case presentation
An 11-year-old female patient from Kenya presented to the urology clinic with a six-month history of recurrent painless gross hematuria without clots, associated with storage symptoms including urinary frequency and occasional urgency. She had no relevant medical or surgical history and was otherwise healthy. Although she was born and residing in the UAE, her family reported occasional short visits to Kenya (approximately once every one to two years for brief stays), indicating limited but notable exposure risk in an endemic environment.
Physical examination revealed a hemodynamically stable, afebrile child with a soft, non-tender abdomen and no palpable masses. Laboratory investigations, including complete blood count, renal profile, and electrolytes, were within normal limits, with no eosinophilia or anemia. Urinalysis demonstrated numerous red blood cells and elevated white blood cells, while urine culture demonstrated no bacterial growth, indicating sterile pyuria (Table 1).
Urine cytology was performed early due to persistent painless hematuria despite negative cultures, to evaluate for rare etiologies such as parasitic ova or malignant cells. Cytology revealed Schistosoma haematobium eggs in a hemorrhagic and suppurative background with no malignant features.
Ultrasound of the kidneys, ureters, and bladder (KUB) revealed floating intraluminal echoes within the urinary bladder (Figure 1).
Ultrasound of the kidneys, ureters, and bladder (KUB) revealed floating intraluminal echoes within the urinary bladder (yellow arrows).
CT urography demonstrated thin, patchy calcifications along the inner bladder wall consistent with submucosal calcifications (Figure 2).
CT urography demonstrates thin, patchy calcifications along the inner bladder wall, consistent with submucosal calcifications (red arrows).
Cystourethroscopy was performed under general anesthesia and revealed extensive sandy patches covering the bladder mucosa. Cold-cup biopsies were obtained from both lateral bladder walls, the posterior bladder wall, and the trigone (Figure 3).
Cystoscopic findings in the present case of bladder schistosomiasis.(A) Cystoscopic view of the posterior bladder wall mucosa demonstrating multiple characteristic sandy patches (yellow arrows) consistent with calcified schistosomal egg deposition. (B) Cystoscopic view of the left lateral bladder wall showing sandy patches (yellow arrows) adjacent to the left ureteric orifice (red arrow), with partial visualization of the trigone.
Histopathology demonstrated preserved urothelial morphology with *Schistosoma haematobium *ova associated with a giant-cell reaction, with no evidence of dysplasia or malignancy.
The patient was treated with praziquantel at a single oral dose of 40 mg/kg, repeated after four weeks. Treatment was well-tolerated without adverse effects. At six-month follow-up, she was asymptomatic, and repeat urinalysis and urine cytology showed no Schistosoma haematobium ova. Ultrasound KUB was normal, and renal function remained stable (Table 2).
The family received education about schistosomiasis transmission and prevention. She was placed on long-term surveillance with periodic urinalysis and imaging due to the risk of delayed complications in chronic schistosomiasis.
Discussion
According to the World Health Organization, bladder schistosomiasis, caused by Schistosoma haematobium, remains endemic across several regions of sub-Saharan Africa and the Middle East, including Kenya, Sudan, Tanzania, Uganda, Zimbabwe, Zambia, Togo, Eswatini, Mozambique, and Yemen [4]. Transmission occurs through exposure to freshwater containing infected snails that release cercariae, which penetrate the human skin and then migrate and mature in the circulatory system into adult worms that lay thousands of eggs daily at the venous plexus of the bladder. These eggs penetrate the bladder wall and are released into the urine to continue the life cycle [5,6].
Egg deposition triggers a Th2-mediated immune response characterized by eosinophilic infiltration, resulting in granulomatous inflammation, chronic fibrosis, and bladder wall calcification. Gross hematuria is the earliest and most characteristic manifestation, while dysuria, frequency, suprapubic pain, and secondary infections may also occur. In pediatric populations, the differential diagnosis of painless hematuria includes hypercalciuria, kidney stones, urinary tract infections, strenuous exercise, inherited kidney disorders such as Alport syndrome and thin basement membrane disease, glomerular diseases, and vascular abnormalities such as the Nutcracker syndrome. Chronic schistosomal infection may lead to bladder fibrosis, hydronephrosis, or squamous cell carcinoma [7].
The gold standard for diagnosing urinary schistosomiasis is the detection of Schistosoma haematobium eggs in urine sediment. PCR assays and serology offer high sensitivity and specificity, particularly in patients from non-endemic regions, although accessibility may be limited. Antigen-based tests, such as the circulating cathodic antigen and circulating anodic antigen assays, are still considered investigational. Imaging provides valuable supportive information: ultrasound may reveal bladder wall thickening or upper tract involvement, while CT urography is more sensitive for detecting calcifications or ureteric strictures [8]. Cystoscopic identification of sandy patches is highly suggestive of chronic schistosomiasis. Histopathology confirms the diagnosis by demonstrating schistosomal ova and the associated granulomatous reaction [9].
Reports of urogenital schistosomiasis in the UAE are extremely rare. One case was identified from an online clinical report available on a hospital website, published in May 2025, involving a 41-year-old male patient initially diagnosed with a ureteric calculus. Similar pediatric cases have been described in non-endemic European countries, often diagnosed months after the onset of symptoms, highlighting the diagnostic challenges in low-prevalence settings [3,5].
Praziquantel remains the treatment of choice; it induces spastic paralysis in adult worms, enabling their clearance by host immunity [10,11]. A single oral dose of 40 mg/kg achieves cure rates exceeding 85% and significantly reduces egg excretion. Early diagnosis and treatment are crucial for the prevention of complications such as bladder contracture, ureteric obstruction, and malignant transformation. Given global travel patterns, clinicians in non-endemic areas should maintain a high degree of suspicion, particularly among migrants or travelers from endemic regions [12]. Routine travel history and early cytological investigation can facilitate timely diagnosis [13].
Conclusions
Bladder schistosomiasis, although rare in non-endemic countries, remains an important differential diagnosis for pediatric hematuria. Incorporating epidemiological factors into routine urological assessment is essential for early diagnosis, timely treatment, and the prevention of chronic complications such as fibrosis or malignancy. Long-term follow-up remains essential to detect and manage any delayed complications related to chronic schistosomal inflammation, and ongoing surveillance with periodic clinical and urinary evaluations is recommended to ensure sustained recovery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A rare case of schistosomiasis (bilharzia) of the bladder in a non-endemic area Pol J Radiol Thummar HG Vithlani HI Suthar PP John DR Thummar N Chauhan H 3763788220172879481110.12659/PJR.901140 PMC 5516680 · doi ↗ · pubmed ↗
- 2WHO guideline on control and elimination of human schistosomiasis WHO Guideline on Control and Elimination of Human Schistosomiasis 12 2025 World Health Organization Geneva, Switzerland World Health Organization 2022 https://www.who.int/publications/i/item/978924004160835235279 · pubmed ↗
- 3Pediatric urogenital schistosomiasis diagnosed in France Pediatr Nephrol Percheron L Leblanc C Ulinski T 18931900392024 https://doi.org/10.1007/s 00467-023-06260-x 3821241910.1007/s 00467-023-06260-x · doi ↗ · pubmed ↗
- 4Schistosomiasis: status of endemic countries 12 2025 2024 https://www.who.int/data/gho/data/themes/topics/schistosomiasis
- 5Case report: uncommon presentation of Schistosoma haematobium infection in a migrant patient: diagnostic and therapeutic challenges Front Med (Lausanne) Carraturo F Escolino M Russo A 15832331220254060003610.3389/fmed.2025.1583233 PMC 12209300 · doi ↗ · pubmed ↗
- 6Urinary biomarkers and haematuria as indicators of urogenital schistosomiasis: a systematic review and meta-analysis Acta Trop Vere M Ham-Baloyi WT Oyedele O Mduluza T Melariri PE 10771626920254063379810.1016/j.actatropica.2025.107716 · doi ↗ · pubmed ↗
- 7Schistosomiasis (urinary tract manifestations) 12 2025 2017 https://doi.org/10.53347/r ID-57022
- 8Urinary schistosomiasis in an elderly patient: ultrasonographic findings and case report J Clin Res Rep Sule MB Umar AU Gele IH 1472021