Global quality of care trends for lip and oral cavity cancer: A quality of care index analysis, 1990–2021
Yilin Zhang, Wenkai Xu, Haocheng Wang, Liang Mao, Jing Sun

TL;DR
This study analyzed global trends in lip and oral cavity cancer care quality from 1990 to 2021, finding improvements but persistent disparities linked to socioeconomic factors.
Contribution
The novel Quality of Care Index (QCI) was developed to assess global disparities in lip and oral cavity cancer care.
Findings
Global care quality improved from 1990 to 2021, but disparities persist.
High-income regions had high incidence, while low-income areas had high mortality.
Females consistently had higher care quality scores than males.
Abstract
To evaluate global trends and disparities in the quality of care for lip and oral cavity cancer (LOCC) from 1990 to 2021 using the Quality of Care Index (QCI). Data on LOCC burden were obtained from the Global Burden of Disease (GBD) 2021 study, covering 204 countries and territories from 1990 to 2021. The QCI was constructed via principal component analysis of four component indices: mortality-to-incidence ratio, prevalence-to-incidence ratio, years of life lost to years lived with disability ratio, and disability-adjusted life years to prevalence ratio. Analyses were stratified by socio-demographic index (SDI), age, and sex. A geographical decoupling was observed: high-SDI regions had the highest LOCC incidence, while low-middle SDI regions had the highest mortality. The global QCI improved from 1990 to 2021 but strongly correlated with national development. Females consistently had…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
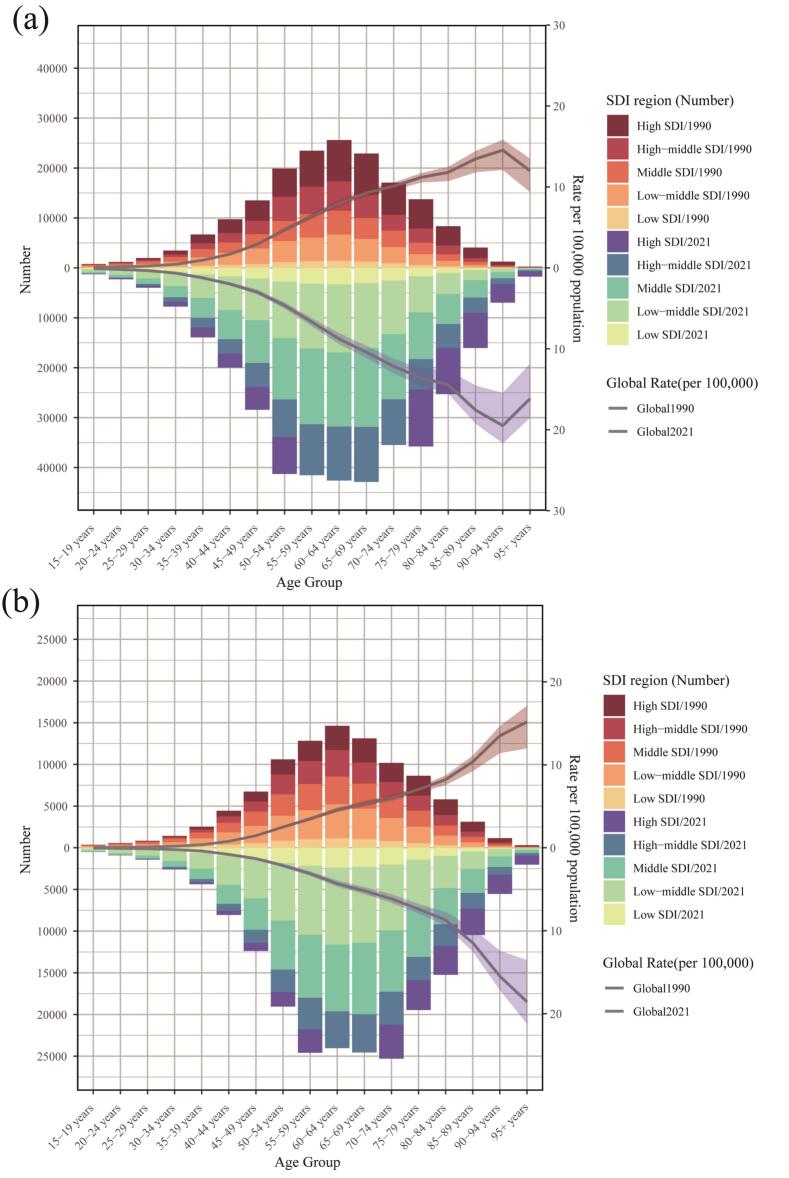 Figure 1
Figure 1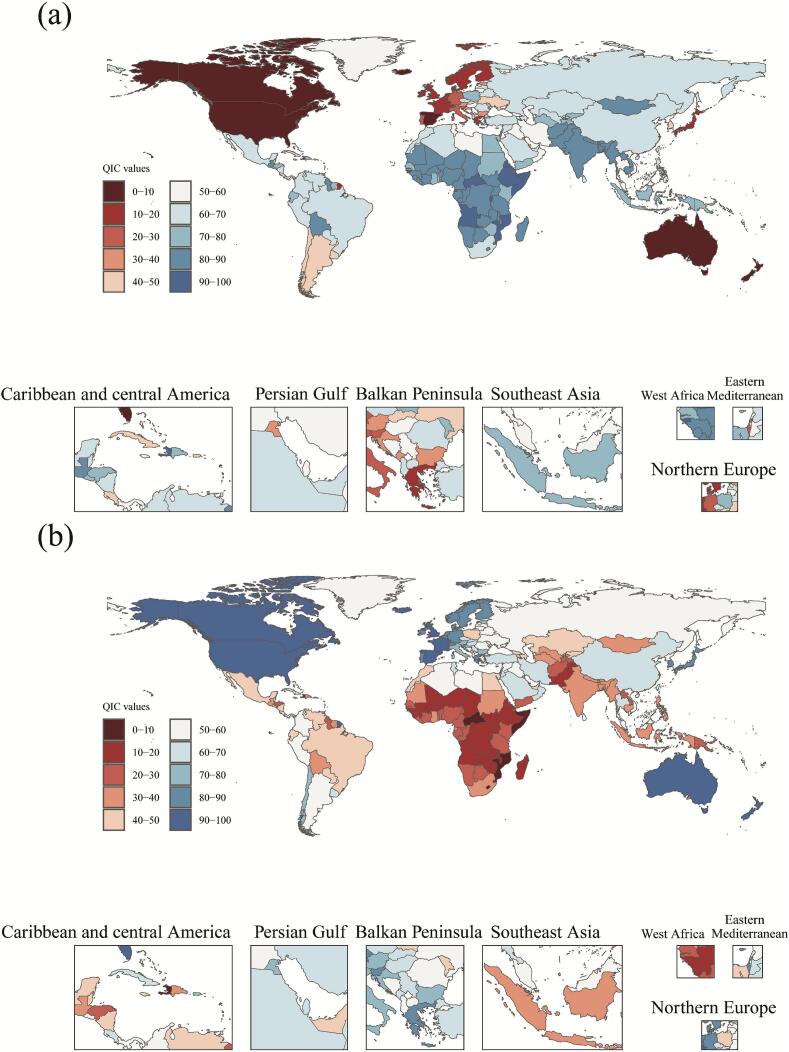 Figure 2
Figure 2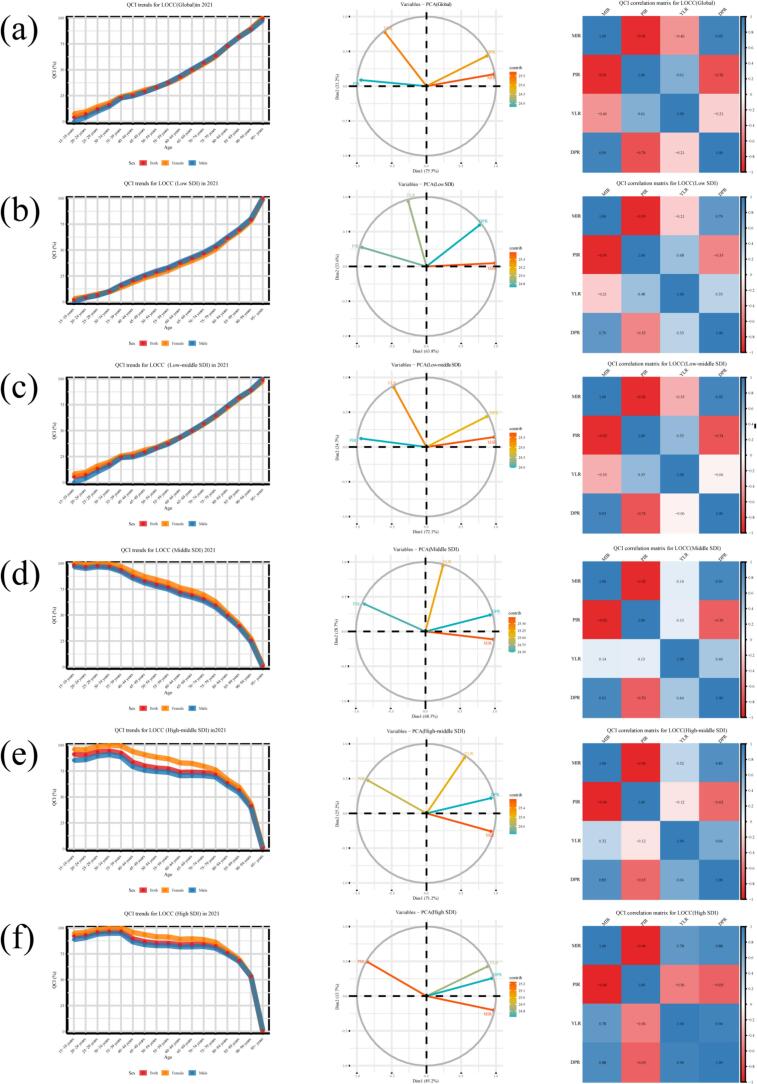 Figure 3
Figure 3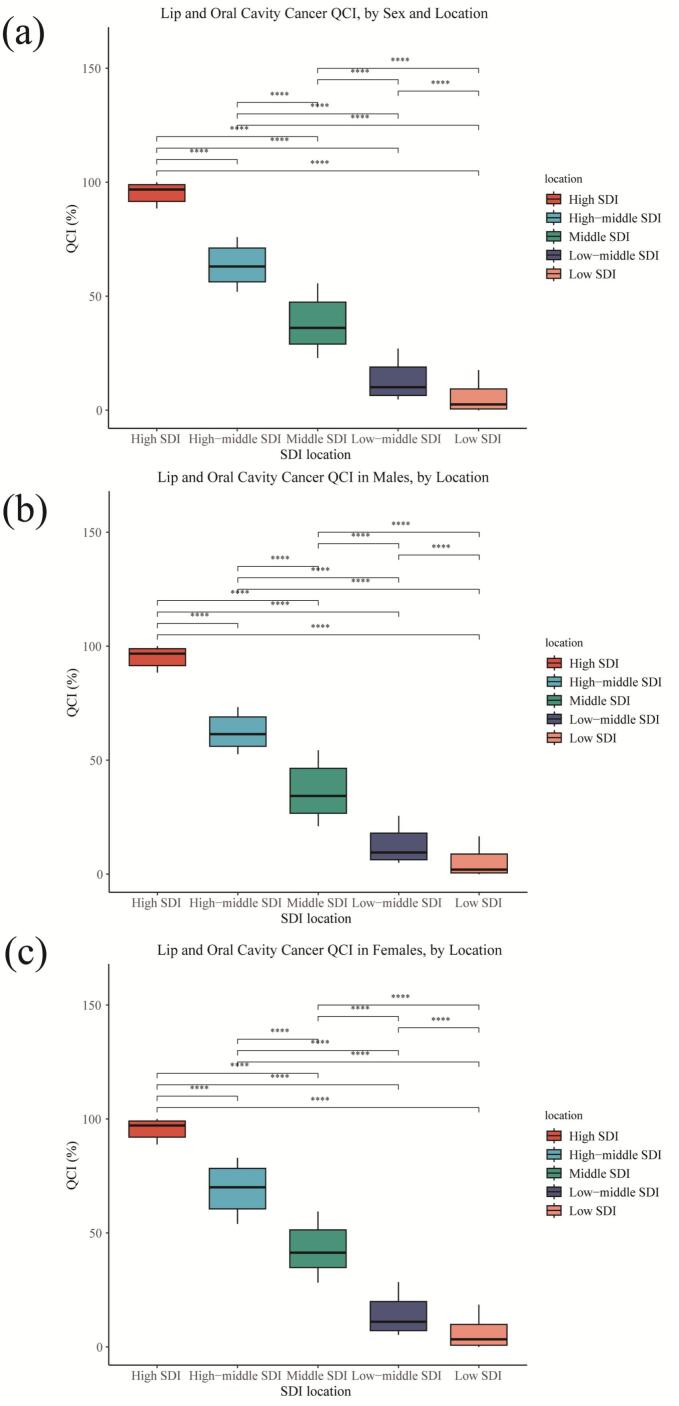 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHead and Neck Cancer Studies · Cleft Lip and Palate Research · Oral Health Pathology and Treatment
Introduction
1
LOCC represents a significant global public health challenge(GBD 2017 Oral Disorders Collaborators and Bernabe, 2020). As the most common subtype of head and neck cancers, it is associated with substantial morbidity, mortality, and detrimental impacts on essential functions such as speech and swallowing(Chen et al., 2025). According to the GBD studies, LOCC affected over 1.54 million people worldwide in 2021(Alves-Costa et al., 2025). The burden exhibits notable disparities linked to geographic region, socioeconomic status, and healthcare access(Fan et al., 2022), compounded by risk factors like tobacco and alcohol use(Dai et al., 2025).
Extensive epidemiological studies and cancer registries have detailed LOCC incidence and mortality(GBD, 2023 Cancer Collaborators and, 2025). However, these metrics primarily reflect disease burden rather than healthcare system performance in prevention and treatment(Pan et al., 2025). A critical gap remains in quantitatively assessing the quality of LOCC care globally(Bi et al., 2025).
To bridge this gap, the QCI, a composite metric derived from GBD data, has been developed(Luo et al., 2025). The QCI synthesizes several key health metrics into a single, interpretable score, enabling a standardized, comparative assessment of healthcare quality across different geographies and over time(Xu et al., 2025). The longitudinal data (1990–2021) are crucial for evaluating trends in care quality, which evolve slowly with health system development. The GBD 2021 estimates remain the most recent comprehensive global data, ensuring contemporary relevance for policy. Therefore, this study aims to assess global and regional trends in the quality of care for LOCC from 1990 to 2021 using the QCI, examine disparities by SDI, age, and sex, and identify policy-relevant patterns that may inform equitable cancer control strategies.
Methods
2
Study design and population
2.1
Ethical statement: This study used publicly available, anonymized data from the GBD 2021 study and was exempt from ethical review approval at our institution.
The Global Burden of Disease 2021 study offers a comprehensive evaluation of the health impacts of 371 diseases and injuries, encompassing 204 countries and territories(GBD 2021 Diseases and Injuries Collaborators, 2024). Within the framework of this study, LOCC was delineated by the ICD-10 codes C00 through C08(Yu et al., 2024). All data, models, and methods are available via the GBD 2021 repository: https://ghdx.healthdata.org/gbd-2021/sources.
Our analysis was based on LOCC data from the GBD study (1990–2021), encompassing 204 countries and territories. The metrics extracted included incidence, mortality, prevalence, years of life lost (YLLs), years lived with disability (YLDs), and disability-adjusted life years (DALYs), alongside demographic variables(GBD 2021 Diseases and Injuries Collaborators, 2024). The SDI, a composite indicator of a country's development level (ranging from 0 to 1), was used for stratification(GBD 2019 Healthcare Access and Quality Collaborators, 2022). According to the GBD framework, study units were grouped into five SDI regions. Data for individuals under 15 years of age were excluded at the point of extraction from the GBD repository; therefore, all subsequent analyses, including the calculation of component indices and the PCA, were based solely on the population aged 15 years and older.(Alves-Costa et al., 2025).
Measures
2.2
The incidence and deaths of LOCC globally and across the five SDI regions in 2021 were summarized and compared.
This study employed four key ratios derived from GBD data to indirectly assess the quality of care for LOCC(Ghamari et al., 2022). The Years of life lost to Years lived with disability Ratio (YLR) distinguishes between diseases causing primarily premature death (high YLR) and those leading predominantly to disability (low YLR)(Azadnajafabad et al., 2023). The Mortality to Incidence Ratio (MIR) directly reflects the lethality of the disease and the effectiveness of medical interventions, with a lower MIR signifying more effective care(Choi et al., 2017). The Disability-adjusted life years to Prevalence Ratio (DPR) evaluates the severity of the disease at the population level; a high DPR indicates that even with low prevalence, the disease imposes a severe health burden. Lastly, the Prevalence to Incidence Ratio (PIR) sheds light on the disease duration, where a high PIR is characteristic of chronic conditions, and a low PIR suggests an acute disease process(Sofi-Mahmudi et al., 2021). These indices were calculated from the GBD estimates as follows: MIR = Deaths / Incidence; PIR = Prevalence / Incidence; YLR = YLLs / YLDs; DPR = DALYs / Prevalence(Ghafouri et al., 2023).
Statistical analysis
2.3
Data preprocessing was conducted to ensure robustness. Instances with zero denominators in the calculation of these ratios were handled by setting the resulting ratio to zero. Subsequently, all calculated values for MIR, PIR, YLR, and DPR were checked for infinite, missing, or extreme outlier values; all such instances were recoded to zero.(Ringnér, 2008). Prior to dimensionality reduction, the four component indices were standardized using Z-score normalization (mean-centered and scaled to unit variance) to account for differences in their scales and variances. Principal Component Analysis (PCA) was then performed on the standardized matrix. The PCA calculation was implemented using the prcomp function from the R stats package, while the factoextra package was employed for the visualization of PCA results. The first two principal components (PC1 and PC2) were retained for the construction of the composite index.(Pan et al., 2025). The final QCI score for each observation was derived in two steps. First, a weighted composite score was calculated from PC1 and PC2, with weights proportional to the variance explained by each component. This composite score was then linearly rescaled to a range of 0 to 100, where a higher score indicates better quality of care. All statistical analyses and visualizations were performed using R software (version 4.3.1).
Results
3
The global burden of lip and oral cavity cancer in 2021 and trends since 1990
3.1
This study presents a comprehensive analysis of the burden of LOCC from 1990 to 2021, focusing on incidence and mortality across the SDI spectrum (Fig. 1 and Supplemental Table 1). The incidence of LOCC was highest in high-SDI regions, however, a critical divergence was observed in mortality patterns, as the highest number of deaths was concentrated in low-middle SDI regions, significantly surpassing those in high-SDI areas. This discrepancy underscores a stark disparity in healthcare outcomes, suggesting that while high-SDI regions detect more cases, low-middle SDI regions face greater challenges in delivering effective treatment, leading to poorer survival. From 1990 to 2021, the absolute number of both new cases and deaths from LOCC increased globally across most SDI levels and age groups. A marked rise in incident cases was documented; for instance, in the middle-high SDI region, cases in the 60–64 age group increased from 5943.89(95%UIs,5649.86265.4) to 10,807.5(95%UIs,9817.611765.8). Mortality exhibited a similarly concerning upward trend, particularly in low-middle SDI regions, where deaths in the 55–59 age group surged from 3494.9 to 8276.3(95%UIs,7146.69468), representing one of the most pronounced increases. In contrast, some high-SDI regions showed stable or even declining mortality in younger age groups. The age distribution of LOCC burden demonstrated a consistent pattern, with both incidence and mortality remaining low in younger ages (15–49 years), rising precipitously through middle age, and peaking between 60 and 70 years before declining in the oldest old (80+ years). This pattern aligns with the typical carcinogenesis process of LOCC, with the peak mortality burden occurring slightly earlier, in the 55-69 year cohort, within low-middle SDI regions.Fig. 1. Age-specific incidence (A) and mortality (B) of lip and oral cavity cancer among individuals aged 15 years and older, stratified by Socio-demographic Index region, 1990 and 2021.Fig. 1
QCI trends in various countries around the world
3.2
The QCI assessment revealed a global distribution across a spectrum of performance levels Fig. 2 and Supplemental Table 2). Countries with QCI scores of 90 or above, such as Australia, Spain, and the United States, represented the highest tier. This was followed by countries scoring between 80 and 89, including Switzerland, Norway, Japan, and South Korea. A tier of scores from 60 to 79 included nations like Italy, Singapore, and China (67.1 points,95%UIs:60**,70), while scores in the 40–59 range were observed in countries such as Russia and Brazil (47.2 points,95%UIs:40,50). Lower performance tiers included scores of 20–39 (e.g., India at 34.8 points,95%UIs:30,**40), 10–19 (e.g., Pakistan, Ethiopia), and below 10, with the lowest scores found in Haiti, Somalia, and the Central African Republic.Fig. 2. Global distribution of the Quality of Care Index for lip and oral cavity cancer among individuals aged 15 years and older, 2021.Fig. 2
Geographically, higher QCI scores were concentrated in Oceania, Western Europe, and North America, whereas lower scores were predominantly clustered in Sub-Saharan Africa and South Asia. The index demonstrated a positive association with national economic development levels. However, some countries, including Cuba (61.9 points,95%UIs:60**,70) and Costa Rica (62.4 points, 95%UIs:60,70), achieved scores notably higher than their economic peers. Regional disparities were evident within Asia, with Japan and South Korea attaining high scores, contrasting with the significant gap between Singapore (79.7 points,95%UIs:70,80) and Cambodia (32.76 points,95%UIs:30,**40). European countries consistently demonstrated strong performance, featuring prominently among the higher-scoring nations.
QCI situation of each age group
3.3
Globally, the QCI exhibited a consistent positive correlation with age, increasing from a mean of 1.8(95%UIs: 0**,10) in the 15–19 age group to 99.7(95%UIs:90,100) in the 95+ age group, with females generally showing marginally higher QCI values than males. Principal component analysis revealed that the PC1 accounted for 75.5% of the total variance (Fig. 3 and Supplemental Table 3). Analysis across SDI regions revealed distinct patterns. In Low and Low-Middle SDI regions, QCI demonstrated a monotonic increase with advancing age, rising from 0 to 7.5(95%UIs:0,10) to 98.1–100(95%UIs:90,100) and from approximately 5.3(95%UIs:0,10) to 98.8(95%UIs:90,100), respectively; females consistently had higher QCI values, and PC1 explained a substantial portion of the variance (63.8% and 72.1%, respectively) (Fig. 3b and c and Supplemental Table3). Conversely, in the Middle SDI region, QCI declined with age, from 98.4(95%UIs:90,100) in the youngest group to 0.7(95%UIs:0,10) in the oldest, with higher female QCI, while PC1 explained 68.3% of the variance (Fig. 3d and Supplemental Table 3). An inverted U-shaped trajectory was observed in High-Middle and High SDI regions, where QCI initially rose to a peak in middle age (e.g., 100(95%UIs:90,**100) in females aged 30–34 and 35–39, respectively) before sharply declining to near zero in the oldest groups; females maintained a QCI advantage, and the explanatory power of PC1 was 71.2% and 85.2%, respectively (Fig. 3e and f and Supplemental Table 3).Fig. 3. Age- and sex-specific trends in the Quality of Care Index for lip and oral cavity cancer and its correlation with component indices among individuals aged 15 years and older, stratified by Socio-demographic Index region, 2021.(Component indices: Years of Life Lost to Years Lived with Disability Ratio, Disability-Adjusted Life Years to Prevalence Ratio, Mortality-to-Incidence Ratio, Prevalence-to-Incidence Ratio).Fig. 3
Analysis of correlations among MIR, PIR, YLR, and DPR revealed that (Fig. 3): In the Low SDI region, MIR showed a strong positive correlation with DPR. In the Low-Middle SDI region, MIR also demonstrated strong positive correlations with YLR and DPR (approximately 0.8–0.9), while PIR was negatively correlated with these indicators. In the Middle SDI region, MIR and DPR increased with age and were negatively correlated with QCI, whereas PIR showed a positive correlation trend with QCI. In the High-Middle and High SDI regions, QCI exhibited strong negative correlations with MIR, YLR, and DPR, and a strong positive correlation with PIR.
QCI situation of each sex group
3.4
Between 1990 and 2021, the QCI showed universal improvement across all SDI regions for the combined data of both sexes. The high SDI region maintained the highest QCI, increasing from 88.5(95%UIs:80**,90) to 100(95%UIs:90,100), while the middle SDI region demonstrated the most significant growth, surging by 143% from 22.9(95%UIs:20,30) to 55.6(95%UIs:50,60) (Fig. 4a and Supplemental Table 4). Analysis by gender also revealed a consistent upward trend. Among males, QCI increased from 88.4(95%UIs:80,90) to 100(95%UIs:90,100) in the high SDI region, from 52.6(95%UIs:50,60) to 73.3(95%UIs:70,80) in the high-middle SDI region, from 21(95%UIs:20,30) to 54.4(95%UIs:50,60) in the middle SDI region, from 4.9(95%UIs:0,10) to 25.5(95%UIs:20,30) in the low-middle SDI region, and from 0.6(95%UIs:0,10) to 16.5(95%UIs:10,20) in the low SDI region (Fig. 4b and Supplemental Table 4). Similarly, among females, QCI rose from 88.9(95%UIs:80,90) to 100(95%UIs:90,100) in the high SDI region, from 53.9(95%UIs:50,60) to 83(95%UIs:80,90) in the high-middle SDI region, from 28.2(95%UIs:20,30) to 59.4(95%UIs:50,60) in the middle SDI region, from 5.3(95%UIs:0,10) to 28.4(95%UIs:20,30) in the low-middle SDI region, and from 0.27(95%UIs:0,10) to 18.5(95%UIs:10,**20) in the low SDI region (Fig. 4c and Supplemental Table 4). Throughout the study period, females consistently showed higher QCI values than males across all SDI regions, which aligns with our previous analysis.Fig. 4. Univariate analysis of Quality of Care Index scores for lip and oral cavity cancer among individuals aged 15 years and older, stratified by sex and Socio-demographic Index group, 2021.Fig. 4
Discussion
4
This study, based on global data on the burden and quality of care for oral cancer from 1990 to 2021, systematically reveals its multidimensional characteristics in terms of incidence, mortality, and the QCI. The main findings present a complex and uneven global picture. These persistent disparities highlight priorities that remain urgent today, such as strengthening early detection in low-resource settings. The findings thus provide directly actionable evidence for current efforts to achieve equitable cancer care.
Regarding disease burden, a notable “geographic decoupling of incidence and mortality” was observed: while high-SDI regions reported the highest incidence rates, low- and low-middle SDI regions bore the heaviest mortality burden(Meng et al., 2025). This contrast highlights structural inequities in early diagnosis and treatment accessibility for oral cancer globally. More comprehensive screening systems and diagnostic capabilities in high-SDI regions drive higher registered incidence, whereas low- and middle-low SDI regions suffer from high mortality due to scarce medical resources and delayed treatment, particularly evident among the core working-age population(Wu et al., 2025a, Wu et al., 2025b). This highlights the urgent need for targeted interventions in resource-limited settings. For example, strengthening community-based patient education to improve recognition of early oral symptoms such as persistent ulcers, lumps, or red or white patches could encourage earlier care seeking. Training primary healthcare workers in basic oral examination and referral protocols may also help bridge the diagnostic gap where specialist access is limited. (Liu and Han, 2025).
The global distribution of QCI further confirms the strong correlation between healthcare resources and economic development levels. High-scoring countries are concentrated in North America, Western Europe, and Oceania, while low-scoring countries cluster in Sub-Saharan Africa and South Asia. Countries like Cuba and Costa Rica achieved QCI scores significantly surpassing their SDI counterparts. This suggests that targeted health policies and strategic resource allocation can partially mitigate economic constraints(Benzian et al., 2022).Cuba's achievement may be attributed to its deeply embedded, community-oriented primary healthcare network, which could facilitate early detection and patient navigation(Dresang et al., 2005). Costa Rica's performance might reflect the success of its robust public health system and sustained tobacco control policies(Crosbie et al., 2016). These examples emphasize that beyond gross national income, governance, political commitment to health equity, and the design of service delivery models are pivotal determinants of cancer care quality. China's QCI score places it in the middle range, above most developing countries but still showing a noticeable gap compared to high-performing nations, reflecting room for improvement in its specialized oral cancer prevention and treatment system(Wu et al., 2025a, Wu et al., 2025b).
The relationship between QCI and age exhibited distinct patterns stratified by SDI levels. In low and low-middle SDI regions, QCI increased monotonically with age, suggesting that limited resources might be channeled more toward older patients with advanced disease, representing a passive, reactive approach rather than proactive prevention(Yang et al., 2025a, Yang et al., 2025b). In contrast, in high-middle and high SDI regions, QCI showed an inverted U-shaped relationship with age, with a sharp decline in the oldest groups (especially those over 80), hinting at potential age-based undertreatment or clinical bias, where even in resource-rich settings, older patients may face barriers to receiving aggressive therapy(Pan et al., 2025).
Females consistently demonstrated a QCI advantage across all SDI regions and age groups. This disparity may stem from behavioral patterns (higher exposure to tobacco and alcohol among males), health awareness (earlier help-seeking and better oral hygiene in females), and biological factors (protective effects of hormones or differential immune regulation)(Ghanem et al., 2024; Yang et al., 2023). Furthermore, QCI showed an upward trend across all regions from 1990 to 2021, with the most significant increase in middle-SDI regions, reflecting overall global improvement in oral cancer care quality and the gradual effectiveness of control measures(Ghamari et al., 2022).
The correlations between QCI and its component indicators (MIR, PIR, YLR, DPR) across SDI regions also offer policy insights. The strong positive correlation between MIR and DPR in low-SDI regions suggests a priority should be expanding access to essential healthcare services(Mohammadi et al., 2021). The positive correlation between QCI and PIR in high-SDI regions validates the successful model of improving survival through high-quality, standardized treatment(Yang et al., 2025a, Yang et al., 2025b). In low-middle SDI regions, the negative correlation between PIR and poor outcome indicators serves as a warning that merely expanding service coverage without enhancing treatment quality may fail to effectively reduce mortality rates(Lin et al., 2025). To address this, integrating palliative and supportive care services represents a critical dimension of quality enhancement that is often overlooked. Improving symptom control, pain management, and psychosocial support for advanced-stage patients through training for nurses and community health workers is not merely a compassionate add-on, but a fundamental component of effective care that can reduce suffering and potentially mitigate poor outcomes even when curative options are scarce(Huynh and Moore, 2021). This approach ensures that expanded service coverage is matched with substantive improvements in the patient experience and clinical management at all stages of disease.
This study has several limitations. First, incomplete disease registration systems in some low- and middle-low SDI countries may lead to underreporting and underestimation of the true burden. Second, reliance on GBD modeled estimates may introduce uncertainty. Third, the macro-level data cannot infer individual-level exposure-outcome relationships. Fourth, the retrospective design limits causal inference between care quality and health outcomes and may not fully capture recent advances in diagnosis and treatment.
Conclusion
5
From 1990 to 2021, the overall quality of care for lip and oral cavity cancer improved globally, yet significant inequities persist across regions, ages, and genders. Future strategies for LOCC control must move beyond merely tracking incidence and mortality and focus on systematically enhancing the performance of entire health systems. The QCI, as a comprehensive assessment tool, can provide crucial evidence for policymakers. We call for expanded access to primary care and standardized treatment in resource-limited settings, while in high-resource regions, attention should shift toward equitable diagnosis and management for elderly patients.
CRediT authorship contribution statement
Yilin Zhang: Writing – original draft, Visualization, Software, Methodology. Wenkai Xu: Writing – original draft, Validation, Software, Resources. Haocheng Wang: Visualization, Validation, Software. Liang Mao: Writing – review & editing, Methodology, Data curation. Jing Sun: Writing – review & editing, Project administration, Funding acquisition.
Ethical approval
Not Applicable.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1GBD 2021 Diseases and Injuries Collaborators Global incidence, prevalence, years lived with disability (YL Ds), disability-adjusted life-years (DAL Ys), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021 Lancet 4031044020242133216110.1016/S 0140-6736(24)00757-838642570 PMC 11122111 · doi ↗ · pubmed ↗
- 2GBD 2019 Healthcare Access and Quality Collaborators Assessing performance of the healthcare access and quality index, overall and by select age groups, for 204 countries and territories, 1990-2019: a systematic analysis from the global burden of disease study 2019 Lancet Glob. Health 10122022 e 1715 e 174310.1016/S 2214-109X(22)00429-636209761 PMC 9666426 · doi ↗ · pubmed ↗
- 3Alves-Costa S.Romandini M.Nascimento G.G.Lip and Oral Cancer, caries and other Oral conditions: estimates from the 2021 global burden of disease study and projections up to 2050 J. Periodontal Res.606202554455810.1111/jre.1342140530949 PMC 12312818 · doi ↗ · pubmed ↗
- 4Azadnajafabad S.Saeedi Moghaddam S.Keykhaei M.Expansion of the quality of care index on breast cancer and its risk factors using the global burden of disease study 2019 Cancer Med.12220231729174310.1002/cam 4.495135770711 PMC 9883412 · doi ↗ · pubmed ↗
- 5Benzian H.Watt R.Makino Y.Stauf N.Varenne B.WHO calls to end the global crisis of oral health Lancet 4001036720221909191010.1016/S 0140-6736(22)02322-436410360 · doi ↗ · pubmed ↗
- 6Bi Y.Huang K.Wang M.Jin Y.Zheng Z.J.Global, regional and national burden and quality of care index (QCI) of leukaemia and brain and central nervous system tumours in children and adolescents aged 0-19 years: a systematic analysis of the global burden of disease study 1990-2019 BMJ Open 1532025 e 09339710.1136/bmjopen-2024-093397 PMC 1193194240122536 · doi ↗ · pubmed ↗
- 7Chen S.Yang X.Huang L.Xie Y.Li Y.Lin Y.Increasing incidence, prevalence, and mortality of lip and oral cavity cancer in adults aged 70 and older globally: findings from GBD 2021 World J. Surg. Oncol.231202527610.1186/s 12957-025-03933-940652241 PMC 12255997 · doi ↗ · pubmed ↗
- 8Choi E.Lee S.Nhung B.C.Cancer mortality-to-incidence ratio as an indicator of cancer management outcomes in Organization for Economic Cooperation and Development countries Epidemiol. Health 39e 2017006201710.4178/epih.e 2017006 PMC 543422828171715 · doi ↗ · pubmed ↗