Prosthetic Joint Infections in Trapeziometacarpal Arthroplasty: A Comprehensive Systematic Review
Guido Bocchino, Silvia Pietramala, Stella La Rocca, Giulia Di Pietro, Alessandro El Motassime, Giacomo Capece, Domenico De Mauro, Camillo Fulchignoni, Giulio Maccauro, Raffaele Vitiello

TL;DR
This paper reviews prosthetic joint infections in TMC arthroplasty, finding them rare but challenging to manage due to inconsistent reporting and treatment.
Contribution
The study provides a systematic review of infection rates and management in TMC joint prostheses, highlighting the need for standardized protocols.
Findings
Only 0.36% of 4165 TMC joint procedures had infections, with Staphylococcus aureus in two cases.
Infection management included antibiotics, debridement, and prosthesis removal with or without reimplantation.
Inconsistent diagnostic criteria and treatment approaches limit uniform conclusions.
Abstract
Background: Osteoarthritisof the first trapeziometacarpal (TMC) joint (rhizarthrosis) is a degenerative condition causing pain, reduced mobility, and functional limitations, particularly in older adults and postmenopausal women. Though conservative treatments offer symptomatic relief, advanced cases often require trapeziectomy or total joint replacement. The choice of prosthesis is tailored to patient-specific factors such as age, functional demands, and comorbidities. Despite the benefits of TMC joint replacements, prosthetic infections remain underexplored. Materials and Methods: This systematic review (covering 2000–2024) adhered to PRISMA guidelines, searching Medline, Cochrane, and Google Scholar for randomized controlled trials and case series. Data on demographics, prosthesis types, infection rates, and management strategies were extracted and analyzed. Results: Among 4165 TMC…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2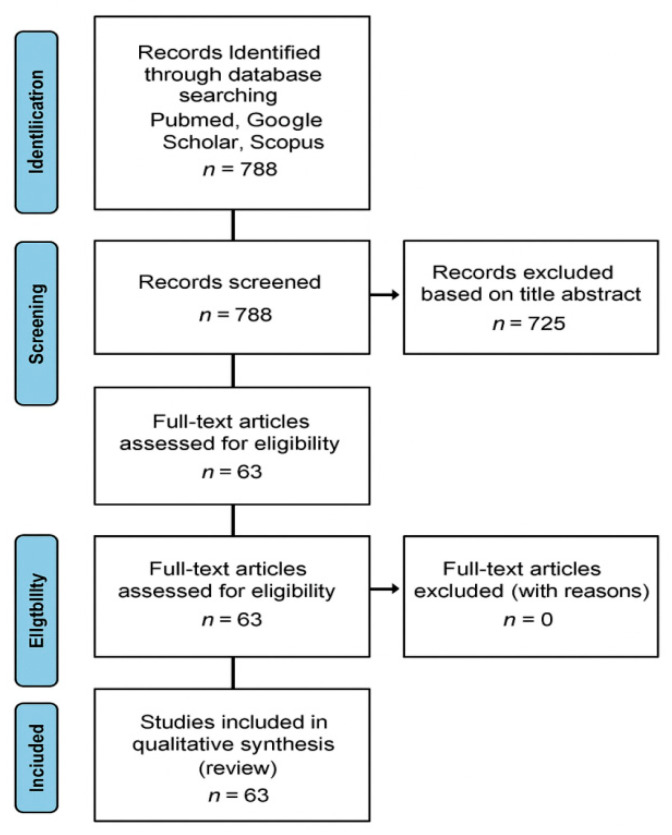 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Surgery and Rehabilitation · Foot and Ankle Surgery · Osteoarthritis Treatment and Mechanisms
1. Introduction
Osteoarthritis of the first trapeziometacarpal (TMC) joint, or rhizarthrosis, is a common condition, with an age-adjusted prevalence of 7% in men and 15% in women [1] (Figure 1). This condition can lead to pain, deformity, reduced range of motion, joint instability, and weakness, resulting in substantial functional limitations, particularly in postmenopausal women and older individuals [2]. The primary goals of treatment are to reduce pain, improve thumb mobility, enhance joint stability, and restore hand functionality [3]. Given the heterogeneity of patient characteristics, disease severity, functional demands, and comorbidities, the management of TMC osteoarthritis increasingly requires a personalized and precision medicine approach tailored to individual patient profiles.
Non-surgical management options include activity modification, oral analgesics, splinting, physical therapy, and corticosteroid injections [4]. Surgical intervention becomes necessary when conservative measures fail to adequately control symptoms. Surgical options include extension osteotomy, TMC arthroscopy with debridement, partial or complete trapeziectomy (alone or combined with ligament reconstruction and tendon interposition (LRTI) or suspensionplasty), arthrodesis, or joint replacement [2].
Trapeziectomy has been a standard surgical treatment for TMC osteoarthritis for over 70 years and is generally effective in relieving pain and restoring thumb mobility [4]. However, thumb shortening remains a concern, as it may impair pinch strength and result in impingement between the metacarpal base and the scaphoid. The addition of ligament reconstruction and tendon interposition was developed to address these challenges. Moreover, post-operative care requires a rigid cast for 3 to 4 weeks with an overall functional recovery time of 3 months. These limitations have highlighted the importance of selecting surgical strategies based on patient-specific functional needs, expectations, and risk factors, in line with principles of precision surgery.
On the other hand, most recent solutions, such as TMC arthroplasties, aim to restore thumb length while maintaining functional mobility, stability, and grip strength [5] (Figure 2). The initial generation of implants primarily utilized silicone spacers [6]. Subsequently, a total joint replacement that converted the TMC saddle joint into a ball-and-socket joint was introduced by integrating a cup in the trapezium and a cemented stem in the first metacarpal [7]. In recent years, attention has shifted towards cementless ball-and-socket implants with metal-on-polyethylene articulations, which aim to improve functionality and longevity while addressing the limitations of earlier designs. These technological advancements have expanded the range of implant options, enabling surgeons to better match implant characteristics to individual anatomical and functional requirements.
Modern cementless TMC implants use metal-on-polyethylene articulations with grid-blasted titanium or hydroxyapatite-coated cobalt-chrome components. These implants are available with various cup designs (e.g., hemispheric, conical, or screw) and stem configurations, as well as options for dual-mobility articulations.
Historically, total TMC joint replacements were considered inferior to trapeziectomy due to high revision rates and limited long-term implant durability. However, more recent non-randomized studies with follow-ups exceeding 12 months have demonstrated superior pinch and grip strength and faster recovery with joint replacements compared to trapeziectomy [8,9]. These findings have contributed to an increased preference for TMC joint replacements, challenging earlier perceptions of their limited benefits. Nonetheless, complications such as prosthetic joint infection, dislocation, loosening, and wear remain potential concerns [5]. Among these, prosthetic joint infection represents a particularly critical complication, as its risk and management may vary significantly according to patient-specific factors, surgical technique, and implant characteristics.
Research on complications related to TMC joint replacement surgery is sparse, with most studies focusing on single-surgeon experiences, older implant designs, and small patient cohorts. The primary aim of this review is to systematically summarize the available evidence on prosthetic infections following thumb CMC joint replacement, including their incidence, clinical presentation, treatment strategies, and outcomes. By synthesizing the existing evidence, this review seeks to support a personalized and precision medicine approach to risk stratification, prevention, and management of prosthetic joint infections in TMC arthroplasty. A secondary objective is to identify gaps in the current literature and provide evidence-based recommendations to guide clinical decision-making and future research in this underexplored area.
2. Materials and Methods
The review adhered to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [10], ensuring a comprehensive and systematic approach to data retrieval and synthesis. The methodological approach was designed to capture patient-specific, surgical, and implant-related variables potentially relevant to personalized and precision medicine strategies in the prevention and management of prosthetic joint infections.
2.1. Search Strategy
The analysis was conducted using the keywords ‘trapeziometacarpal’, ‘rhizarthrosis’, ‘thumb arthritis’, ‘CMC’, ‘TM’, ‘TMC’, ‘thumb’ AND ‘prosthesis’, ‘Touch’, ‘replacement’, ‘Maia’, ‘Isis’. Databases searched included Medline (PubMED), Cochrane and Google Scholar up to 30 September 2024. Articles published in English, Spanish, French, Portuguese and Italian in peer-reviewed journals were considered. Excluded were biomechanical reports, animal studies, cadaver studies, in vitro research, case reports, case series with fewer than 10 cases, literature reviews, technical notes, letters to editors and instructional materials. Four authors (G.B, G.C, G.D.P, C.F.) independently reviewed abstracts and full texts were obtained if abstracts were inconclusive. All differences between the reviewers were discussed and if disagreement remained the senior author (R.V.) was consulted. Reference lists of selected articles were manually checked. All the selected studies were retrospectively analyzed by an author (G.B.) who then extracted and entered the data in an Excel worksheet. Lastly, the data sheet was reviewed by two authors (G.C, D.D.M.) who agreed on the extracted data.
The literature references of identified papers were also searched to find further relevant articles. All journals were considered.
2.2. Inclusion and Exclusion Criteria
The eligibility criteria for inclusion in this review were established to ensure the selection of high-quality studies. Included studies were randomized controlled trials (RCTs), clinical trials. Case reports and case series with fewer than 10 patients were also included if they reported prosthetic joint infections (PJI), due to the rarity and clinical relevance of these events. Excluded were systematic reviews, meta-analyses, in vitro studies, animal studies, cadaver studies, reports on other inflammatory conditions (e.g., tendinitis), and studies published in languages other than English, Spanish, French, Portuguese, or Italian. Studies reporting confirmed or suspected PJI were included. PJI was defined according to each study’s criteria, including microbiological evidence, clinical signs of infection, or requirement for surgical intervention (Table 1).
Three reviewers (G.C, S.L.R, C.F.) independently assessed the full texts of selected articles to determine eligibility and extracted relevant data. In cases of disagreement, the senior author (R.V.) made the final decision. Additionally, the risk of bias was evaluated for each study, with any disagreements resolved through consultation with the supervisor.
2.3. Data Extraction and Analysis
Detailed information was systematically extracted from each selected study. The selected studies covered a range of variables including demographic data, type of fracture, surgical methods, and outcomes related to return to sports. Statistical analysis was performed using SPSS 18.0 for Windows (SPSS Inc., Chicago, IL, USA). Descriptive statistics were used to summarize the findings across all the included studies.
3. Results
3.1. Search and Literature Selection
The data analyzed come from scientific studies published between 2000 and 2024. An initial literature search identified 788 papers for potential evaluation. Out of these, 725 were discarded after reviewing their titles and abstracts, as they did not meet the inclusion criteria. In the end, 63 papers were included in the review (Figure 3). The checklist for this study can be found in the Supplementary Materials (Table S1).
3.2. Study Characteristics and Demographics
This systematic review includes data from 63 studies, including a total of 3573 patients who underwent surgical treatment for rhizarthrosis using a trapeziometacarpal joint prosthesis. Among these studies, 37 were retrospective, 19 were prospective and 5 were case reports. The mean age of participants was consistent across the studies, with an average age of 61.2 years. Regarding gender distribution, 569 patients were male (16%) and 2939 were female (82%), although 4 articles did not provide information on gender distribution [Table 2]. Additionally, 20 articles reported the occupational background of the patients, showing a high prevalence of implants among individuals who had engaged in manual work during their lives. The wide variability in patient age, sex distribution, occupational background, and implant selection highlights the heterogeneity of the treated population, supporting the relevance of patient-specific factors in the assessment of prosthetic joint infection risk.
3.3. Type of Prosthesis
The Maia prosthesis emerged as the most used implant, being reported in 10 out of 63 studies included in this review. It was followed, in descending order of frequency, by the Elektra (9/63), Arpe (9/63), Touch (7/63), Ivory (6/63), Moovis (6/63), Isis (3/63), Moje Acamo (3/63), SR TMC (3/63), Motec (2/63), Roseland (2/63), Guepar (2/63), Swanson (2/63), De la Caffiniére (2/63), Rubis II (2/63), and BioPro Modular implants (1/63).
3.4. Infection Rate
Out of 4165 procedures, 15 were complicated by infections. Among these, 6 cases involved superficial infections, while deep infections were reported in 8 cases. One case was classified as suspected deep infection due to the presence of purulent material in the joint and along the stem, although no pathogens were isolated. The specific pathogen was identified in only 2 cases, both involving Staphylococcus aureus; in the remaining cases, microbiological confirmation was not available, likely due to superficial infections, lack of synovial sampling, or incomplete reporting by the original authors. Only two superficial infections were successfully treated with oral antibiotics, while the treatment approach for the remaining cases was not specified. Surgical intervention was performed in 9 cases, including 3 trapeziectomies, 1 debridement with placement of a bone cement spacer and arthrodesis after 6 months, and 1 prosthesis explantation with conversion to resection arthroplasty. In one additional case, the prosthesis was removed, but the authors provided no further details regarding the procedure [Table 3]. In 5 cases the prosthesis involved was Maia. For most patients, detailed information regarding the time from surgery to onset of infection, the type of surgery performed, and the antibiotic treatment used was not available, limiting the ability to classify infections as early or late. Some of the reported infections were superficial and may not meet strict PJI criteria, highlighting the limited epidemiological information available.
4. Discussion
Over the years, TMC prostheses have become a reliable and widely appreciated solution for managing trapezio-metacarpal joint arthritis, offering significant benefits in pain relief, functionality, and quality of life [69]. The first TMC prosthesis was implanted in 1970 [47] and despite it being a long time, the global follow-up remains poor compared with hip and knee implants. While mechanical implant-related complications are more predictable [13], infection rate is something that has not been examined as, so far, no review addressed the topic. In this context, prosthetic joint infection represents a paradigmatic complication in which patient-specific factors, surgical variables, and implant-related characteristics interact, making a personalized and precision medicine approach particularly relevant. With an average implant survival rate of 90–94% after 10 years [17,48], surgeons must be able to detect and efficiently treat infections. Infection is a relatively uncommon complication in elective hand surgery, with an overall incidence of 1.9% [70]. Authors usually refer to infectious complications using the terms superficial SSI (surgical site infection) and deep infection. A first bias in determining the actual infection rate of TMC prosthesis is the appropriateness in classifying the type of infection. This lack of standardized definitions hampers risk stratification and limits the possibility of tailoring diagnostic and therapeutic strategies to individual patients.
According to Centers for Disease Control and Prevention (CDC) [71] a superficial SSI is defined as an infectious process that occurs within 30 days after the operation and that involves only skin or subcutaneous tissue of the incision. The local factors which identify an SSI are: (1) localized swelling, (2) redness, (3) heat while the presence of a stitch abscess with minimal inflammation and discharge confined to the points of suture penetration or SSI that extend into the fascial and muscle layers mustn’t be related to an SSI. The presence of discharge, especially around an exposed K-wire, is a common finding in hand surgery which can be easily mistaken for a sign of infection.
Accurate clinical interpretation is therefore essential to avoid overtreatment or undertreatment, particularly in frail or comorbid patients.
On the other hand, a deep infection occurs within 30 days if no implant is left in place or within 1 year in cases of implants in place. The main sign of deep infection is the presence of purulent drainage from the deep incision or a deep incision which spontaneously dehisces in patients who report fever, localized pain or tenderness. Another element which defines a deep infection is the presence of an abscess or other evidence of infection involving the deep incision. A limited number of studies in the literature specifically addresses infections in TMC. This scarcity of data highlights the pertinence of this review, which aims to provide a comprehensive analysis of infection rates, potential risk factors and recommended management strategies in TMC.
This scarcity of data highlights the importance of synthesizing available evidence to support individualized clinical decision-making in this highly heterogeneous patient population.
Our research found only 12 [6,8,11,12,16,20,35,37,41,46,59,67] articles addressing infections in TMC prosthesis with a total of 15 cases reported. In most cases [8,11,12,20,35,37,46,67] (9/6) a deep infection was described, and this could lead to a lack of data due to the absence of a report from surgeons in case of superficial and self-resolving infections. The overall incidence reported in our study is 0.36% across 4165 procedures which is low but not negligible, considering an infection rate of 0.3–0.5% in bigger joints such as hip and knee [72]. Due to lack of data regarding the onset of symptoms, it was not possible to estimate the rate of early and late infection which could be helpful in stratifying the causes [47,69,73]. This reduced incidence can be attributed to several factors, including the shorter operative time, reduced surgical exposure, and minimal instrumentation involved in TMP procedures [74]. Moreover, as pointed out by Kistler et al., much of the literature on infection rates in hand surgery is based on reoperation rates while ignoring infectious complications treated simply with outpatients antibiotics [75]. Physicians address prosthetic infections using Parvizi infection criteria, which might seem inappropriate [76].Parvizi infection criteria [76] lack usefulness in this field as synovial fluid aspiration is not a common practice also due to the limited articular space as well as histological analysis of the periprosthetic tissue. The limited applicability of existing diagnostic frameworks further supports the need for tailored criteria adapted to small-joint arthroplasty and individual patient characteristics. In our series, the responsible bacteria were identified in only 2 cases [6,12] (both Staphylococcus aureus) through microbiological samples obtained during revision surgery. CRP and ESR could be easily obtained in most cases along with WBC counts to assess infection, but no author specified whether they used them. Therapeutic strategies are heterogeneous and insufficiently detailed. Implant removal is implemented in some cases [6,33,37,45,55] but no consensus exists.
Treatment decisions should therefore be individualized, integrating infection chronicity, host factors, implant stability, microbiological data, and patient functional demands within a precision medicine framework. Medical management must be carried out in conjunction with an infectious diseases specialist, taking into account the patient’s condition, duration of infection, type of microorganism, whether or not the implant has loosened, and signs of osteitis [12].Treatment consists of antibiotic therapy (specifically targeting Staphylococcus aureus) combined with either early debridement and irrigation with replacement of mobile components, or complete removal of the implant, with or without subsequent reimplantation. While trapeziectomy remains a safe and reliable option in cases of infection requiring implant removal, revision surgery may be the best option for younger and more active patients [77].The major point in revision is to assess if there is concomitant loosening of the implant, as pointed out by Chammas et al. [78]. Secondly, it must be verified if the prosthesis is still available. In this latter case, if there is a concomitant destruction of the trapezium revision is not possible trapeziectomy must be performed, otherwise bipolar revision with a new TCM prosthesis can be pursued.
Despite recent advancements, such as standardized protocols for TMC prosthesis loosening [78], no consensus exists regarding infection management. This review highlights the need for dedicated studies to establish clear diagnostic and therapeutic protocols for TMC prosthetic infections. Future research should focus on stratifying infections by onset, identifying specific risk factors, and optimizing treatment strategies tailored to the unique challenges of TMC prostheses. With improved reporting and standardized approaches, surgeons can better address this rare but clinically significant complication.
Study Limitations
This review is limited by the predominance of retrospective studies and small cohorts, reducing the generalizability of findings. Heterogeneity in diagnostic criteria, reporting of infections, and treatment strategies complicates comparisons and standardization. Many studies lacked detailed data on infection timing, pathogens, and long-term outcomes. Variability in implant designs, surgical techniques, and postoperative protocols further limits the consistency of results. Additionally, publication bias may underestimate the true incidence of complications.
Future research with standardized methodologies and larger multicenter trials is needed to address these gaps and enhance infection management in TMC prosthesis surgery.
5. Conclusions
The management of infections TMC prosthesis remains a complex and underexplored area within hand surgery. While the overall infection rate is relatively low compared to larger joint replacements, the lack of consensus on classification, diagnostic criteria, and treatment protocols poses significant challenges.
The heterogeneity of patient characteristics, implant designs, and clinical presentations underscores the necessity of a personalized and precision medicine approach in both prevention and management. Current evidence suggests that early identification and prompt, tailored intervention—whether medical, surgical, or a combination of both—are critical for preserving joint functionality and patient quality of life. Individualized treatment strategies, integrating patient-specific risk factors, microbiological data, and functional demands, may optimize outcomes and reduce unnecessary implant removal. Future research should focus on developing standardized guidelines for infection management and stratifying risk factors to improve outcomes. This review highlights the necessity of a multidisciplinary approach and underscores the importance of individualized care to address the nuanced complications of TMC joint prosthesis infections.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Haara M.M. Heliövaara M. Kröger H. Arokoski J.P. Manninen P. Kärkkäinen A. Knekt P. Impivaara O. Aromaa A. Osteoarthritis in the carpometacarpal joint of the thumb. Prevalence and associations with disability and mortality J. Bone Jt. Surg. Am.2004861452145710.2106/00004623-200407000-0001315252092 · doi ↗ · pubmed ↗
- 2Baker R.H.J. Al-Shukri J. Davis T.R.C. Evidence-based medicine: Thumb basal joint arthritis Plast. Reconstr. Surg.2017139256 e 266e 10.1097/PRS.000000000000285828027259 · doi ↗ · pubmed ↗
- 3Gillis J. Calder K. Williams J. Review of thumb carpometacarpal arthritis classification treatment and outcomes Can. J. Plast. Surg.20111913413810.1177/22925503110190040923204884 PMC 3249665 · doi ↗ · pubmed ↗
- 4Van Heest A.E. Kallemeier P. Thumb carpal metacarpal arthritis J. Am. Acad. Orthop. Surg.20081614015110.5435/00124635-200803000-0000518316712 · doi ↗ · pubmed ↗
- 5Goubau J.F. Goorens C.K. Van Hoonacker P. Berghs B. Kerckhove D. Scheerlinck T. Clinical and radiological outcomes of the Ivory arthroplasty for trapeziometacarpal joint osteoarthritis with a minimum of 5 years of follow-up a prospective single-centre cohort study J. Hand Surg. Eur.20133886687410.1177/175319341348849423677958 · doi ↗ · pubmed ↗
- 6Mac Dermid J.C. Roth J.H. Rampersaud Y.R. Bain G.I. Trapezial arthroplasty with silicone rubber implantation for advanced osteoarthritis of the trapeziometacarpal joint of the thumb Can. J. Surg.20034610311012691346 PMC 3211682 · pubmed ↗
- 7De la Caffiniere J.Y. Aucouturier P. Trapezio-metacarpal arthroplasty by total prosthesis Hand 197911414610.1016/S 0072-968X(79)80007-8488776 · doi ↗ · pubmed ↗
- 8Cebrian-Gomez R. Lizaur-Utrilla A. Sebastia-Forcada E. Lopez-Prats F.A. Outcomes of cementless joint prosthesis versus tendon interposition for trapeziometacarpal osteoarthritis a prospective study J. Hand Surg. Eur.20194415115810.1177/175319341878715130016903 · doi ↗ · pubmed ↗