Association between cholecystectomy/gallbladder pathology and colorectal polyps: a systematic review and meta-analysis
Shirui Li, Yunfan Deng, Sheng Dai, Qi Fan, Dehai Xiong, Xiuyang Li

TL;DR
This study finds that gallbladder surgery and gallbladder issues are linked to a higher risk of colorectal polyps, suggesting the need for personalized screening.
Contribution
The study provides a meta-analysis showing cholecystectomy and gallbladder pathology are significant risk factors for colorectal polyps.
Findings
Cholecystectomy increases colorectal polyp risk by 39%, with East Asians showing nearly double the risk compared to North Americans.
Gallbladder polyps are more strongly associated with polyp risk than gallbladder stones.
Adjusting for smoking, alcohol, and BMI strengthens the observed risk estimates.
Abstract
Gallbladder-related pathologies may influence colorectal carcinogenesis, yet systematic evaluation of their associations with precursor lesions remains limited. This study addresses critical knowledge gaps by investigating the dual-axis relationship between cholecystectomy/gallbladder pathologies and colorectal polyp risk while elucidating geographical and biological effect modifiers. In accordance with the MOOSE/Cochrane guidelines, 27 observational studies were analysed through PROSPERO (CRD420251012876). Comprehensive meta-analysis was performed to assess the effects of cholecystectomy across polyp subtypes and gallbladder pathology (stones/polyps) associations. Heterogeneity was quantified via I² statistics, and pooled odds ratios (ORs) with 95% confidence intervals (CIs) were calculated via the DerSimonian–Laird random effects model to account for between-study variance. Subgroup…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
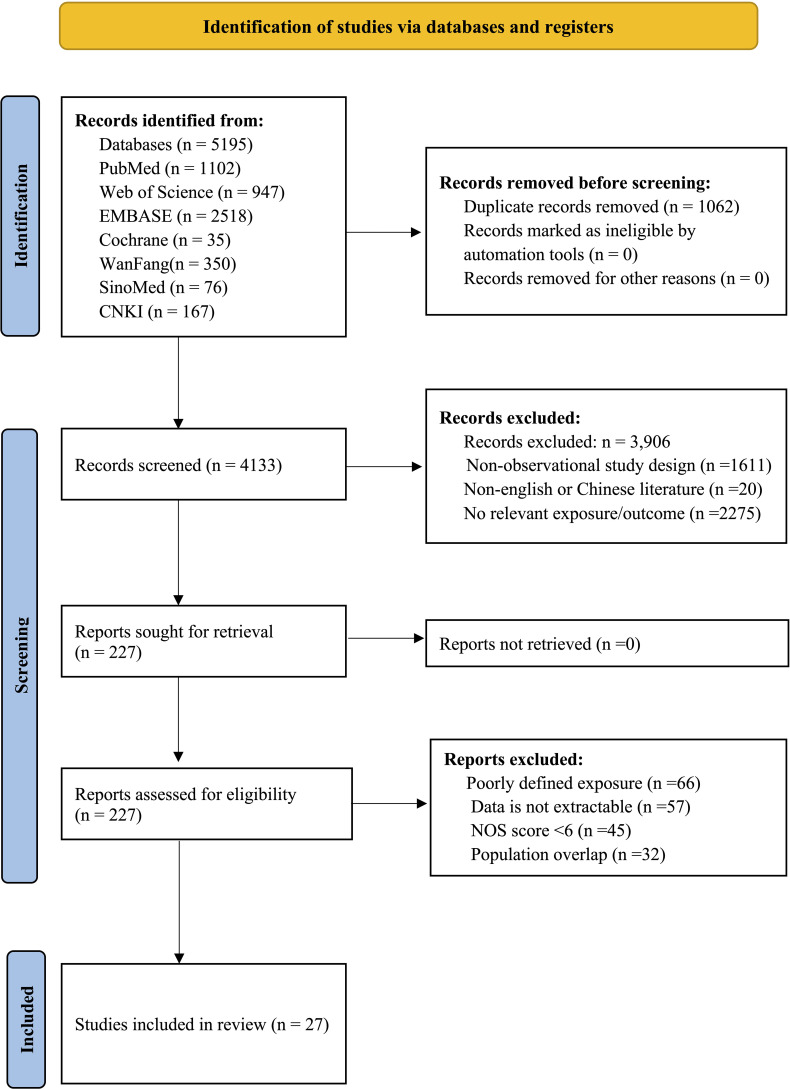 Figure 1
Figure 1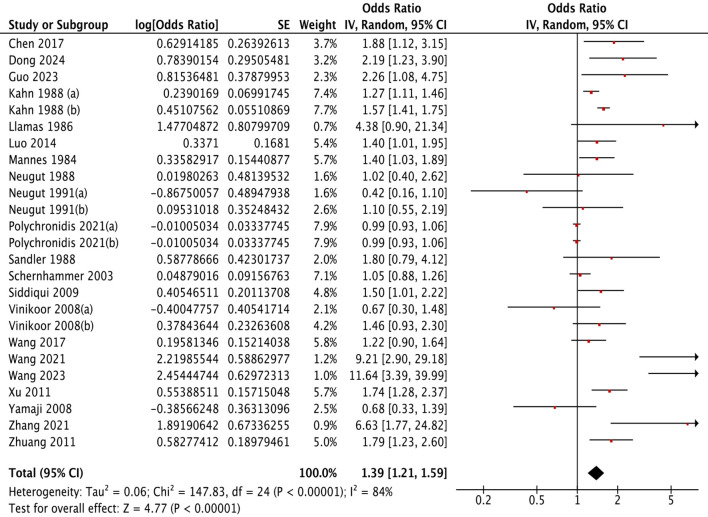 Figure 2
Figure 2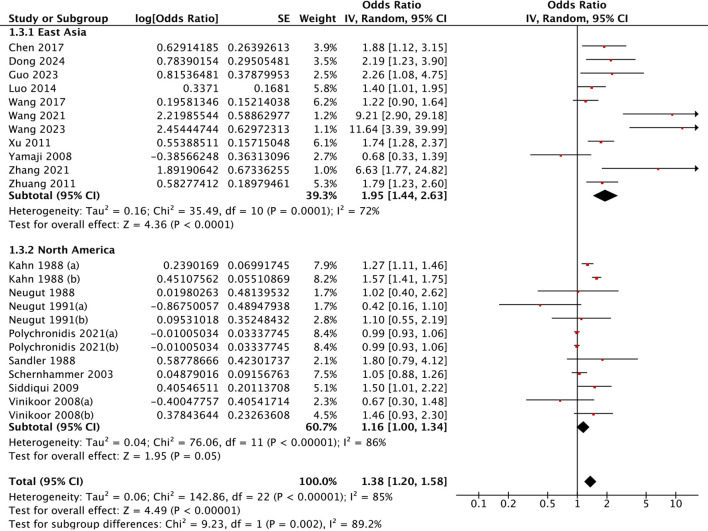 Figure 3
Figure 3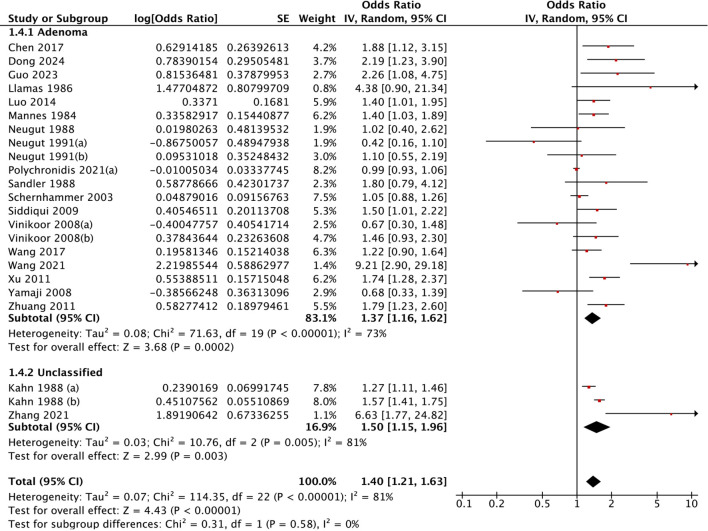 Figure 4
Figure 4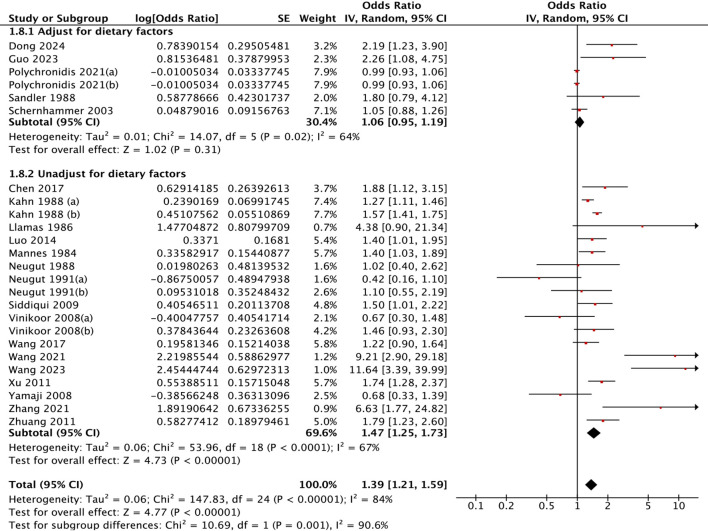 Figure 5
Figure 5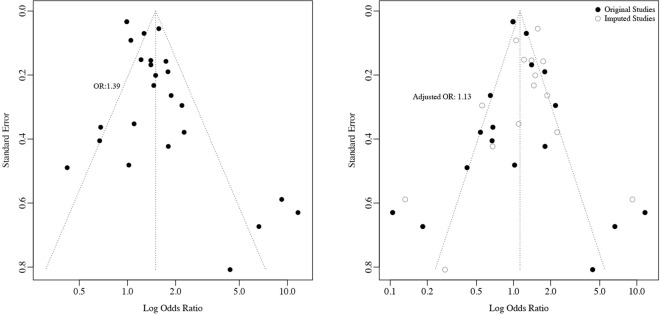 Figure 6
Figure 6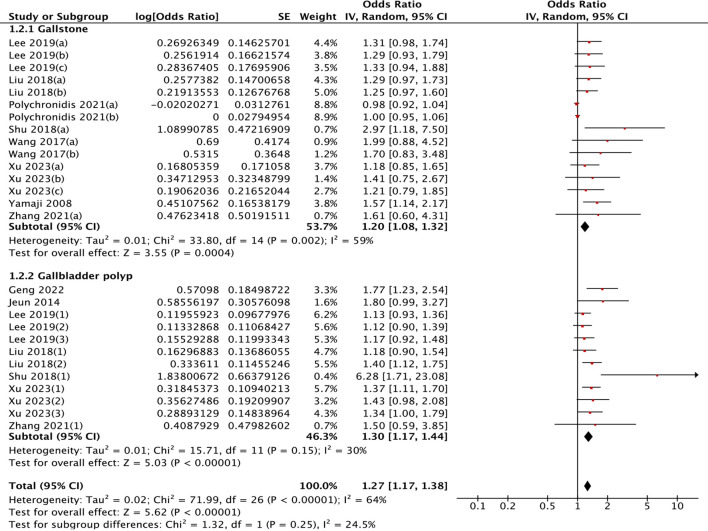 Figure 7
Figure 7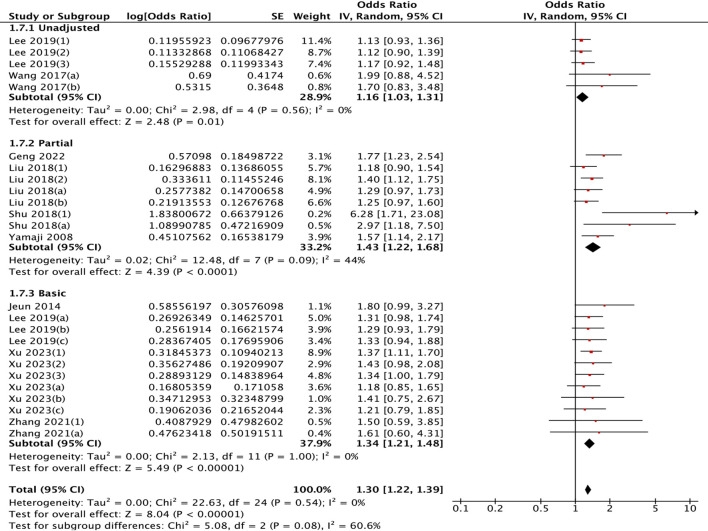 Figure 8
Figure 8| Study (Year) | Pathology type | Study design | Adjustment* | Region | Sample size | Recruitment period | NOS score | Citation |
|---|---|---|---|---|---|---|---|---|
| Yamaji 2008 | Adenoma | Cross-sectional | D+H | Japan | 5,719 | 1991-2003 | 9 | ( |
| Guo 2023 | Adenoma | Case-Control | H+N | China | 1,149 | 2016-2020 | 7 | ( |
| Zhang 2021 | Unclassified | Case-Control | H | China | 242 | 2018-2020 | 6 | ( |
| Chen 2017 | Adenoma | Cross-sectional | D+ | China | 1,125 | 2003-2012 | 7 | ( |
| Dong 2024 | Adenoma | Case-Control | H+N | China | 676 | 2016-2023 | 9 | ( |
| Wang 2021 | Adenoma | Case-Control | D+H | China | 743 | 2014-2018 | 8 | ( |
| Sandler 1988 | Adenoma | Case-Control | D+N | USA | 1,407 | 1983-1985 | 8 | ( |
| Schernhammer 2003 | Adenoma | Cohort | D+H+N | USA | 85,184 | 1982-1998 | 9 | ( |
| Neugut 1988 | Adenoma | Case-Control | D+ | USA | 400 | 1983-1985 | 6 | ( |
| Siddiqui 2009 | Adenoma | Case-Control | D+ | USA | 1,234 | 2000-2007 | 8 | ( |
| Vinikoor 2008 | Adenoma | Case-Control | D+H | USA | 1,437 | 1998-2002 | 8 | ( |
| Kahn 1988 | Unclassified | Cohort | D+H | USA | 154,224 | 1982-1992 | 8 | ( |
| Neugut 1991 | Adenoma | Case-Control | D+ | USA | 2,750 | 1986-1988 | 9 | ( |
| Wang 2023 | Serrated poly | Cohort | D+H | China | 761 | 2019-2022 | 9 | ( |
| Polychronidis 2021 | Adenoma/Serrated poly | Cohort | D+H+N | USA | 133721 | 1991-2012 | 7 | ( |
| Xu 2011 | Adenoma | Cohort | D+ | China | 11,863 | 2008-2011 | 7 | ( |
| Llamas 1986 | Adenoma | Case-Control | D+ | Australia | 144 | 1980-1982 | 6 | ( |
| Mannes 1984 | Adenoma | Cohort | Unreported | Germany | 761 | 1976-1982 | 9 | ( |
| Zhuang 2011 | Adenoma | Cohort | Unreported | China | 503 | 2009-2010 | 9 | ( |
| Wang 2017 | Adenoma | Cross-sectional | Unreported | China | 702 | 2013-2016 | 7 | ( |
| Luo 2014 | Adenoma | Cohort | Unreported | China | 981 | 2007-2013 | 7 | ( |
| Study | OR | 95% CI_lower | 95% CI_upper |
|---|---|---|---|
| Omitting Yamaji 2008 | 1.54 | 1.18 | 2.01 |
| Omitting Guo 2023 | 1.48 | 1.12 | 1.95 |
| Omitting Zhang 2021 | 1.44 | 1.12 | 1.85 |
| Omitting Chen 2017 | 1.49 | 1.13 | 1.97 |
| Omitting Dong 2024 | 1.48 | 1.12 | 1.95 |
| Omitting Wang 2021 | 1.41 | 1.12 | 1.78 |
| Omitting Sandler 1988 | 1.50 | 1.13 | 1.98 |
| Omitting Schernhammer 2003 | 1.53 | 1.16 | 2.02 |
| Omitting Neugut 1988 | 1.52 | 1.16 | 2.01 |
| Omitting Siddiqui 2009 | 1.51 | 1.14 | 1.99 |
| Omitting Vinikoor 2008 (a) | 1.54 | 1.18 | 2.01 |
| Omitting Vinikoor 2008 (b) | 1.51 | 1.14 | 2.00 |
| Omitting Kahn 1988 (a) | 1.52 | 1.15 | 2.01 |
| Omitting Kahn 1988 (b) | 1.50 | 1.13 | 1.99 |
| Omitting Neugut 1991 (a) | 1.54 | 1.20 | 1.98 |
| Omitting Neugut 1991 (b) | 1.52 | 1.15 | 2.01 |
| Omitting Wang 2023 | 1.41 | 1.13 | 1.76 |
| Omitting Polychronidis 2021 (a) | 1.54 | 1.17 | 2.03 |
| Omitting Polychronidis 2021 (b) | 1.54 | 1.17 | 2.03 |
| Omitting Xu 2011 | 1.49 | 1.13 | 1.98 |
| Omitting Llamas 1986 | 1.47 | 1.13 | 1.92 |
| Omitting Mannes 1984 | 1.51 | 1.14 | 2.00 |
| Omitting Zhuang 2011 | 1.49 | 1.13 | 1.97 |
| Omitting Wang 2017 | 1.52 | 1.15 | 2.01 |
| Omitting Luo 2014 | 1.51 | 1.14 | 2.00 |
| Pooled estimate | 1.50 | 1.15 | 1.95 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCholangiocarcinoma and Gallbladder Cancer Studies · Gallbladder and Bile Duct Disorders · Gastric Cancer Management and Outcomes
Introduction
1
Colorectal cancer (CRC), the third most prevalent malignancy worldwide, accounted for approximately 1.92 million new cases and 900,000 deaths in 2022, with Asia bearing the highest regional burden (1). Sporadic CRC predominantly arises from the adenoma–carcinoma sequence, wherein colorectal polyps (CRPs), particularly adenomatous polyps (APs) and serrated polyps (SPs), serve as critical precursor lesions (2–4). While conventional risk factors encompassing APC gene mutations, aging, and dietary patterns (particularly red meat consumption) remain well characterized (5, 6), emerging evidence implicates gallbladder-related pathologies as potential modulators of colorectal carcinogenesis. The proposed biological link primarily involves perturbations in bile acid enterohepatic circulation and gut microbial homeostasis, which may collectively promote a protumorigenic microenvironment in the colorectum (7).
Previous meta-analyses on CRC and gallbladder factors have yielded inconsistent results. For cholecystectomy (CC), some studies reported a modestly elevated CRC risk (RR = 1.22) (8) or site-specific increases (e.g., sigmoid colon, RR = 1.42) (9), whereas others found no significant association with precancerous adenomas (RR = 1.17, 95% CI: 0.93–1.48) (10), suggesting stage-specific effects. Similarly, gallstone disease suffers from endpoint bias; Polychronidis et al. reported moderately increased CRC risk (RR = 1.15) but did not analyze further polyp formation (11). This study design flaw is even more prominent for gallbladder polyps, as CRC development usually requires a long latency period, and it is difficult to capture the driving effect of gallbladder mucosal hyperplasia on early colorectal mucosal lesions using CRC as an endpoint. However, some screening cohorts have reported a 40% increased risk of colorectal adenoma in patients with gallbladder polyps (12), supporting a potential role in early carcinogenesis.
This controversy has highlighted several critical limitations in existing research. First, exposure classification is heterogeneous. For example, gallstones and gallbladder polyps are often grouped under the broad category of “gallbladder disease,” overlooking their distinct pathological mechanisms and, consequently, their potentially different roles in carcinogenesis. Specifically, gallstones primarily reflect a disorder of bile chemistry and gallbladder motility, whereas gallbladder polyps represent mucosal growths frequently driven by localized inflammation. This pathophysiological distinction suggests that they may influence colorectal mucosa through related yet distinct pathways (e.g., chronic bile acid exposure versus systemic inflammatory mediators), justifying their separate evaluation in our analysis (13). Similarly, cholecystectomy is frequently conflated with the underlying pathology, confounding risk estimation (14, 15). Second, the classification of endpoint events is overly broad. While most meta-analyses focus on CRC or colorectal neoplasms (CRNs), systematic investigations into CRPs, a precursor lesion, remain insufficient. This narrow focus limits the understanding of early-stage disease progression. Third, the reporting of key effect modifiers is notably inadequate. Insufficient original data on variables such as the time interval since cholecystectomy, gallstone size, or polyp anatomic location. This lack of granularity restricts the analysis of dose–response relationships and time-dependent risk, hindering the identification of potential causal pathways and effect modifiers.
To overcome these limitations, we propose a two-pronged approach to simultaneously examine the effects of cholecystectomy and gallbladder disorders on CRPs risk. This study specifically aims to: 1) examine the relationship between cholecystectomy and the risk of CRPs across histological subtypes (adenoma, hyperplasia, and serrated); and 2) investigate the relationship between gallbladder disorders and CRPs, independently assess the effects of gallstones and polyps on polyp formation, and differentiation of the independent effects of chronic gallbladder inflammation and anatomical loss. The aim is to avoid misjudgment of effects due to confusion of anatomical changes with the pathological status of the organ and provide clearer clinical guidance. Methodologically, we combined meta-analysis—to quantify effect sizes where data were sufficient—with systematic review for a qualitative synthesis of factors with limited studies. This framework provides a novel perspective on the gallbladder–gut axis and a scientific basis for risk-stratified clinical surveillance.
Methods
2
The Meta-analysis of Observational Studies in Epidemiology guidelines and Cochrane’s Handbook were followed in this study. The study protocol was prospectively registered (CRD420251012876) prior to data extraction, ensuring transparency and reducing selection bias.
Data sources and search strategy
2.1
A systematic search was conducted in the PubMed, Embase, Cochrane Library, Web of Science, and Chinese databases (CNKI, Wanfang, SinoMed) from inception to February 2025, with language restrictions to English and Chinese. We acknowledge that this may introduce language bias, but it was necessary due to practical constraints in translation and resources. The search strategy focused on two themes: (1) gallbladder diseases and surgical interventions (e.g., “gallstones,” “gallbladder polyps,” “cholecystectomy”) and (2) colorectal polyps (e.g., “adenomatous polyps,” “serrated lesions”). We combined MeSH terms (“Gallbladder Diseases,” “Gallstone,” “Colonic Polyps,” “Adenoma”) with free-text keywords via Boolean operators (AND/OR). We did not systematically search grey literature (e.g., conference abstracts, preprints) to ensure the inclusion of only peer-reviewed, full-text articles with complete methodologies and data necessary for rigorous quality assessment and meta-analysis. This approach enhances the reliability of our pooled estimates but may have missed some very recent or unpublished findings. The full search strategies are provided in Supplementary Material 1.
Study selection
2.2
Records were imported into EndNote Web v.20 for deduplication. Two independent reviewers (Li and Deng) screened titles/abstracts via Rayyan, a systematic review management platform, with full-text review for ambiguous cases. Discrepancies were resolved by a third reviewer (Lee). Eligible studies were observational in design (cohort, case–control, or cross-sectional) and investigated associations between specifically defined gallbladder disorders (gallstone, gallbladder polyps, or cholecystectomy) and incident colorectal polyps. Studies merely describing “gallbladder disease” without subtype specification were excluded. Exposures required objective validation: gallstones by imaging/surgical confirmation, gallbladder polyps through ultrasound/CT/MRI/endoscopic ultrasound, or cholecystectomy via surgical records. However, the variability in diagnostic accuracy across these modalities, particularly for polyp detection, represents a potential source of exposure misclassification and between-study heterogeneity. The outcomes included histologically confirmed non-malignant colorectal polyps (adenomas, hyperplastic polyps, serrated polyps, unclassified polyps). We excluded non-observational studies, non-English/Chinese publications, duplicate reports, and studies focused solely on invasive carcinomas. Articles lacking validated exposure measures, insufficient outcome data for effect size calculation, or ambiguous gallbladder disease classification were also excluded. More detailed inclusion and exclusion criteria are presented in Supplementary Material 2. The selection process followed PRISMA guidelines (Figure 1).
PRISMA flow diagram.
Data extraction
2.3
Two independent reviewers used a standardized spreadsheet to extract data: study identifiers, histopathological classification of colorectal polyps, gallbladder disease status, epidemiological study designs, and covariate adjustment. Geographical distribution was documented by continent and country of origin. The demographic parameters included the total sample size, age distribution metrics, and sex composition. The temporal characteristics included the recruitment timeframe, study duration, and publication chronology. For studies reporting multiple polyp subtypes, subtype-specific effect estimates were preserved in discrete data fields. The quantitative measures consisted of risk estimates with 95% CIs supplemented by logarithmic transformations for meta-analytic synthesis. For subgroup analysis, subgroups with fewer than three studies were excluded, and those missing values for a variable (such as the mean age or sex ratio) were excluded from the subgroup analysis and meta-regression.
Evaluating the quality of the studies
2.4
The quality of the included observational studies was assessed via the Newcastle–Ottawa Scale (NOS), a validated tool specifically designed for evaluating the methodological quality of nonrandomized studies, including cohort and case–control studies. Each study was awarded a maximum of 9 stars, with higher scores indicating higher methodological quality. The NOS evaluates studies across three domains:
Selection (4 stars): Assesses the representative of the exposed cohort, selection of the nonexposed cohort, ascertainment of exposure, and demonstration that the outcome of interest was not present at the start of the study.Comparability (2 stars): Evaluates the control for confounding factors, particularly whether the study is adjusted for age, sex, and other relevant variables.Outcome (3 stars): Assesses the method of outcome assessment, the adequacy of follow-up, and whether the follow-up was long enough for outcomes to occur.
The interviewer consistency kappa was 0.85, and disagreements were resolved through consultation.
Statistical analysis methods
2.5
Heterogeneity was evaluated via I² statistics and Cochran’s Q test (significance threshold: I²≥50% or Q test p < 0.10), guiding selection between random effects and fixed effects models. Primary meta-analyses were conducted in Review Manager 5.4 (Cochrane Collaboration) via the DerSimonian–Laird random effects model to account for between-study variance. The sensitivity analysis included leave-one-out analysis, a quality-based analysis in which studies with low NOS scores (<6) were excluded, and restricted maximum likelihood (REML) estimation and Hartung-Knapp adjustments were implemented in R 4.3.0 via the metafor package (v3.8-1). Publication bias was assessed via funnel plots, Egger’s regression test, and Begg’s test. The trim-and-fill method was used to estimate and adjust for potential publication bias. Univariable meta-regression was performed to explore associations between study-level covariates and the effect size. The proportion of variance explained (R²) was calculated for each covariate. A detailed classification of all subgroup analyses and statistical methods is provided in Supplementary Material 3. All the statistical tests were two-tailed (α = 0.05).
Result
3
Cholecystectomy and colorectal polyps
3.1
Study selection and characteristics
3.1.1
This meta-analysis synthesized evidence from 21 observational studies (25 effect estimates) involving 405,527 participants across three continents, with publication dates spanning 1984-2024. Geographically, 10 studies originated from China, 8 studies from North America, and 3 studies from other regions, including Japan and Australia. Methodologically, case–control designs predominated (n=10), followed by cohort studies (n=8) and cross-sectional investigations (n=3). Sample sizes demonstrated substantial heterogeneity, ranging from 144 participants in an Australian case–control study to 154,224 subjects in a U.S. cohort. Quality assessment via the Newcastle–Ottawa Scale revealed moderate methodological rigor (median score=7), with post-2010 studies showing improved quality scores (53.8% with NOS≥8 vs. 33% in earlier research). The complete study characteristics are tabulated in Table 1.
Cholecystectomy and colorectal polyp risk
3.1.2
Cholecystectomy was associated with a 39% greater risk of colorectal polyps (OR = 1.39, 95% CI: 1.21–1.59; I² = 84%, P < 0.001) (Figure 2). The 95% prediction interval, which estimates the range within which the true effect size would fall in 95% of future similar settings, was 0.84 to 2.29. This wide interval reflects the substantial heterogeneity observed across studies.
Association of gallbladder conditions with colorectal polyps.
Geographical disparities were evident. East Asian populations demonstrated significantly greater risks (OR = 1.95, 95% CI: 1.44-2.63) than North American cohorts did (OR = 1.16, 95% CI: 1.00-.34). This geographical disparity was statistically confirmed through heterogeneity testing (Chi²=9.23, P = 0.002) (Figure 3). In terms of polyp pathology, adenoma-specific studies demonstrated a pooled OR of 1.37 (95% CI: 1.16-1.62), whereas studies of unclassified types revealed significant associations (OR = 1.50, 95% CI: 1.15-1.96) (Figure 4). Furthermore, the strength of association varied with the adjustment for different confounders. Models adjusting for health factors (e.g., smoking, BMI) yielded an OR of 1.34 (95% CI: 1.12-1.61), while further adjustment for dietary factors attenuated the effect to non-significance (OR = 1.06, 95% CI: 0.95-1.19) (Figure 5). Analyses of other methodological factors, including study sample size, are presented in Supplementary Figure S1 and Supplementary Table S1.
Subgroup analysis by geographic region: association between cholecystectomy and colorectal polyp risk.
Subgroup analysis by polyp pathology: association between cholecystectomy and colorectal polyp risk.
Subgroup analysis by dietary adjustments: association between cholecystectomy and colorectal polyp risk.
Sensitivity analysis and publication bias
3.1.3
Leave-one-out iterations produced consistent effect estimates (OR range: 1.41-1.54; all P < 0.05), with no single study disproportionately influencing the pooled estimate (Table 2). Egger’s test suggested potential small-study effects (P = 0.005), whereas Begg’s test revealed no significant publication bias (P = 0.469). Trim-and-fill adjustment imputing 8 hypothetical studies yielded an attenuated but still significant effect size (OR = 1.13, 95% CI: 1.01-1.27), indicating that while the observed effect might be slightly overestimated, the positive association remains statistically robust (Figure 6). The cumulative meta-analysis demonstrated relative stabilization of effect estimates over time (OR = 1.50, 95% CI: 1.15-1.95), despite early fluctuations caused by imprecise estimates in pioneering studies (Supplementary Table S2).
Publication Bias assessment and trim-and-fill adjustment: (a) Funnel Plot (b) Trim and Fill adjusted effect Size Distribution.
Gallbladder pathology and colorectal polyp
3.2
Study selection and characteristics
3.2.1
Ten studies (pooled sample: 133,721 participants) investigated associations between gallbladder pathology (stones/polyps) and colorectal polyps. Geographical distribution revealed strong Asian representation, with one U.S. cohort broadening demographic diversity. Methodologies included cross-sectional, case–control and cohort designs, spanning diverse age groups (<50 years: 5 studies; ≥50 years: 5 studies), with sample sizes spanning two orders of magnitude (103-133,721 participants). Methodological quality and recruitment periods showed substantial variability (Supplementary Table S3).
Gallbladder pathology and colorectal polyp risk
3.2.2
The pooled analysis demonstrated a modest association between gallbladder pathology and colorectal polyps (OR = 1.27, 95% CI: 1.17–1.38; I² = 64%, P < 0.001). The 95% prediction interval for this association was 0.95 to 1.70.
Stratification by pathology type revealed differential risks: gallstones (OR = 1.20, 95% CI: 1.08–1.32) versus gallbladder polyps (OR = 1.30, 95% CI: 1.17–1.44) (Figure 7). Age-stratified analysis demonstrated stronger associations in older populations (≥50 years: OR = 1.41, 95% CI: 1.20-1.66) than in younger subgroups (OR = 1.20, 95% CI: 1.10-1.30), although this difference did not reach formal statistical significance (P = 0.07) (Supplementary Figure S2). A clear pattern emerged regarding confounding control: more comprehensive adjustment models yielded stronger associations. The risk estimate increased from OR = 1.16 (unadjusted) to OR = 1.34 (adjusted for age/sex), and was strongest (OR = 1.43, 95% CI: 1.22–1.68) in models that additionally accounted for smoking, alcohol, and BMI (Figure 8). Meta-regression identified that higher study quality (NOS score) was a significant inverse predictor of the risk estimate (β = -0.19 per point, P < 0.001), suggesting that methodological rigor may attenuate the observed effect. Full meta-regression results are available in Supplementary Table S4. Analyses of other methodological factors, including study type, are presented in Supplementary Figure S2.
Differential impact of gallbladder pathology subtypes on colorectal polyp risk.
Subgroup analysis of association between cholecystectomy and colorectal polyp risk. (a) by gender; (b) by sample size; (c) by adjustment for basic factors (sex/age); (d) by adjustment for healthy factors (alcohol/ smoking/ BMI).
Sensitivity analysis and publication bias
3.2.3
Leave-one-out sensitivity analysis confirmed robustness (OR = 1.24-1.28; all P < 0.001). However, trim-and-fill adjustment imputing 14 studies attenuated the effects to no significance (OR = 1.09, 95% CI: 0.96–1.23), revealing potential publication bias and suggesting that the observed association for gallbladder pathology requires more cautious interpretation and further validation (Supplementary Table S5).
Certainty of the evidence
3.3
The certainty of the evidence was assessed via the GRADE (Grading of Recommendations, Assessment, Development, and Evaluations) framework. The certainty was further graded on the basis of the risk of bias (assessed via the Newcastle–Ottawa Scale), inconsistency (evaluated via I² statistics), indirectness, imprecision (wide confidence intervals), and publication bias (assessed via funnel plots, Egger’s test, and Begg’s test). The final certainty of the evidence for each outcome is presented in the summary table (Supplementary Table S6).
Discussion
4
Main findings and risk gradient
4.1
Our study revealed a significant association between cholecystectomy and colorectal polyp risk (OR = 1.39, 95% CI: 1.21-1.59), with a greater effect magnitude than that reported in previous meta-analyses on CRC outcomes. Notably, although earlier meta-analyses failed to identify significant CC-CRPs associations (RR = 1.17, 95% CI: 0.93-1.48), our findings revealed greater effect sizes for cholecystectomy on adenomas (OR = 1.37, 95% CI: 1.16-1.62) than for unclassified polyps, suggesting stage-specific gallbladder involvement in the adenoma–carcinoma sequence. However, given that the annual malignant transformation rate of adenomas ranges from merely 0.25%-6%, with variation by age, sex, and surveillance duration (36), cautious interpretation remains warranted regarding the CRC implications of gallbladder–polyp associations. Through our two-pronged analysis and subgroup stratification, we identified a risk gradient (CC OR = 1.39 > gallbladder polyp OR = 1.30 > gallstone OR = 1.20), indicating that anatomical irreversibility and distinct inflammatory patterns of gallbladder pathology potentially constitute key drivers of risk stratification.
Biological plausibility and proposed mechanisms
4.2
Post-cholecystectomy bile acid enterohepatic cycling acceleration significantly elevates secondary bile acid proportions (e.g., DCA and LCA) through continuous biliary flow into the intestine (37). These hydrophobic bile acids directly damage enterocyte membranes while inducing reactive ROS/RNS generation, triggering oxidative–nitrosative stress that induces DNA damage and promotes proliferative signaling via the Wnt/β-catenin pathway, thereby driving adenoma formation (38–40). This is compounded by concomitant gut microbiota dysbiosis, characterized by a reduction in beneficial, short-chain fatty acid-producing bacteria and an expansion of pathobionts, which impairs intestinal barrier integrity, LPS translocation and amplifies systemic low-grade inflammation, insulin resistance, and lipid metabolism disorders (41–43). A vicious cycle emerges through bile acid–microbiota crosstalk: increased bacterial BSH activity accelerates primary bile acid deconjugation, further increasing DCA production, enriching pathobionts to exacerbate the imbalance in the mucosal microenvironment (44, 45).
In contrast, gallstone impaction induces sphincter of Oddi dysfunction with abnormal bile excretion patterns (38). Clinical studies have revealed exaggerated postprandial bile acid concentration fluctuations in gallstone patients, exacerbating DNA damage through mitochondrial apoptosis pathways (46). Gallbladder polyps, often arising in a background of chronic cholecystitis, are linked to the hypersecretion of pro-inflammatory cytokines such as IL-6, which can promote remote neoplastic progression via angiogenic and invasive pathways (47, 48).
This mechanistic heterogeneity explains the observed risk gradient: cholecystectomy exerts prolonged effects through dual-pathway synergy (bile acid dysmetabolism and microbiota disruption), whereas polyps primarily mediate remote effects via inflammatory cytokines. Although both pathologies involve bile acid composition alterations, their spatiotemporal inflammatory patterns (pulsatile vs. sustained) may partially account for risk stratification.
Clinical and demographic effect modifiers
4.3
The substantial statistical heterogeneity (I² = 84%) and wide 95% prediction intervals indicate that the cholecystectomy–polyp association is not uniform but is modified by other factors. Our subgroup analyses and meta-regression identify key sources of this heterogeneity from clinical/demographic effect modifiers, methodological diversity across studies, and varying degrees of confounding control. Clinical and demographic modifiers constituted a major source of heterogeneity. The most striking disparity was geographical, with East Asian populations exhibiting nearly double the risk of North Americans (OR = 1.95 vs. 1.16). This disparity may stem from gene-environment interactions, particularly differences in dietary patterns (e.g., high refined carbohydrate intake) (49). The elevated risk in East Asian populations implies that refined carbohydrate intake may exert stronger driving effects on the microbiota–DCA axis than the protective role of dietary fiber does, whereas the heterogeneous risk profile in North Americans with prevalent low-fiber consumption might be modulated by subgroup dietary variations (e.g., high-fiber consumers). Furthermore, demographic factors played a role. The stronger association in older individuals (≥50 years: OR = 1.41) may reflect an age-related decline in mucosal resilience. The elevated risk observed in women, particularly within the first post-operative decade (OR = 2.02; Vinikoor et al.), suggesting a potential modulatory role of sex hormones, possibly through interactions with bile acid signaling pathways, and indicating a time-sensitive window of susceptibility (50). Anatomical site was another modifier, with the left colon showing greater susceptibility (OR = 1.82 vs. right colon OR = 1.11; Yamaji et al.), potentially due to the enhanced toxicity of bile acids in its more acidic environment (51). Paradoxical associations between lesion size and risk (e.g., strong correlation with small but not large adenomas) may reflect stage-specific mechanistic influences in early carcinogenesis (52).
Methodological diversity constituted another major source of heterogeneity. The pooling of diverse study designs (e.g., cohort vs. case-control)—which inherently differ in their susceptibility to recall and selection bias—introduced fundamental variation. Furthermore, the operational diagnostic criteria of both exposure and outcome were inconsistent across studies. For exposure, the diagnostic methods for gallbladder conditions varied widely, from self-report to different imaging modalities (ultrasound, CT, MRI, endoscopic ultrasound) with varying accuracy, especially for polyp detection. This heterogeneity in exposure ascertainment likely contributed to measurement error and between-study variability. Crucially, the extent of confounding control was highly variable; while most studies adjusted for age and sex, fewer accounted for dietary patterns, which our subgroup analysis revealed to be a critical modifier. This spectrum of methodological rigor likely contributed to the disparate risk estimates.
Clinical implications and future directions
4.4
Our findings advocate for the integration of gallbladder history into personalized CRC risk assessment. The consistent risk gradient suggests that patients with a history of cholecystectomy, particularly those of East Asian descent, females in the early post-operative years, or individuals over 50, could be candidates for earlier initiation of colonoscopy or shortened surveillance intervals. The presence of gallbladder polyps may also warrant heightened clinical vigilance. Future research should prioritize longitudinal studies with serial biospecimen collection to delineate the temporal dynamics of risk and elucidate the precise roles of specific bile acids and microbial taxa. Mechanistic studies using organoid models are needed to confirm the carcinogenicity of post-cholecystectomy bile. Finally, cost-effectiveness analyses are required to translate these epidemiological findings into formal, updated screening guidelines.
Limitations
4.5
Our conclusions must be interpreted within the context of several limitations. First, the inherent nature of observational data precludes causal inference. Despite adjustments for key confounders, residual confounding by unmeasured or imperfectly measured factors (e.g., detailed dietary components, physical activity) remains possible. Crucially, reverse causality cannot be ruled out; underlying metabolic conditions such as insulin resistance or a pro-inflammatory state may predispose individuals to both gallbladder diseases necessitating surgery and the development of colorectal polyps. Second, the geographic concentration of studies, particularly on gallbladder pathology in East Asia, limits the generalizability of our findings to other ethnic and populations with different genetic backgrounds and lifestyle patterns. Third, and importantly, the lack of individual-level data on the time since cholecystectomy prevented a dose-response analysis of duration effects, leaving a key clinical question about the temporal dynamics of risk unresolved. Finally, while our comprehensive search strategy focused on major databases, restricting to English and Chinese publications may have introduced language bias.
Conclusion
5
This systematic review and meta-analysis of 27 observational studies found evidence of an association between cholecystectomy and an increased risk of colorectal polyps (OR = 1.39, 95% CI: 1.21–1.59), with adenomas showing stronger associations than unclassified polyps. Gallbladder pathologies—particularly polyps (OR = 1.30) and stones (OR = 1.20)—are also associated with elevated risks, though these estimates are lower than that for cholecystectomy. Key findings include the following:
Geographical disparities: East Asian populations presented nearly double the risk of North Americans (OR = 1.95 vs. 1.16), potentially linked to unmeasured dietary or genetic modifiers.Methodological influences: Medium-sized studies and those adjusting for smoking/alcohol/BMI yielded higher estimates, whereas dietary adjustment attenuated the effects.Age stratification: Stronger associations in individuals ≥50 years (OR = 1.41) suggest age-related mucosal vulnerability.
The observed risk gradient (cholecystectomy > polyps > stones) may reflect a corresponding gradient in the degree or persistence of biliary and systemic disturbances, although the exact nature of these disturbances requires clarification. However, residual heterogeneity (I²=84% for cholecystectomy), potential publication bias (trim-and-fill adjusted OR = 1.13) and most importantly, the observational nature of all included studies underscores the need for cautious interpretation. Residual confounding (e.g., by diet or metabolic factors) or reverse causality remain plausible alternative explanations. In summary, this study identifies gallbladder status, and particularly a history of cholecystectomy, as a factor associated with a higher prevalence of colorectal polyps. These findings suggest that gallbladder history could be considered in personalized CRC risk assessment, which might help to identify individuals for whom earlier or more intensive colonoscopic surveillance could be evaluated. Future studies should prioritize standardized exposure classification and longitudinal designs to better understand the nature of this association and clarify any underlying causal pathways.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F Laversanne M Sung H Ferlay J Siegel RL Soerjomataram I . Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024) 74:229–63. doi: 10.3322/caac.21834, PMID: 38572751 · doi ↗ · pubmed ↗
- 2Vogelstein B Fearon ER Hamilton SR Kern SE Preisinger AC Leppert M . Genetic alterations during colorectal-tumor development. N Engl J Med. (1988) 319:525–32. doi: 10.1056/nejm 198809013190901, PMID: 2841597 · doi ↗ · pubmed ↗
- 3Snover DC . Update on the serrated pathway to colorectal carcinoma. Hum Pathol. (2011) 42:1–10. doi: 10.1016/j.humpath.2010.06.002, PMID: 20869746 · doi ↗ · pubmed ↗
- 4Rex DK Ahnen DJ Baron JA Batts KP Burke CA Burt RW . Serrated lesions of the colorectum: review and recommendations from an expert panel. Am J Gastroenterol. (2012) 107:1315–29; quiz 4, 30. doi: 10.1038/ajg.2012.161, PMID: 22710576 PMC 3629844 · doi ↗ · pubmed ↗
- 5Clinton SK Giovannucci EL Hursting SD . The world cancer research fund/American institute for cancer research third expert report on diet, nutrition, physical activity, and cancer: impact and future directions. J Nutr. (2020) 150:663–71. doi: 10.1093/jn/nxz 268, PMID: 31758189 PMC 7317613 · doi ↗ · pubmed ↗
- 6Valle L Vilar E Tavtigian SV Stoffel EM . Genetic predisposition to colorectal cancer: syndromes, genes, classification of genetic variants and implications for precision medicine. J Pathol. (2019) 247:574–88. doi: 10.1002/path.5229, PMID: 30584801 PMC 6747691 · doi ↗ · pubmed ↗
- 7Feng Q Liang S Jia H Stadlmayr A Tang L Lan Z . Gut microbiome development along the colorectal adenoma–carcinoma sequence. Nat Commun. (2015) 6:6528. doi: 10.1038/ncomms 7528, PMID: 25758642 · doi ↗ · pubmed ↗
- 8Zhang Y Liu H Li L Ai M Gong Z He Y . Cholecystectomy can increase the risk of colorectal cancer: A meta-analysis of 10 cohort studies. P Lo S One. (2017) 12:e 0181852. doi: 10.1371/journal.pone.0181852, PMID: 28771518 PMC 5542607 · doi ↗ · pubmed ↗