Eosinophilic Gastrointestinal Disease After Pediatric Organ and Bone Marrow Transplantation
Erin Sinai, Bridget E. Wilson, Melissa Pecak, Shauna Schroeder, Edward L. Swing, Cindy Bauer

TL;DR
This study explores how different types of organ and bone marrow transplants in children are linked to specific forms of eosinophilic gastrointestinal disease.
Contribution
The study identifies a novel association between multivisceral transplants and a specific subtype of EGID (EoE + EoG).
Findings
EoE + EoG was significantly more common in multivisceral transplant recipients compared to liver transplant recipients.
GER and oral allergy syndrome varied significantly between transplant groups.
No significant differences were found in symptoms, histologic features, or medication responses across transplant types.
Abstract
Previous studies have shown an increased prevalence of eosinophilic gastrointestinal disease (EGID) in pediatric liver and heart transplant recipients. However, EGID after other solid organ and bone marrow transplantations has not been extensively evaluated. The purpose of this study is to determine relationships between subsets of EGID with different solid organ and bone marrow transplants in pediatric patients. We performed a single‐center retrospective chart review of pediatric patients with transplant and EGID between 2007 and 2023. For comparison between transplant groups, ANOVA was used for statistical analysis of continuous variables, and Fisher's exact test was used for categorical variables. There were 30 patients with EGID (eosinophilic esophagitis [EoE] = 21; eosinophilic gastritis [EoG] = 4; EoE + EoG = 3; EoE + eosinophilic colitis [EoC] = 1; eosinophilic duodenitis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
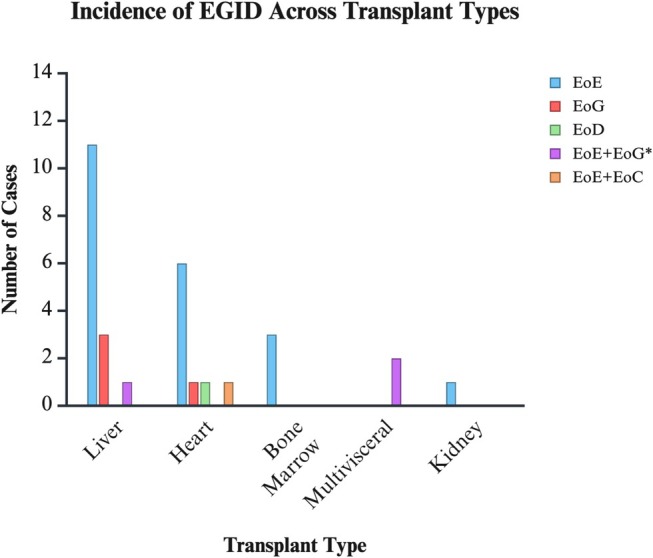 FIGURE 1
FIGURE 1| Age | Months |
| Mean age at transplant, range | 37.4 (1–226) |
| Sex | Number of patients (%) |
| Male | 14 (47%) |
| Race | |
| Native American | 2 (7%) |
| Asian | 1 (3%) |
| Black | 2 (7%) |
| White | 25 (83%) |
| Ethnicity | |
| Hispanic | 12 (40%) |
| Non‐Hispanic | 16 (53%) |
| Not reported | 2 (7%) |
| Medical insurance | |
| Private | 19 (63%) |
| Atopic conditions before first transplant | |
| Asthma | 1 (3%) |
| Allergic rhinitis ± conjunctivitis | 1 (3%) |
| Atopic dermatitis | 3 (10%) |
| None | 27 (90%) |
| Family history of atopy | 9 (30%) |
| Family history of EGID | 3 (10%) |
| Gastrointestinal symptoms before first transplant | |
| Dysphagia or feeding dysfunction | 2 (7%) |
| Abdominal pain | 4 (13%) |
| Vomiting | 4 (13%) |
| Diarrhea/loose stool | 2 (7%) |
| Constipation | 3 (10%) |
| Gastroesophageal reflux | 2 (7%) |
| Poor weight gain/weight loss | 3 (10%) |
| None | 22 (73%) |
| Transplant | Liver | Heart | Bone marrow | Multivisceral | Kidney |
|
|---|---|---|---|---|---|---|
| Number of patients, | 15 | 9 | 3 | 2 | 1 | — |
| EGID, | ||||||
| EoE | 11 (73%) | 6 (67%) | 3 (100%) | 0 | 1 (100%) | 0.210 |
| EoG | 3 (20%) | 1 (11%) | 0 | 0 | 0 | 1.000 |
| EoD | 0 | 1 (11%) | 0 | 0 | 0 | 0.500 |
| EoE + EoG | 1 (7%) | 0 | 0 | 2 (100%) | 0 | 0.011 |
| EoE + EoC | 0 | 1 (11%) | 0 | 0 | 0 | 0.500 |
| Eosinophils/hpf on diagnostic scope, mean (SD) | ||||||
| Upper esophagus | 16.1 (14.2) | 36.0 (31.9) | 45.3 (41.1) | 0.5 (0.7) | 36 | 0.156 |
| Middle esophagus | 21.6 (39.2) | 22.1 (27.2) | 6.7 (11.5) | 0 | 20 | 0.869 |
| Lower esophagus | 41.2 (25.8) | 23.7 (25.3) | 39.0 (14.9) | 18.5 (2.1) | 32 | 0.525 |
| Gastric body | 42.0 (44.4) | 19.5 (27.6) | — | 20.0 (28.3) | — | 0.732 |
| Gastric antrum | 49.3 (43.5) | 63.5 (51.6) | — | 50.0 (70.7) | — | 0.947 |
| Morphologic features on diagnostic scope, | ||||||
| Linear furrows | 4 (27%) | 3 (33%) | 1 (33%) | 0 | 0 | 1.000 |
| White papules | 1 (7%) | 0 | 0 | 0 | 0 | 1.000 |
| Edema | 0 | 1 (11%) | 1 (33%) | 0 | 0 | 0.193 |
| Erythema | 0 | 0 | 1 (33%) | 0 | 0 | 0.200 |
| Erosion/ulceration | 3 (20%) | 0 | 0 | 0 | 0 | 0.634 |
| Corrugated mucosa | 1 (7%) | 0 | 0 | 0 | 0 | 1.000 |
| None | 6 (40%) | 6 (67%) | 1 (33%) | 2 (100%) | 1 (100%) | 0.369 |
| Months between transplant and diagnostic scope, mean (SD) | 64.9 (60.4) | 56.7 (52.9) | 65.0 (91.9) | 97.0 (1.4) | 90 | 0.894 |
| Comorbid GI disorders, | ||||||
| GER | 1 (7%) | 2 (22%) | 2 (67%) | 0 | 1 (100%) | 0.036 |
| Celiac disease | 0 | 0 | 0 | 1 (50%) | 0 | 0.100 |
| Inflammatory bowel disease | 0 | 1 (11%) | 0 | 1 | 0 | 0.131 |
| Dysmotility/gastroparesis | 1 (7%) | 0 | 0 | 0 | 0 | 1.000 |
| Rumination | 1 (7%) | 0 | 0 | 0 | 0 | 1.000 |
| Chronic constipation | 1 (7%) | 0 | 1 (33%) | 0 | 0 | 0.448 |
| Enteral feeding tube | 4 (27%) | 5 (56%) | 0 | 0 | 0 | 0.690 |
| Short bowel | 2 (13%) | 0 | 0 | 1 (50%) | 0 | 0.278 |
| Gastroschisis | 1 (7%) | 0 | 0 | 0 | 0 | 1.000 |
| GI bleed | 0 | 0 | 0 | 1 (50%) | 0 | 0.100 |
| Total parenteral nutrition‐induced cholestasis | 1 (7%) | 0 | 0 | 0 | 0 | 1.000 |
| Small intestinal bacterial overgrowth | 1 (7%) | 0 | 0 | 0 | 0 | 1.000 |
| Post‐transplant lymphoproliferative disease of GI tract | 0 | 1 (11%) | 0 | 0 | 0 | 0.500 |
| Comorbid atopic conditions, | ||||||
| Allergic rhinitis ± conjunctivitis | 6 (40%) | 3 (33%) | 2 (67%) | 1 (50%) | 1 (100%) | 0.783 |
| Atopic dermatitis | 7 (47%) | 3 (33%) | 2 (67%) | 0 | 0 | 0.688 |
| IgE‐mediated food allergy | 2 (13%) | 0 | 0 | 0 | 0 | 0.690 |
| Oral allergy syndrome | 0 | 0 | 0 | 0 | 1 (100%) | 0.033 |
| Asthma | 3 (20%) | 2 (22%) | 1 (33%) | 0 | 1 (100%) | 0.471 |
| Symptoms leading to GI evaluation, | ||||||
| Dysphagia | 2 (13%) | 5 (56%) | 1 (33%) | 0 | 1 (100%) | 0.079 |
| Food impaction | 1 (7%) | 1 (11%) | 0 | 0 | 0 | 1.000 |
| Abdominal pain | 5 (33%) | 4 (44%) | 1 (33%) | 1 (50%) | 0 | 0.954 |
| Nausea | 1 (7%) | 0 | 1 (33%) | 0 | 0 | 0.448 |
| Vomiting | 6 (40%) | 4 (44%) | 2 (67%) | 0 | 0 | 0.754 |
| Diarrhea/loose stool | 3 (20%) | 4 (44%) | 1 (33%) | 0 | 0 | 0.646 |
| Poor weight gain/weight loss | 5 (33%) | 5 (56%) | 0 | 0 | 1 (100%) | 0.246 |
| Food avoidance | 4 (27%) | 2 (22%) | 0 | 0 | 0 | 1.000 |
| Cough/difficulty breathing after eating | 1 (7%) | 0 | 0 | 0 | 1 (100%) | 0.090 |
| Bloating | 1 (7%) | 0 | 0 | 0 | 0 | 1.000 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEosinophilic Esophagitis · Eosinophilic Disorders and Syndromes · Microscopic Colitis
Introduction
1
Eosinophilic gastrointestinal disease (EGID) represents a group of allergic inflammatory disorders of the gastrointestinal tract characterized by eosinophilic inflammation [1]. As the incidence of EGID in pediatric populations rises, there has been an even greater increase in EGID amongst post‐organ transplant pediatric patients [2]. This relationship between pediatric patients who underwent an organ transplant and subsequently developed EGID is thought to be due to mechanisms involving immune dysregulation due to immunosuppressive therapy, rejection episodes, food allergies, and viral infections [3, 4]. Previous studies have focused primarily on liver and heart transplant recipients, while differences in transplant type, immunosuppression, types of EGID, and remission treatments have not yet been explored [5, 6].
Pediatric liver transplant recipients that later developed EGID were found to have higher rates of comorbid IgE‐mediated food allergy, allergic rhinitis, asthma, and eczema, which could have put these patients at higher risk for later developing EGID post transplantation [5]. Further studies found a relationship between specific immunosuppressive medications, tacrolimus, and EGID incidence after liver transplantation [3, 5, 7, 8]. Specifically, tacrolimus may contribute to EGID by selectively suppressing Th1 lymphocytes while promoting the Th2 signal pathway, leading to an immune imbalance that enhances IL‐4 and IL‐5 production, driving eosinophilic recruitment and activation [9]. Similar findings were confirmed in pediatric heart transplantation studies [4, 9].
In this study from a single pediatric medical center, we investigated the relationship between various types of EGID in patients with bone marrow transplants (BMTs) and other solid organ transplants, including liver, heart, kidney, and multivisceral (liver, small bowel, and pancreas). The types of EGID analyzed include eosinophilic esophagitis (EoE), eosinophilic gastritis (EoG), eosinophilic duodenitis (EoD), and eosinophilic colitis (EoC), and combinations of the subtypes were included, including EoE + EoG and EoE + EoC. To our knowledge, this is the first study to characterize EGID in pediatric bone marrow and multivisceral transplant patients, providing novel insights into this complication in these populations. The purpose of this study is to determine relationships between subsets of EGID with different solid organ transplants and BMTs in pediatric patients.
Methods
2
This was an IRB‐approved (IRB‐23‐019) retrospective study of pediatric patients with solid organ transplant or BMT who were diagnosed with eosinophilic gastrointestinal disorders (EGID) at a medical center between 2007 and 2023. Patients were identified using ICD‐10 codes for EGID and transplant status: K52.81 (eosinophilic gastritis), K52.82 (eosinophilic colitis), Z94.0, Z94.1, Z94.2, Z94.3, Z94.4, Z94.81, Z94.82, Z94.83, Z94.84, and Z94.9. EGID was defined by established eosinophil thresholds: EoE ≥ 15 eos/hpf; EoG ≥ 30; EoD ≥ 52; right colon ≥ 100; transverse/descending colon ≥ 84; rectosigmoid ≥ 64 eos/hpf. Only biopsies meeting these thresholds were included. All data were de‐identified in REDCap. Pathology reviewers were blinded to transplant status. Patients were excluded if > 18 years, had a prior EGID diagnosis before transplant, or did not meet biopsy criteria. Diagnostic definitions were based on chart documentation and ICD‐10 coding. GER was identified through provider documentation and/or relevant ICD‐10 codes. ICD‐10 codes. Oral allergy syndrome (OAS) was defined by documented symptoms triggered by fresh fruits or vegetables, often accompanied by a food‐allergy ICD‐10 code. Histologic remission was defined as eosinophil counts below the site‐specific thresholds listed above. Medical records were reviewed to extract demographic and clinical data, including transplant type, EGID characteristics, and treatment history. Peripheral eosinophils were taken from available CBC/diff results. Because this was a retrospective review, timing was not standardized; we recorded the peak absolute eosinophil count documented for each patient. The age‐specific reference range at our institution is 0.05–0.70 × 10^9^/L. All patients were evaluated using a standardized clinical intake process, which included specific documentation of gastrointestinal symptoms (e.g., reflux, dysphagia, and abdominal pain) and relevant history, such as family history of atopy. Descriptive statistics were used to summarize the data for all patients. For comparisons between transplant groups, ANOVA was performed for continuous variables, and Fisher's exact test was used for categorical variables. All statistical analyses were conducted using SPSS statistical software (version 17.0).
Results
3
Thirty pediatric transplant recipients with EGID, including EoE, EoG, EoD, and EoC, and combinations of the subtypes were included, including EoE + EoG and EoE + EoC. Transplants included liver (n = 15), heart (n = 9), bone marrow (n = 3), multivisceral (n = 2), and kidney (n = 1). Of these, 47% were male and 40% were Hispanic. The mean age at the time of transplant was 37 months, with most patients having no atopic conditions before transplant (27/30, 90%). In general, most had no family history of atopy (21/30, 70%), and only 3 (10%) had a family history of EGID (Table 1). The average number of months between transplant and diagnostic esophagogastroduodenoscopy ± colonoscopy was 66.5 months, with the most common symptom leading to gastroenterology evaluation being vomiting (12/30, 40%). The average peak peripheral eosinophil count was 1.09 × 10^9^/L (range: 0.3–4.1). Additional demographic and baseline data are in Table 1.
When comparing the various transplant groups, there was a significant difference in the incidence of EoE + EoG between all transplant groups, with EoE + EoG present in the 2 multivisceral transplant patients (p = 0.011; Table 2). These patients did not have underlying graft‐versus‐host disease (GVHD) or drug infections. One patient had post‐transplant lymphoproliferative disorder (PTLD). There were no other significant differences between EGID subtypes and transplant types (Figure 1).
Incidence of EGID across different solid organ and bone marrow transplants in pediatric patients.
A statistically significant difference in the presence of comorbid gastroesophageal reflux (GER) between groups was noted (p = 0.036; Table 2). Specifically, GER was present in one kidney (100%), one liver (1/15, 7%), two hearts (2/9, 22%), two bone marrows (2/3, 67%), and zero multivisceral transplant patients. OAS was diagnosed in the one kidney transplant patient but not in the other transplant patients (p = 0.033; Table 2).
Various immunosuppressant medications were used for induction and post‐solid organ transplant for the patients, including tacrolimus, mycophenolate, sirolimus, and glucocorticoids. Treatment with thymoglobulin during induction (p = 0.02; kidney n = 1; heart n = 4) and glucocorticoids during maintenance (p = 0.039; kidney n = 1, liver n = 3, heart n = 1, multivisceral n = 1) was associated with EoC incidence. For the other EGID subtypes, there was no association with specific induction or maintenance immunosuppressant medications. Similarly, there were no differences between morphologic features or eosinophils/high‐power field on diagnostic endoscopy; maximum recorded peripheral eosinophil count; achievement of histologic remission; medications leading to EGID remission; or family history of atopy or EGID. Additional results are summarized in Table 2.
Discussion
4
This study provides new insights into the incidence and characteristics of EGID in pediatric transplant recipients, showing significant associations with a variety of transplant types and comorbid conditions. Specifically, we found significant differences in the incidence of EoE + EoG between groups, with increased prevalence in the multivisceral transplant population. We also observed that thymoglobulin use during induction and glucocorticoid use during maintenance were associated with EoC incidence. This uniquely highlights the importance of studying EGID in all types of pediatric transplant recipients in addition to liver and heart.
Previous studies describe the relationship between peripheral eosinophilia and EGID after pediatric transplants with immunosuppressant medications [8, 10]. Immunosuppressant medications, specifically tacrolimus, have been linked to increased eosinophil production through differential inhibition of cytokine elaboration, which might alter the balance between Th1 and Th2 T‐cell subsets [7]. In contrast, in our study we found no differences in peripheral eosinophilia counts and EGID types with different immunosuppressant medications, including tacrolimus. However, we found that thymoglobulin use during induction and glucocorticoid use during maintenance had significant associations with EoC, while the exact mechanism for this association remains unclear. Previous studies have demonstrated a significant association between thymoglobulin and the development of PTLD in pediatric patients who have undergone bone marrow or multivisceral transplantation. While PTLD is distinct from EoC, both conditions may share underlying mechanisms related to immune dysregulation induced by immunosuppressive therapy. Thymoglobulin's potent T‐cell depletion may contribute to an imbalance in immune signaling, potentially favoring Th2‐driven eosinophilic inflammation in EGID while also creating an environment conducive to uncontrolled lymphoproliferation in PTLD [11, 12].
Previous studies have shown other causes of inflammation that lead to eosinophilia in transplant patients. These include drug reactions, infections, PTLD, and GVHD [3, 13]. Only one of our patients had comorbid PTLD, and no cases were attributed to drug interactions, infections, or GVHD. All diagnoses of EGID in our cohort were confirmed through endoscopy and histologic examination. Therefore, we can conclude that these cases of eosinophilia in our post‐transplant patients were related to EGID.
Ozdogan et al. demonstrated higher rates of allergen sensitization and atopy in liver transplant recipients with EGID when compared to those without EGID [2]. In our study, most patients did not have comorbid atopic conditions. This may be attributed to the younger median age at transplantation in our study population, which could mean that some patients had not yet developed atopic conditions at the time of analysis. The relationship between age at transplantation and the incidence of EGID has been explored in prior studies, with younger age identified as a risk factor for developing posttransplant allergic conditions, including EGID [2, 10]. The proposed mechanism involves immune dysregulation and an imbalance in immune signaling associated with early immune system development. Younger patients have an immature immune system that may be more prone to Th2‐skewed immune responses, leading to increased production of cytokines like IL‐4 and IL‐5, which drive eosinophilic recruitment and activation. In addition, early‐life immune disruptions, such as exposure to immunosuppressants like tacrolimus, may selectively suppress Th1 responses while promoting Th2 dominance, further enhancing allergic and eosinophilic inflammation. This heightened reactivity increases the risk of EGID development post‐transplant [2, 3, 6].
Clinically, these findings may help guide earlier screening in pediatric patients with EGID symptoms after solid organ and BMT. The association with immunosuppressant exposure suggests that immune modulation may play a role in disease mechanisms, although this requires further investigation. While exploratory, our results may inform future studies aimed at understanding potential inflammatory or immune‐mediated pathways.
This study has several limitations. First, its single‐center retrospective design introduces risks of selection and information bias, particularly because case identification relied on ICD‐10 code extraction and available chart documentation. The small sample size, especially in certain transplant groups, and imbalanced cohort distribution limit generalizability. Variability in pathologic criteria and biopsy availability, along with missing data on PPI use, dietary exposures, and avoidance history, may affect interpretation of eosinophil severity. Follow‐up duration also varied across patients, limiting assessment of longitudinal outcomes. Endoscopic evaluation was not performed uniformly, so the true incidence of EGID in transplant recipients remains unknown, and some cases may have been missed due to vague symptoms or immunosuppression blunting disease presentation. We were also unable to calculate incidence by transplant type without the total number of transplant recipients. Finally, this study is exploratory and identifies associations rather than causal relationships; mechanistic links, including those involving immunosuppressive agents, require further study.
Conclusion
5
To our knowledge, this is the largest cohort of multivisceral and BMT patients with EGID reported to date. In this population, we found all the patients with multivisceral transplants developed EoE + EoG, though a clear limitation is the small size of this group (n = 2). While previous reports describe an increase in the prevalence of post‐transplant allergy and autoimmune disorders in patients with multivisceral transplants, the relationship with EoE + EoG could be due to the altered immune response following multivisceral transplantation. Future studies including larger numbers of non‐liver and non‐heart transplant patients with EGID are needed to better understand the disease progression and chronicity of EGID in patients with transplantation. By broadening the scope of future studies to include diverse transplant populations, we can enhance our understanding and management of EGID in this unique group of patients.
Author Contributions
Erin Sinai: data collection, drafting manuscript. Bridget E. Wilson: planning, drafting the manuscript. Melissa Pecak: data collection. Shauna Schroeder: planning, drafting the manuscript. Edward L. Swing: interpreting data. Cindy Bauer: planning, drafting the manuscript. All authors have approved the final draft being submitted.
Funding
The authors have nothing to report.
Ethics Statement
This study was approved by the IRB‐23‐019.
Consent
Informed consent was obtained from legal guardians.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. Licari , M. Votto , E. D'Auria , R. Castagnoli , S. M. E. Caimmi , and G. L. Marseglia , “Eosinophilic Gastrointestinal Diseases in Children: A Practical Review,” Current Pediatric Reviews 16, no. 2 (2020): 106–114, 10.2174/1573396315666191022154432.31642786 · doi ↗ · pubmed ↗
- 2E. Ozdogan , L. Doganay , D. Can , and C. Arikan , “Disease Course and Treatment Response of Eosinophilic Gastrointestinal Diseases in Children With Liver Transplantation: Long‐Term Follow‐Up,” American Journal of Gastroenterology 116, no. 1 (2021): 188–197, 10.14309/ajg.0000000000000934.33065587 · doi ↗ · pubmed ↗
- 3R. Romero , C. R. Abramowsky , T. Pillen , G. A. Smallwood , and T. G. Heffron , “Peripheral Eosinophilia and Eosinophilic Gastroenteritis After Pediatric Liver Transplantation,” Pediatric Transplantation 7, no. 6 (2003): 484–488, 10.1046/j.1397-3142.2003.00116.x.14870899 · doi ↗ · pubmed ↗
- 4J. W. Bush , S. Mohammad , H. Melin‐Aldana , A. F. Kagalwalla , and N. C. Arva , “Eosinophilic Density in Graft Biopsies Positive for Rejection and Blood Eosinophil Count Can Predict Development of Post‐Transplant Digestive Tract Eosinophilia,” Pediatric Transplantation 20, no. 4 (2016): 540–551, 10.1111/petr.12693.26917244 · doi ↗ · pubmed ↗
- 5J. Wisniewski , J. Lieberman , A. Nowak‐Weogonekgrzyn , et al., “De Novo Food Sensitization and Eosinophilic Gastrointestinal Disease in Children Post‐Liver Transplantation,” Clinical Transplantation 26 (2012): E 365–E 371, 10.1111/j.1399-0012.2012.01670.x.22694084 · doi ↗ · pubmed ↗
- 6J. H. Mouledoux , E. L. Albers , Z. Lu , B. R. Saville , D. J. Moore , and D. A. Dodd , “Clinical Predictors of Autoimmune and Severe Atopic Disease in Pediatric Heart Transplant Recipients,” Pediatric Transplantation 18, no. 2 (2014): 197–203, 10.1111/petr.12205.24372990 PMC 3988248 · doi ↗ · pubmed ↗
- 7S. A. Saeed , M. J. Integlia , R. G. Pleskow , et al., “Tacrolimus‐Associated Eosinophilic Gastroenterocolitis in Pediatric Liver Transplant Recipients: Role of Potential Food Allergies in Pathogenesis,” Pediatric Transplantation 10, no. 6 (2006): 730–735, 10.1111/j.1399-3046.2006.00538.x.16911498 · doi ↗ · pubmed ↗
- 8J. H. Lee , H. Y. Park , Y. H. Choe , S. Lee , and S. Il Lee , “The Development of Eosinophilic Colitis After Liver Transplantation in Children,” Pediatric Transplantation 11, no. 5 (2007): 518–523, 10.1111/j.1399-3046.2007.00693.x.17631020 · doi ↗ · pubmed ↗