Spontaneous Rupture of the Renal Pelvis Secondary to Upper Tract Urothelial Carcinoma
Nikolay A Halachev, Stamen Andreev, Alexander Stoychev

TL;DR
A rare case of spontaneous renal pelvis rupture caused by upper tract urothelial carcinoma is presented, highlighting the diagnostic challenges and treatment approach.
Contribution
This paper reports a rare clinical case linking spontaneous renal pelvis rupture to upper tract urothelial carcinoma.
Findings
Spontaneous renal pelvis rupture was diagnosed as a result of upper tract urothelial carcinoma.
Radical nephroureterectomy with bladder cuff excision was effective in treating the condition.
No disease recurrence was observed following follow-up procedures.
Abstract
Spontaneous rupture of the renal pelvis is a rare case of urologic emergency. In almost all instances, it occurs as a result of obstruction of the urinary tract, leading to increased pelvic pressure, most often caused by a calculus. We present a case of a 71-year-old male with flank and abdominal pain. Rupture of the renal pelvis with urohematoma was suspected, but the etiology was unknown. Imaging, retrograde ureteropyelograhy, and flexible ureterorenoscopy couldn't find the underlying cause for the suspected renal pelvis rupture, and a subsequent explorative surgery was needed in order to establish a diagnosis. Treatment included radical nephroureterctomy with bladder cuff excision. Cystoscopy and PET/CT were performed as a follow-up. No evidence of disease recurrence was found.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
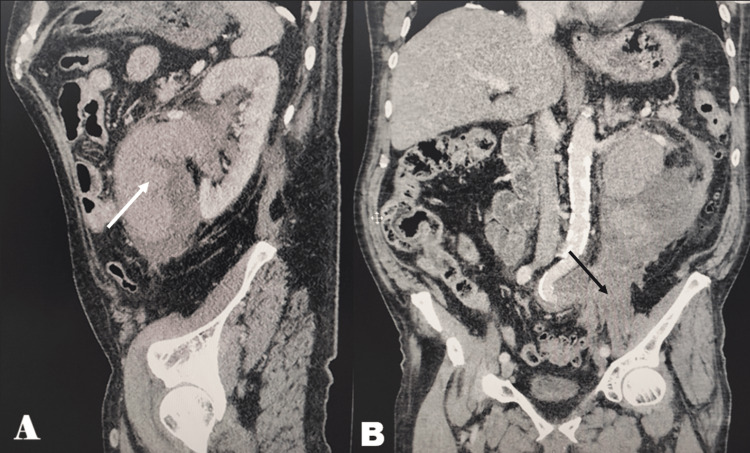 Figure 1
Figure 1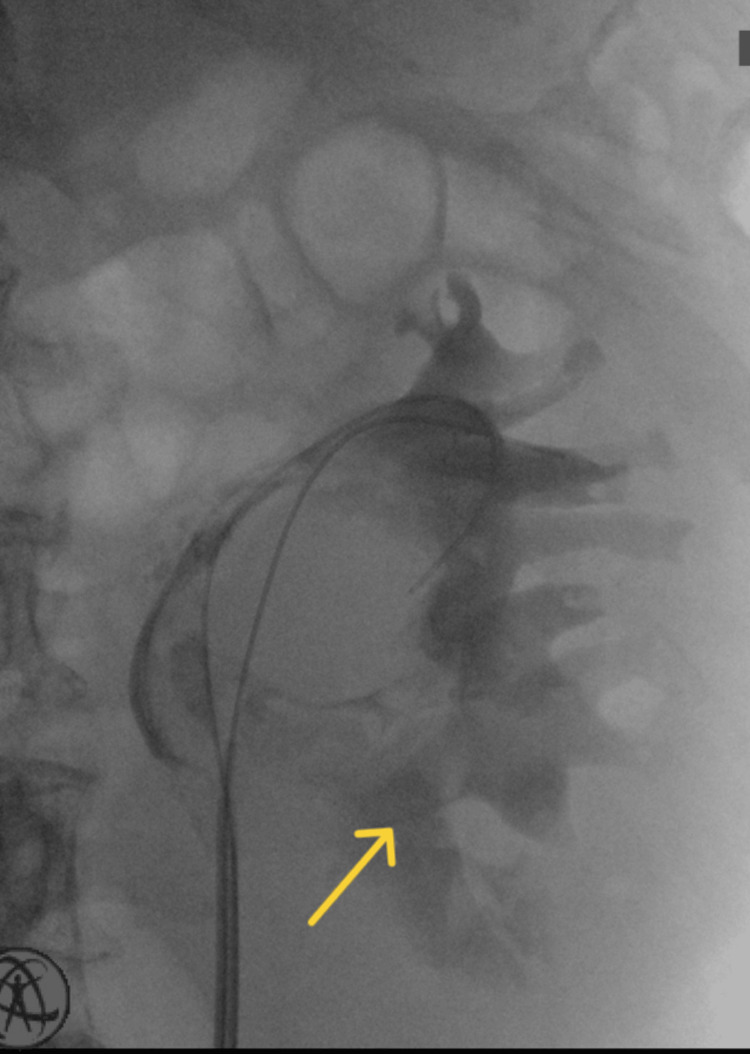 Figure 2
Figure 2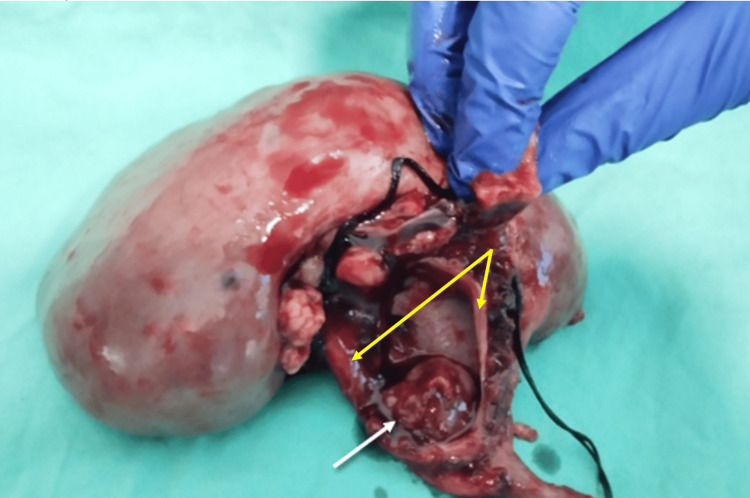 Figure 3
Figure 3| Blood test | Value | Normal range |
| Hemoglobin | 92 g/L | 135-180 g/L |
| Leukocytes | 12.5x10⁹ | 3.5-10.5x10⁹ |
| CRP | 327 mg/L | 0-5 mg/L |
| Iron | 4.1 μmol/L | 11.6-31.3 μmol/L |
| Iron binding capacity | 38.3 μmol/L | 50.4-90.7 μmol/L |
| Creatinine | 87 μmol/L | 63-111 μmol/L |
| BUN | 5.6 mmol/L | 2.8-8.3 mmol/L |
| Bacteria in urine* | 67 μmol/L | 0-33 μmol/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUreteral procedures and complications · Urological Disorders and Treatments · Abdominal Trauma and Injuries
Introduction
Spontaneous rupture of the renal pelvis is a rare case of urologic emergency, which is most often caused by an obstructing ureteric calculus leading to increased intrapelvic pressure [1]. Underlying causes can be divided into two groups - internal and external to the urogenital tract. The first one includes calculi, infections, iatrogenic, and tumors [1-6], and the second - trauma, malignancies, retroperitoneal fibrosis, lymph nodes, and aberrant vessels [7-12], causing an external compression leading to hydronephrosis and subsequent rupture. In the literature, however, idiopathic rupture has also been reported [13]. Our aim is to report a case of spontaneous pelvic rupture due to an obstructing urothelial carcinoma located in the pyeloureteral junction.
Case presentation
A 71-year-old male was admitted to the gastroenterology department due to elevated liver enzymes, poor general condition, and abdominal pain. The patient stated that the abdominal pain is located in the left upper and lower quadrants with maximum intensity in the left lumbar region. These symptoms occurred approximately 48 hours prior to admission. The patient denied any history of trauma or smoking and does not recall recent weight loss. Comorbidities include heart failure (New York Heart Association, NYHA class 2), hypertension, and mild aortic stenosis. Due to the pain in the lumbar region, a consultation with a urologist was made.
Physical examination revealed tenderness and exacerbation of pain on palpation in the said region. The patient was also febrile, with a temperature up to 38ᵒC. Some of the more important findings in the clinical laboratory are shown in Table 1.
Rupture of the kidney pelvis was suspected, and a CT scan with contrast medium was requested (Figure 1). It showed medial and caudal to the left kidney a massive non-homogeneous lesion suggestive of urohematoma measuring 10x6x15 cm. The said lesion did not enhance after administering contrast medium; only the kidney appeared to enhance its density. Due to the presence of the suspected urohematoma, any tumor formations couldn't be distinguished.
CT scan of the pelvisA: The white arrow shows hyperdense content mixed with fluid density.B: The lesion can be traced to the pelvis as pointed by the black arrow.
With these findings, highly suspicious of urinoma or perirenal hematoma, and the worsening overall condition of the patient, it was decided to proceed surgically. Retrograde ureteropyelography was conducted in order to find a cause. Extravasation of the contrast dye at the level of the kidney pelvis was seen (Figure 2). Filling defect, however, was not visualized due to the dilution of contrast medium in the already extravasated fluids. Subsequent retrograde flexible ureterorenoscopy couldn't establish an etiology for the pelvic rupture either because of the hematoma obstructing the view.
Retrograde ureteropyelographyTumor formation wasn't visualized; extravasation of the contrast medium was seen, as shown by the yellow arrow.
The patient underwent an open nephroureterectomy with bladder cuff excision. During the operation, the obstructing tumor located at the pelviureteric junction was clearly visualized. Proximal to the tumor on the medial upper wall of the renal pelvis, a rupture (Figure 3) was seen as well as a surrounding perirenal urohematoma, confirming the diagnosis. Pathologic evaluation revealed G2/LG (World Health Organization/International Society of Urological Pathology, WHO/ISUP) muscle-invasive papillary urothelial carcinoma of the pelvis without lymphovascular invasion; lymph nodes were negative for metastatic disease and negative surgical margins - pT2N0M0.
Post-nephrectomy kidney with the ruptured pelvisThe white arrow shows the obstructing tumor. The yellow arrows show the edges of the ruptured pelvic wall (site of rupture).
Serial follow-up three months post-surgery using cystoscopy and urine cytology, as well as a PET/CT at six months, showed no evidence of disease recurrence.
Discussion
Spontaneous renal pelvis rupture is a rare entity that is underreported in the literature [2]. In about 80% of the cases, the cause is obstruction due to impacted stones. There are a few cases worldwide regarding spontaneous rupture of the renal pelvis due to obstruction by a tumor. Patients typically present with back pain, dysuria, and microscopic hematuria, but sometimes they can be asymptomatic. If there is suspicion for such a diagnosis, an imaging modality like a CT scan is preferred [14].
Upper tract urothelial carcinoma (UTUC) is a relatively infrequent malignancy with an incidence of 5-10% of all urothelial tumors. It is more common in male patients between 70-90 years, with >50% of them being current smokers. UTUC arises from the urothelial lining of the renal pelvis and ureter and is characterized by distinct molecular, genetic, and environmental features compared to bladder urothelial carcinoma. Tumor growth narrows or occludes the urinary tract lumen, impeding urine outflow, and as the pressure exceeds the tensile strength of the renal pelvic wall, rupture occurs. Consequently, external compression from other types of tumors, such as rectal cancer and metastatic disease, can also cause such ruptures [7,8].
Hematuria is the most frequent symptom. In addition, there is about a 29% chance of recurrence in the bladder after treatment for UTUC, which means it is mandatory to perform cystoscopic evaluation at the time of diagnosis and as follow-up [15].
Diagnostic workup of UTUC includes CT urography, which has the highest diagnostic accuracy for detecting and staging [16]. The lesions appear to be mildly hyperdense in the unenhanced phase of the CT, in contrast to the more hyperdense blood clots or stones. Due to their poor blood supply, UTUCs have little accumulation of contrast in the arterial phase. In the excretory phase, they appear as filling defects [1]. MR urogram can also be useful in the diagnostic workup.
There is a lack of evidence on how to properly treat patients with upper urinary tract ruptures [17]. Most of the cases described in the literature suggest treatment modalities ranging from conservative ones with antibiotic administration up to surgical ones like placement of a ureteral stent or a nephrostomy tube [5,14,17]. Most authors favor non-surgical treatment. Morgan et al. propose that surgical approaches are suitable for patients with signs of infection, kidney failure, or other risk factors [17].
Tumor seeding following renal pelvis rupture caused by an obstructing tumor is a concerning possible complication - viable tumor cells may implant and proliferate outside the urinary tract, potentially leading to local recurrence, peritoneal carcinomatosis, or distant metastasis as seen with transitional cell carcinoma of the bladder after perforation [18]. Tumor seeding along the percutaneous access route for treatment of UTUC has also been reported in the literature [19,20].
Conclusions
Spontaneous rupture of the renal pelvis is a rare condition usually secondary to obstructing ureteric calculi. In a few cases, however, the underlying cause may be a urothelial tumor as seen in this case. Symptoms are not specific, ranging from mild flank pain and hematuria to an acute abdomen. It is suspected clinically and usually confirmed with appropriate imaging modalities. Early diagnosis is important in order to prevent further complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Spontaneous rupture of renal pelvis secondary to ureteral obstruction by urothelial tumor Rev Assoc Med Bras Fernandes DA Palma ALG Kido RYZ 415417602014
- 2Spontaneous rupture of the renal pelvis due to obstruction of pelviureteric junction by renal stone: a case report and review of the literature Urol Ann Yanaral F Ozkan A Cilesiz NC Nuhoglu B 293295920172879460210.4103/UA.UA_24_17PMC 5532903 · doi ↗ · pubmed ↗
- 3Pyonephrosis complicated with spontaneous intraperitoneal rupture and diffuse peritonitis: case report and literature review Clin Nephrol Nikolovski A Misimi S Draskacheva N Limani N 14715110120243817488010.5414/CN 111286 · doi ↗ · pubmed ↗
- 4Spontaneous rupture of the renal pelvis caused by upper urinary tract obstruction: a case report and review of the literature Medicine Zhang H Zhuang G Sun D Deng T Zhang J 096201710.1097/MD.0000000000009190 PMC 581574429390332 · doi ↗ · pubmed ↗
- 5Two cases of spontaneous rupture of upper urinary tract caused by the primary ureteral or renal pelvic tumor: a case report (in Japanese)Hinyokika Kiyo Inahara M Kojima S Takei K 3134552009 http://hdl.handle.net/2433/7276319227210 · pubmed ↗
- 6Renal pelvic rupture: a case report of an unexpected cause Int J Surg Case Rep Fouimtizi J Hosni A Jroundi L Slaoui A Koutani A Ibn Attya Andaloussi A 1061768520213438889310.1016/j.ijscr.2021.106176 PMC 8355923 · doi ↗ · pubmed ↗
- 7Urinoma formation secondary to ureteral obstruction by metastatic squamous cell carcinoma of the appendix. Case report Tumori Angulo JC Lopez JI Lopez-Arregui E Flores N 447449791993817174910.1177/030089169307900616 · doi ↗ · pubmed ↗
- 8Spontaneous rupture of the renal pelvis presenting as an urinoma in locally advanced rectal cancer World J Clin Cases Garg PK Mohanty D Rathi V Jain BK 108110220142474912310.12998/wjcc.v 2.i 4.108PMC 3985039 · doi ↗ · pubmed ↗