Comprehensive geriatric assessment for people living with HIV and frailty: A mixed‐methods feasibility randomized controlled trial
Natalie St Clair‐Sullivan, Katherine Bristowe, Stephen Bremner, Matthew Maddocks, Richard Harding, Thomas Levett, Jonathan Roberts, Zoe Adler, Peter May, Gary Pargeter, Jaime H. Vera

TL;DR
This study tested a new approach combining geriatric and HIV care for older HIV patients with frailty, finding it feasible and acceptable.
Contribution
The study introduces a joint geriatric-HIV care model and assesses its feasibility in a clinical setting.
Findings
High retention and completion rates of follow-up and outcome measures were observed.
Participants found the Silver Clinic intervention valuable and acceptable.
Recruiting enough frail HIV patients from a single site was challenging.
Abstract
Prevalence of geriatric syndromes including frailty among people living with HIV is increasing and at younger ages. There is no gold standard model of care for people with HIV and frailty. This study aimed to determine the acceptability of a comprehensive geriatric assessment and management plan, delivered jointly by a geriatrician and HIV physician (the Silver Clinic) in outpatient HIV services, and also the feasibility of conducting a randomized controlled trial (RCT) of the Silver Clinic compared with standard care. Mixed‐methods single‐centre, parallel, two‐arm feasibility RCT. People living with HIV ≥50 years old, who screened as frail using the FRAIL scale were randomized to: usual care or the Silver Clinic. Randomization was stratified by age and sex, target N = 84. The primary objective was to determine whether a definitive trial is feasible. Twenty‐five participants (46% of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
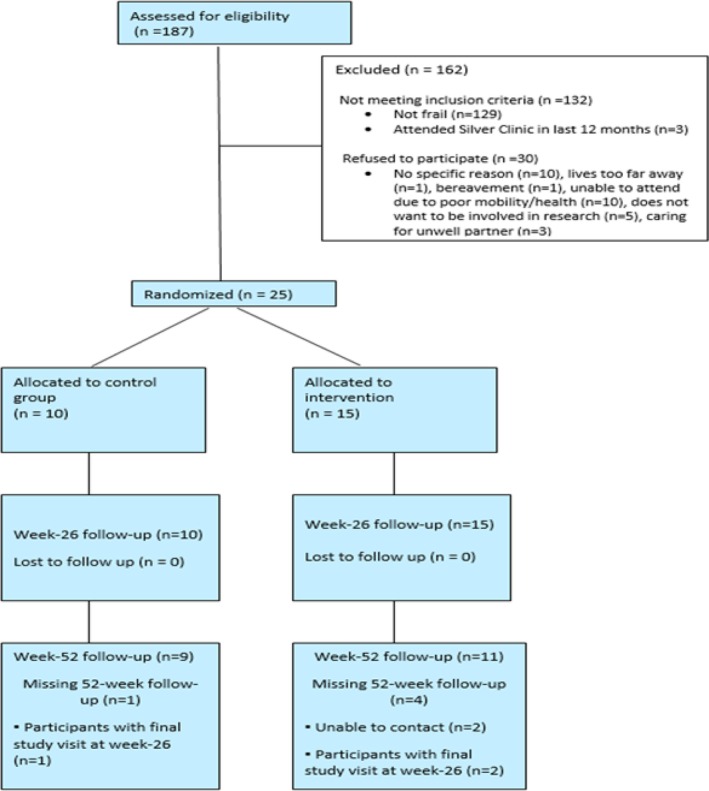 FIGURE 1
FIGURE 1| Intervention | Control | All | |
|---|---|---|---|
| Age (years) | 62.6 (5.95) | 65.1 (6.2) | 63.6 (6.1) |
| Time on ART (years) | 18 [8, 23] | 23 [10.3, 26.8] | 19 [9, 25] |
| On ART | |||
| Yes | 15 (100) | 9 (90) | 24 (96) |
| No | 0 (0) | 1 (10) | 1 (4) |
| Viral Load <40 copies | 15 (100) | 10 (100) | 25 (100) |
| Last CD4 count | 795 [557, 966] | 715.5 [525, 1134.3] | 759 [550, 1006] |
| Time since diagnosis (years) | 24 [14, 25] | 33 [18.2, 37] | 24 [16.5, 34] |
| Fall last 6 months (number) | 1 [0, 6] | 0 [0,2] | 0 [0,4.5] |
| Number of non‐ART medications | 9 [5.0, 10] | 10 [5.6, 10] | 10 [5.5, 10] |
| FRAIL scale score | 3 (3–4) | 3 (3–4) | 3 (3–4) |
| Sexual orientation | |||
| Heterosexual or straight | 1 (6.7) | 0 (0) | 1 (4) |
| Gay or lesbian | 11 (73.3) | 9 (90) | 20 (80) |
| Bisexual | 1 (6.7) | 1 (10) | 2 (8) |
| Other | 2 (13.3) | 0 (0) | 2 (8) |
| Ethnicity | |||
| White British | 11 (73.3) | 9 (90) | 20 (80) |
| Black African | 1 (6.7) | 0 (0) | 1 (4) |
| Black & White Caribbean | 2 (13.3) | 0 (0) | 2 (8) |
| White other | 1 (6.7) | 1 (10) | 2 (8) |
| Charlson Comorbidity Index | 2.7 (1.3) | 3.2 (1.2) | 2.9 (1.3) |
| Number of comorbidities | 6 [5, 9] | 5 [5, 9] | 6 [5, 9] |
| Sex | |||
| Male | 14 (93.3) | 10 (100) | 24 (96) |
| Female | 1 (6.7) | 0 (0) | 1 (4) |
| Gender | |||
| Male | 14 (93.3) | 9 (90) | 23 (92) |
| Female | 1 (6.7) | 0 (0) | 1 (4) |
| Gender fluid | 0 (0) | 1 (10) | 1 (4) |
| Marital status | |||
| Single (never married) | 7 (46.7) | 7 (70) | 14 (56) |
| Married/domestic partnership | 4 (26.7) | 1 (10) | 5 (20) |
| Widowed | 1 (6.7) | 1 (10) | 2 (8) |
| Divorced | 2 (13.3) | 1 (10) | 3 (12) |
| Separated | 1 (6.7) | 0 (0) | 1 (4) |
| Education | 0 (0) | 2 (20) | 2 (8) |
| Primary school | 3 (20) | 3 (30) | 6 (24) |
| Secondary school up to 16 years Higher/further education | 3 (20) | 2 (20) | 5 (20) |
| College or university | 6 (40) | 2 (20) | 8 (32) |
| Post‐graduate degree | 2 (13.3) | 1 (10) | 3 (12) |
| Prefer not to say | 1 (6.7) | 0 (0) | 1 (4) |
| Household annual income | |||
| Below £10 000 | 2 (13.3) | 1 (10) | 3 (12) |
| £10 001–£20 000 | 6 (40) | 6 (60) | 12 (48) |
| £20 001–£30 000 | 1 (6.7) | 2 (20) | 3 (12) |
| £30 001–£40 000 | 0 (0) | 0 (0) | 0 (0) |
| Above £40 000 | 4 (26.7) | 0 (0) | 4 (16) |
| Prefer not to say | 2 (13.3) | 1 (10) | 3 (12) |
| Present home | |||
| Owner occupied/owned outright | 4 (26.7) | 1 (10) | 5 (20) |
| Owner occupied/ mortgage | 1 (6.7) | 1 (10) | 2 (8) |
| Rented housing/council assoc. | 9 (60) | 5 (50) | 14 (56) |
| Rented/private landlord | 1 (6.7) | 3 (30) | 4 (16) |
| Employment status | |||
| Employed, 1–39 h/pw | 0 (0) | 1 (10) | 1 (4) |
| Employed, 40+ h/pw | 0 (0) | 0 (0) | 0 (0) |
| Not employed, not looking | 1 (6.7) | 1 (10) | 2 (8) |
| Retired | 8 (53.3) | 3 (30) | 11 (44) |
| Disabled, not able to work | 5 (33.3) | 5 (50) | 10 (40) |
| Prefer not to say | 1 (6.7) | 0 (0) | 1 (4) |
| Intervention | Control | |||||
|---|---|---|---|---|---|---|
| T1 ( | T2 ( | T3 ( | T1 ( | T2 ( | T3 ( | |
| TUGT^ | 15 [11, 18] | 15 [12, 20] | 12 [10, 16] | 12 [6.8, 20] | 12 [10, 22] | 13 [10, 23] |
| SCRQoL (ASCOT)+ | 0.6 [0.4, 0.74] | 0.5 [0.4, 0.9] | 0.71 [0.4, 0.9] | 0.6 [0.33, 0.74] | 0.6 [0.41, 0.7] | 0.5 [0.4, 0.8] |
| EQ5D5L VAS+ | 50 [50, 65] | 50 [40, 65] | 57 [50, 75] | 58 [39, 65] | 65 [44, 79] | 50 [41, 60] |
| HIV PROM+ | 30.7 (7.1) | 28.7 (10.0) | 28.3 (9) | 29.0 (9.3) | 24.8 (8.4) | 25.5 (12.2) |
| MOCA+ | 26 [24, 27] | 25 [23, 26.3] | 26 [24, 27] | 26.5 [23, 28.3] | 24 [21, 27] | 25 [24, 28] |
| FRAIL scale^ | 3 [3, 3] | 3 [3, 3] | 3 [2, 3] | 3 [3, 3] | 3 [2, 3.3] | 2 [2, 3] |
| FRIED^ | 3 [3, 3] | 3 [3, 3] | 3 [3, 3] | 3 [2, 3] | 3 [2, 3] | 3 [2, 3] |
| Hospital days | 0 (0) | 1 (4) | 0 (0) | 0 (0) | 2.4 (7) | 1.2 (4) |
| GP contacts | 4 (3.1) | 1.5 (2) | 3 (4) | 1 (1) | 1 (2) | 8.1 (20.3) |
| Consultant contacts | 1.8 (1.2) | 2 (1.6) | 1.5 (1.4) | 1 (1) | 1.3 (1.1) | 1.7 (1.3) |
| AHP contacts | 2.3 (7.4) | 1.1 (3.1) | 1.1 (3) | 0.1 (0.3) | 0.1 (0.3) | 2.4 (7) |
| Experiences of participating in the trial |
‘
|
| Feelings around outcomes measures |
‘
|
| Experiences of the Silver Clinic |
|
| Ways to improve the Silver Clinic |
|
- —National Institute for Health and Care Research10.13039/501100000272
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV-related health complications and treatments · Frailty in Older Adults · HIV/AIDS Research and Interventions
INTRODUCTION
Ageing people living with HIV face a higher burden of comorbidities, social care challenges and geriatric conditions, such as frailty and cognitive decline, compared with the general population [1]. These significantly impact mental well‐being, functional capabilities and quality of life, and increase healthcare utilization and associated costs [2].
There is no gold standard model of care for the management of people living with HIV and frailty [3]. While there is growing recognition of the need to address geriatric syndromes within HIV care settings [4], existing HIV care provision lacks the necessary expertise or resources to manage geriatric syndromes effectively [5]. The European AIDS Clinical Society now recommends routine frailty screening for people living with HIV aged 50 and above, followed by a comprehensive geriatric assessment for those identified as frail [6]. The comprehensive geriatric assessment, the gold standard for managing frailty in older people, is a multidimensional assessment of an older person, including health and well‐being, to create an individualized care plan [7]. However, published data from geriatric clinics for people living with HIV are limited, and there is little evidence to support the efficacy of frailty screening, or the role of the comprehensive geriatric assessment in improving health outcomes for people living with HIV [5, 8].
This study aimed to determine the acceptability of a comprehensive geriatric assessment and frailty management plan, delivered jointly by a geriatrician and HIV physician (the Silver Clinic) in outpatient HIV services, and the feasibility of conducting an randomized controlled trial (RCT) of the Silver Clinic compared with standard care. Specifically, it examined the feasibility of trial procedures and participant retention, initial cost and service utilization analysis and areas for refinement in referral pathways, clinic frameworks and intervention strategies.
METHODS
Study design
A UK‐based mixed‐methods single‐centre, parallel, two‐arm feasibility RCT among older people living with HIV (≥50 years old), screened as frail using the FRAIL scale. Participants were randomized to either the intervention group (comprehensive geriatric assessment and management plan, delivered jointly by a geriatrician and HIV physician in outpatient HIV services, known as the ‘Silver Clinic’) or standard care. A full description of the protocol is available elsewhere [9].
Setting
Participants were recruited from the HIV unit at the Royal Sussex County Hospital, Brighton, UK.
Recruitment
All potentially eligible patients who attended their routine HIV annual health visit during the study recruitment period were identified and screened. This visit is a standard procedure, as part of usual HIV care in the United Kingdom. Performed by nurses, it encompasses weight assessment, blood pressure monitoring, urinalysis, mental health evaluation, sexual health screening, adherence assessment, cervical cytology and contraception review. During this assessment, individuals aged 50 and above underwent frailty screening utilizing the FRAIL scale [10]. 1572/2457 (64%) attending the Lawson Unit are 50 years and over and 60 (4%) are women [11]. The FRAIL scale was selected due to it being recommended by the European AIDS Clinical Society, its ease of use, and that it does not have space implications within the clinic [11]. Telephone‐based frailty screening was also conducted with participants from a previous study who had consented to be contacted, and patients that were identified as pre‐frail the previous year were rescreened. Those exhibiting signs of frailty on screening were informed about the study and, if interested, connected with a research assistant or nurse to provide further information, and address any queries. Written informed consent was obtained before any data collection commenced at their baseline visit.
Inclusion criteria
- People living with HIV aged 50 years or older with evidence of frailty, scoring 3+ on the FRAIL scale.
- Able to provide informed consent.
- Consented to their general practitioner being informed about participation.
Exclusion criteria
- People living with HIV aged <50 years old or not defined as frail.
- Attended the Silver Clinic previously during the last 12 months.
Data collection
Data were collected simultaneously in both groups at baseline (T1), 26 weeks (T2, primary end point) and 52 weeks (T3) using standardized clinical outcome measures. Due to challenges in recruitment, the initial recruitment period was extended by 2 months. Due to time restrictions, those recruited after September 2022 had only T1 and T2 follow‐ups. The Montreal Cognitive Assessment (MoCA) was initially planned to be conducted at T1 only. Subsequent ethical approval was obtained to include the MoCA at T2 and T3 after the trial had commenced.
Patient demographic and characterization data
Baseline demographic data were collected including personal characteristics (age, gender, sex at birth, ethnicity, sexual orientation) and social determinants of health (marital status, employment status, residential status, formal education level, annual income) and comorbidities.
Feasibility outcomes
Primary outcome
To determine whether a definitive trial is feasible, assessed by:
- Recruitment rate
- Study retention
- Completion of study outcome measures
Secondary outcomes
Frailty and patient‐reported outcome measures
Secondary outcomes were captured at all time points (T1, T2 and T3) via standardized clinical outcome measures that represent multiple health and healthcare service domains. The Timed Up and Go test (TUGT) is used to assess functional mobility and falls risk [12]; the Adult Social Care Outcomes Toolkit (ASCOT) measures social care‐related quality of life [13]; the EuroQol EQ‐5D5L measures health‐related quality of life [14]; the Positive Outcomes HIV PROM (HIV PROM) measures multidimensional symptoms and concerns for people living with HIV [15]; the MoCA assesses early detection of mild cognitive impairment [16]; the Consultation and relational empathy measure (CARE) is used to assess interpersonal quality of healthcare encounters [17]; the FRAIL scale and the Fried Frailty Phenotype [18] are used to assess physical frailty.
Health service use
The Client Service Receipt Inventory (CSRI) [19] captures planned and unplanned contact with general practitioners, hospital and emergency department attendance and admissions, and informal care by family and/or friends, to measure the costs of caring for older people living with HIV and frailty.
Description of interventions
Intervention arm: The Silver Clinic
The Silver Clinic is a pre‐existing, joint HIV–ageing outpatient service that was first established in 2012 to address the emerging needs of older adults living with HIV. The Silver Clinic consists of a comprehensive geriatric assessment and management plan, delivered jointly by a geriatrician and HIV physician in outpatient HIV services at the Royal Sussex County Hospital. The clinic uses a comprehensive geriatric assessment approach that involves the comprehensive evaluation and management of geriatric syndromes commonly observed in older people living with HIV, such as frailty, falls, polypharmacy, multimorbidity and medication‐related issues associated with antiretroviral therapy (ART) [9]. Additionally, the intervention provides support for older people living with HIV facing social and psychological challenges by devising patient‐centred health interventions including physical activity promotion and peer support. Each clinic appointment involves a structured process comprising history‐taking, physical examination, collection of blood samples, medication review, cognitive assessment and evaluation of social and mental health aspects. An individualized care plan is formulated and communicated to the patient's primary care provider or HIV physician for coordination of care. All participants had a separate general practitioner.
The clinic operates on a monthly basis offering individual appointments of 40 min to up to 16 patients per month. Follow‐up requirements are determined by the Silver Clinic physicians, in line with the needs of the patient. Silver Clinic appointments are offered both in‐person and virtually to ensure ease of access to the service.
Control arm: Standard care
Participants randomized to the control arm continued to receive routine healthcare services from their HIV physician, general practitioner and community resources as per standard practice (see Figure 1). All participants had a separate general practitioner. HIV standard care is typically provided twice a year, with primary care services predominantly accessed upon patient request. Participants were provided with information regarding frailty and consented to the disclosure of their frailty assessment outcomes to their GP and HIV physician. They received general healthy ageing advice but did not have access to the intervention during the study. Upon completion of the 12‐month study period, control group participants were offered an opportunity to attend the Silver Clinic.
CONSORT flow diagram.
Randomization and blinding
After baseline assessment, the research assistant randomized participants using REDCap in a 1:1 allocation using randomly permuted blocks to receive standard care (control arm) or referral to the Silver Clinic (intervention arm), stratifying by age (50–65, 66–80, 81–95) and sex at birth to ensure a balanced sample in both arms. Participants were informed of their study arm in person and those allocated to the intervention arm were booked into the Silver Clinic within 6 weeks.
A priori progression criteria to a definitive trial
To guide decisions on trial feasibility, we established the following a priori progression criteria. Meeting these thresholds indicated the study could progress to a definitive trial without substantive changes.
- Recruitment of 60% of eligible patients;
- Recruitment of 84 patients within 3 months; from first patient randomized;
- Retention of 70 patients (allowing up to 15% attrition) to primary end point (6 months); and
- Outcome measure completion for 90% of available participants at each time point.
Sample size
To accurately estimate the standard deviation of the primary outcome for the subsequent trial, it is recommended to have a minimum of 35 participants per arm [20, 21]. Considering our local patient population (total cohort of 2450; 54% aged over 50), we planned to recruit 42 patients per group, totalling 84 participants overall, with a 15% allowance for attrition, allowing us to estimate retention to within approximately ±8% with 95% confidence.
Statistical analysis
Baseline characteristics of the participants were summarized using descriptive statistics. Normally distributed variables were summarized by their means and SD, skewed continuous variables by their medians and interquartile ranges and categorical variables by their frequencies and percentages. For the feasibility outcomes, the proportion of patients recruited, participants retained and data completeness were analysed and summarized in line with the a priori progression criteria and 95% CIs are presented.
Explanatory qualitative interviews
We aimed to interview up to 15 participants from each arm of the trial, via purposive sampling to examine experiences of: recruitment to the trial, management of their priority concerns during the course of the trial, referral to the Silver Clinic, the description of comprehensive geriatric assessment, experience of the Silver Clinic and perceived impact on priority outcomes (intervention arm only), satisfaction with care and acceptability of participating in an RCT of the Silver Clinic intervention. Due to recruitment challenges for the main trial, a decision was made to invite all trial participants to participate in a qualitative interview in order to ensure sufficient information power to address the aim of the study [22].
Qualitative analysis
Interviews were audio‐recorded, transcribed verbatim and analysed using reflexive thematic analysis, using the six‐phase process [23, 24]. Commencing with immersion in the data the second phase involved generating initial codes, which are refined through an iterative process into themes and sub‐themes in the subsequent phases, to accurately depict the participants' experiences [25]. Coding was led by a physiotherapist (NS) with experience in qualitative research and overseen by the qualitative lead for the study (KB). The themes and findings were reviewed and refined with the study team.
Patient and public involvement
Patient and public involvement was embedded through the development and conduct of the study, including recruitment strategies and participant‐facing materials, and dissemination of study findings.
Ethical approval
Ethical approval was granted by East Midlands–Leicester Central Research Ethics Committee (reference 21/EM/0200). The study was registered at www.isrctn.com (ISRCTN14646435).
RESULTS
Recruitment and retention
Recruitment took place between November 2021 and March 2023. The last participant visit was completed in September 2023. Of n = 187 individuals assessed for eligibility, n = 162 (86.7%) were not eligible (n = 129 did not screen as frail, n = 3 had attended the Silver Clinic in the last 12 months). Of the n = 55 who were eligible, n = 30 (54.5%) declined to take part (n = 10 gave no specific reason, n = 1 lived too far away, n = 1 had experienced a bereavement, n = 10 were unable to due to poor health/mobility, n = 5 did not want to be involved in research and n = 3 were caring for an unwell partner). N = 25 (45.5%, 95% CI = 32.0, 59.4) were recruited and randomly allocated to intervention (n = 15) or usual care (n = 10) (Figure 1). One hundred percent of participants attended their T2 follow‐up (primary endpoint) and 91.0% at T3.
Participant characteristics
Most participants were male (99%) and White (88%), with a median (IQR) age of 64 (54–79) years. Participants had been living with HIV for a median (IQR) of 24 (16.5, 34) years, on ART for a median (IQR) of 19 (9, 25) years, a median (IQR) of 6 (5, 9) comorbidities. See Table 1 for baseline characteristics by randomized group.
Completion rates for outcome measures
99.7% of outcome measures were completed at baseline, 99.0% at T2 and 90.2% at T3. Data were missing in the TUGT (4% at T2, 17.2% at T3), due to a participant not being able to physically walk that distance, a participant who felt too frail to attend their T2 and T3 visit in person and two participants not attending their T3 visit (reason unknown). As the follow‐up MoCAs were introduced as an amendment to the study, two MoCAs (8%) were not completed at T2, due to those participants already having had their T2 visit and two MoCAs (9.1%) were not completed at T3 due to participants not attending.
Outcome measure results
Overall, satisfaction with care was high in all areas of the CARE measure, with ≥70% rating their practitioner as excellent, very good or good at T2 and T3 visits (see Appendix A). Improvements were seen in the intervention arm in the TUGT (T1 = 15, T3 = 12), ASCOT (T1 = 0.6, T3 = 0.71) and the EQ5D5L VAS (T1 = 50, T3 = 57), at T3 rather than T2 (Table 2). The intervention arm also reported fewer hospital days, GP contacts, consultant contacts and Allied health professional contacts between T1 and T3.
Trial qualitative interview findings
All but one participant from the main trial completed qualitative interviews (telephone n = 17, video call n = 1, HIV research unit n = 6), after their T2 study visit. The sample consisted of 22 men, one woman and one person who identified as gender fluid. Interviews lasted up to 1 h (range 35–60 min).
Interviews revealed that participants found the trial processes and communication to be acceptable and clear. Participants largely described a feeling of neutral acceptance towards the outcome measures and questionnaires used during the trial, often describing them as ‘fine’ and ‘par for the course’. However, participants discussed how they may identify issues that they themselves may not have been aware of. Overall participants described their experiences of attending the Silver Clinic as positive, particularly in relation to their mental well‐being. Suggestions on how to improve the Silver Clinic were centred around improving linkage of care and increasing follow‐up appointments (e.g., quotes see Table 3).
DISCUSSION
Key findings
This study aimed to determine the acceptability of a comprehensive geriatric assessment and management plan, delivered jointly by a geriatrician and HIV physician (the Silver Clinic) in outpatient HIV services, and the feasibility of conducting an RCT of the Silver Clinic compared with standard care. We found that due to recruitment challenges, conducting a full‐scale RCT using the current methodology would not be feasible. However, all other trial progression criteria were met, including high participant retention (100% at 6 months and 91% at 12 months) and high rates of outcome measure completion (99.7% at baseline, 99% at 6 months, 90.2% at 12 months). Our qualitative findings further support the acceptability of the study processes and outcome measures, with participants expressing positive experiences, including enjoyment of their study visits. Those in the intervention arm uniformly reported that attending the Silver Clinic was beneficial and considered it a valuable addition to their HIV care. Participants also provided useful feedback on potential improvements to the intervention, including direct access to test results, improved coordination of care and more frequent follow‐ups. Consistent with previous research, these findings underscore the interconnected nature of physical and mental health and highlight the potential for physical health interventions to confer secondary benefits on mental well‐being [26, 27]. The potential for the term frailty to be perceived as stigmatizing is an important issue within both people living with HIV and care provider communities. As we have explored these issues in depth elsewhere [28, 29], the present paper focuses on feasibility outcomes. This study also demonstrated that screening people living with HIV aged ≥50 years using the FRAIL scale was both feasible and acceptable to participants. Identification of frailty is particularly critical, as frailty has been shown to predict poor health outcomes and is negatively associated with adherence to ART [30]. While multiple frailty screening tools exist, there is no consensus on which is a ‘gold standard’ tool [31] and is reliable and simple enough for routine clinical settings [32]. Additionally, there are no screening tools that are validated in people living with HIV [33] and many that are validated are in populations that are 65 years or over [34]. Evidence suggests that the Fried Frailty Phenotype is not suited for implementation in large‐scale population studies or busy clinics and that short, rapid instruments are more appropriate [31]. It is also important to recognize that the FRAIL scale is a screening tool, whereas the diagnosis of frailty typically relies on the Frailty Phenotype or other established diagnostic metrics. Analysis of secondary outcomes suggests that frailty screening and management pathways may contribute to improved health outcomes over the longer term, with benefits observed at 12 rather than 6 months. This highlights the importance of extending trial durations when evaluating interventions for conditions such as frailty, where improvements in physical function and adaptation to new management strategies may take longer to manifest [35, 36]. While these findings should be interpreted with caution due to the small sample size and feasibility focus of the study, they provide a foundation for future hypothesis‐driven research and underscore the necessity of conducting a definitive RCT of a comprehensive geriatric assessment for older people living with HIV with frailty.
Although evidence for the use of the comprehensive geriatric assessment in pre‐frail populations is limited, including among people living with HIV, pre‐frailty is increasingly recognized as a ‘warning sign’ for impending frailty [31] and therefore represents an important window for identification and timely intervention to reduce the risk of further deterioration. As pre‐frail individuals are at increased risk of becoming frail within 3–4 years [37], early recognition and intervention are likely to provide the greatest benefit [38, 39]. In people living with HIV, early identification of frailty could enable access to interventions that may delay or reverse progression, thereby reducing disability, hospitalization and mortality [40]. Future work should examine how the comprehensive geriatric assessment might be optimally delivered in this context and its potential role in addressing pre‐frailty.
To improve the feasibility of a future trial, we propose expanding recruitment criteria to include pre‐frail individuals, who comprise an estimated 25–30% of people living with HIV aged ≥50 years [41]. Screening for and intervening in pre‐frailty offers an opportunity to slow or reverse frailty progression, particularly among individuals in their 50s who may be more receptive to interventions aimed at maintaining long‐term health. A shift from a reactive to a proactive model of care may therefore be more appropriate and acceptable [42]. Additionally, recruitment is expected to improve as clinical services resume face‐to‐face appointments, particularly for individuals with complex healthcare needs. Expanding the number of trial sites offering a comprehensive geriatric assessment will also enhance recruitment and generalizability.
Strengths and limitations
This study has several limitations. Participants were not blinded to their group allocation, although HIV physicians and geriatricians conducting the Silver Clinic were unaware of who the trial participants were. The sample predominantly comprised White males, reflecting the ongoing issue of underrepresentation of women in HIV clinical trials [43]. Future trials should prioritize inclusive recruitment strategies, such as extending research sites to diverse geographical locations, engaging women's health specialists and collaborating with women's advocacy groups to build trust and encourage participation [44].
Recruitment fell short of expectations due to delays associated with the COVID‐19 pandemic, including staff redeployment, hospital service disruptions and patient reluctance to attend in‐person visits. To mitigate these challenges, we extended the recruitment period (resulting in some participants receiving only 6 months of follow‐up), recruited patients who had participated in previous studies, rescreened individuals previously identified as pre‐frail, and implemented telephone‐based frailty screening. These adaptations demonstrated the feasibility and acceptability of administering the FRAIL scale remotely, offering a time‐efficient alternative with minimal implications for clinic space.
Missing outcome data were primarily attributed to participant mobility limitations, which affected their ability to attend study visits or complete assessments, an issue commonly observed in frailty‐related research [45]. This highlights the importance of offering flexible means to participation (in person or virtually) for a future trial. While missing data in frailty measures may serve as an indicator of frailty severity, it could also result in misclassification, with participants being categorized as pre‐frail rather than frail due to an inability to complete certain measures. Furthermore, while the FRAIL scale demonstrated feasibility and acceptability, further validation against other screening tools is warranted to ensure optimal accuracy and reliability.
Despite these limitations, this study provides valuable new insights. High participant satisfaction with both trial procedures and the Silver Clinic intervention reinforces the acceptability of the study design. Additionally, the successful use of telephone‐based FRAIL screening highlights the potential for integrating remote screening methods into future frailty‐related trials. Key considerations for a definitive RCT include optimizing recruitment strategies, offering flexible participation options (virtual and in‐person), refining screening methodologies and minimizing missing data during assessments.
CONCLUSION
While recruitment to a full‐scale RCT is not feasible using the current methodology, retention rates and study outcome completion were exceptionally high. Future trials should adopt a proactive recruitment strategy by expanding the number of study sites, potentially expanding to include pre‐frail individuals, and incorporating flexible participation options. These adaptations may enhance feasibility and ensure broader applicability. A definitive RCT remains essential to evaluate the effectiveness of the comprehensive geriatric assessment in improving health outcomes for older people living with HIV with frailty. If successful, this work could inform the integration of comprehensive geriatric assessment within routine HIV outpatient care, ultimately supporting healthy ageing and improved quality of life in this population.
AUTHOR CONTRIBUTIONS
JV was the grant award holder and chief investigator, and KB was the principal investigator and provided project oversight. JV, KB, NS, MM, RH, SB, TL and GP contributed to the study design. NS collected the data and data analysis was led by NS, KB, JV and SB. NS drafted the first version of the manuscript. All authors contributed to the interpretation of the data revised the manuscript and gave final approval of the manuscript.
FUNDING INFORMATION
This project is funded by the National Institute for Health and Care Research (NIHR) under its Research for Patient Benefit (RfPB) Programme (Grant Reference Number NIHR201060). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
CONFLICT OF INTEREST STATEMENT
The authors have no conflicts of interest to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sarma P , Cassidy R , Corlett S , Katusiime B . Ageing with HIV: medicine optimisation challenges and support needs for older people living with HIV: a systematic review. Drugs Aging. 2023;40:179‐240.36670321 10.1007/s 40266-022-01003-3PMC 9857901 · doi ↗ · pubmed ↗
- 2Greene M , Shi Y , Boscardin J , Sudore R , Gandhi M , Covinsky K . Geriatric conditions and healthcare utilisation in older adults living with HIV. Age Ageing. 2022;51(5):1‐9.10.1093/ageing/afac 093PMC 927123435511728 · doi ↗ · pubmed ↗
- 3Davis AJ , Greene M , Siegler E , et al. Strengths and challenges of various models of geriatric consultation for older adults living with human immunodeficiency virus. Clin Infect Dis. 2022;74(6):1101.34358303 10.1093/cid/ciab 682PMC 8946774 · doi ↗ · pubmed ↗
- 4Kehler DS , Milic J , Guaraldi G , Fulop T , Falutz J . Frailty in older people living with HIV: current status and clinical management. BMC Geriatr. 2022;22(1):919.36447144 10.1186/s 12877-022-03477-7PMC 9708514 · doi ↗ · pubmed ↗
- 5Kokorelias KM , Grosse A , Zhabokritsky A , Sirisegaram L . Understanding geriatric models of care for older adults living with HIV: a scoping review and qualitative analysis. BMC Geriatr. 2023;23(1):417.37422631 10.1186/s 12877-023-04114-7PMC 10329351 · doi ↗ · pubmed ↗
- 6European AIDS Clinical Society . EACS Guidelines Version 11.0. 2021 https://www.eacsociety.org/media/final 2021 eacsguidelinesv 11.0_oct 2021.pdf
- 7Garrard JW , Cox NJ , Dodds RM , Roberts HC , Sayer AA . Comprehensive geriatric assessment in primary care: a systematic review. Aging Clin Exp Res. 2020;32:197‐205.30968287 10.1007/s 40520-019-01183-w PMC 7033083 · doi ↗ · pubmed ↗
- 8Jones HT , Levett T , Barber TJ . Frailty in people living with HIV: an update. Curr Opin Infect Dis. 2022;35(1):21‐30.34799510 10.1097/QCO.0000000000000798 · doi ↗ · pubmed ↗