Effect of caffeine ingestion on cycling performance: a systematic review and meta-analysis
Jinyan Wu, Kai Xu, Mingyue Yin, Xianming Ding, Tong Wang, Qiubo Zhang, Xiaowei Wu, Ningkun Xiao

TL;DR
This study shows that caffeine improves cycling performance, with low doses being as effective as higher ones.
Contribution
The study provides a meta-analysis on caffeine's effect on cycling performance, highlighting dosage and age as key factors.
Findings
Caffeine significantly reduced cycling completion time and increased mean power output.
Low caffeine doses (≤3 mg/kg) were more effective than higher doses in reducing completion time.
Age significantly moderated the effect of caffeine on cycling performance.
Abstract
This study aimed to determine the effects of acute caffeine ingestion on cycling performance through a systematic review and meta-analysis, while also exploring the moderating roles of caffeine dosage, training status, and athlete age. A comprehensive search was conducted across five databases, yielding 20 eligible studies with a total of 226 participants. A three-level mixed-effects model was applied to pool main effects on cycling time trial performance, mean power output, mean heart rate, and ratings of perceived exertion (RPE). Subgroup analyses and meta-regression were performed to examine potential moderators. Caffeine intake significantly reduced cycling completion time (SMD = −0.36, 95% CI: −0.57 to −0.15, p = 0.0017) and increased mean power output (SMD = 0.29, 95% CI: 0.05 to 0.52, p = 0.02), but had no significant effect on heart rate or RPE. Subgroup analysis indicated that…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
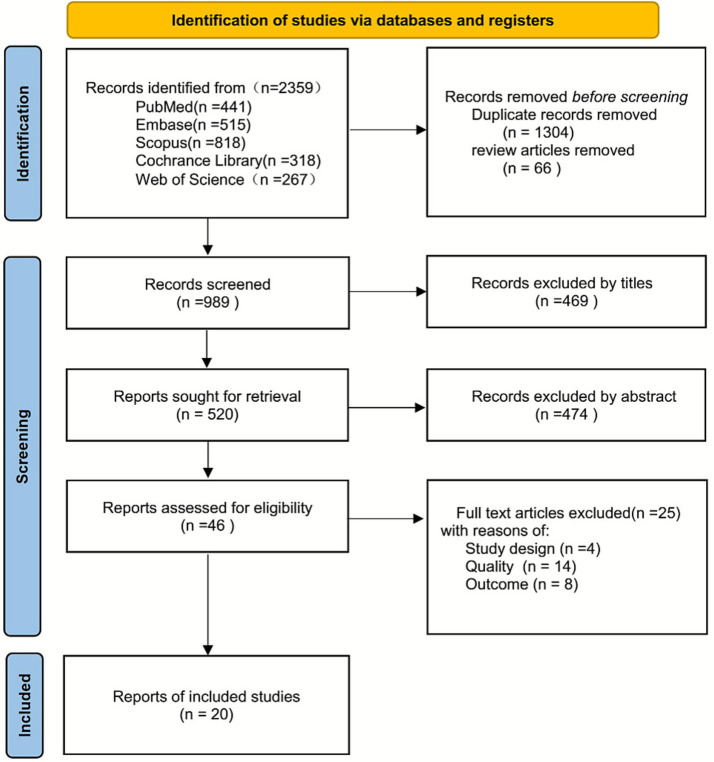 Figure 1
Figure 1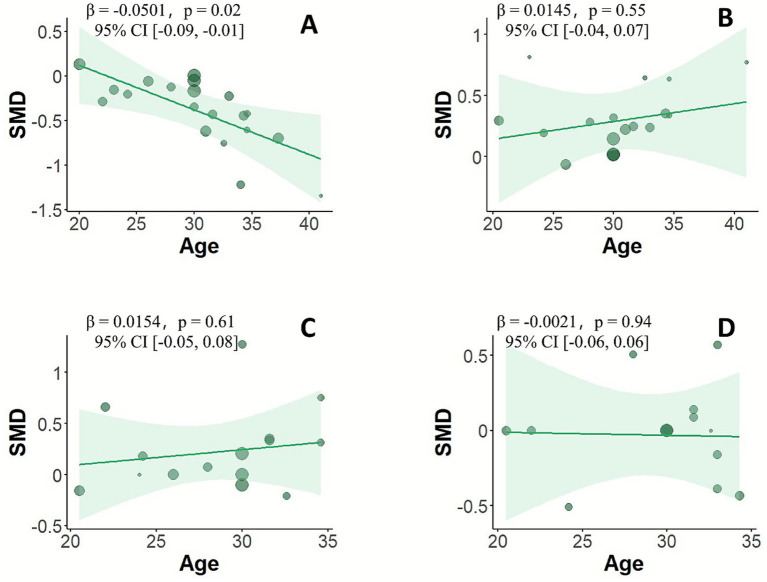 Figure 2
Figure 2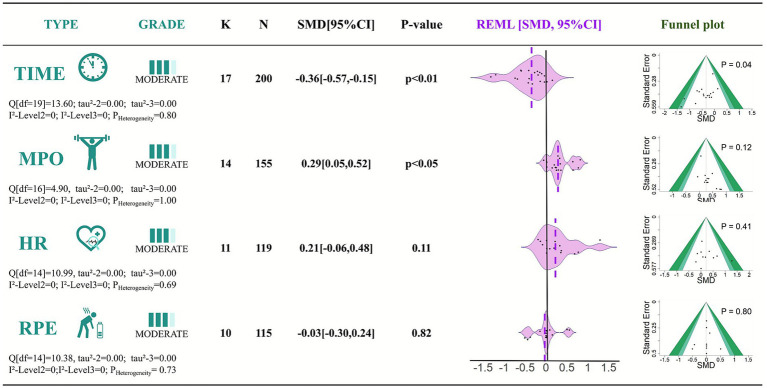 Figure 3
Figure 3| Study | Country | Sample | Age | training level | Cycling protocol | Timing | Doses | From | Measures | Results |
|---|---|---|---|---|---|---|---|---|---|---|
| Backhouse | UK | 6 | 24 ± 1 | Well-trained | 90 min VO2 max 70% | 60 | 6 | Solution | ③ | ③↑ |
| Santos | Brazil | 8 | 32.6 ± 5.4 | Well-trained | TT: 4KM | 60 | 5 | Capsule | ①②③④ | ①↓②↑③↔④↔ |
| Lee | USA | 15 | 37.3 ± 2.5 | Well-trained | 8mi | 5 | Total 70 mg | Tablets | ① | ①↓ |
| Paton | New Zealand | 20 | 30 ± 10 | Well-trained | TT:30 km | After 10 km | 3–4 | Gum | ①②③④ | ①↓②↑③↔④↔ |
| Bottoms | UK | 12 | 20.5 ± 0.7 | Recreational | 30 min | Every 6 min | Total 32 mg | Mouthwash | ②③④ | ②↑③↔④↔ |
| Quinlivan | Australia | 11 | 31.6 ± 6.1 | Well-trained | 60 min | 90 | 3 | Capsule | ①②③④ | ①↓②↑③↑④↑ |
| Kizzi | UK | 8 | 23 ± 2 | Recreational | 90 min VO2 max 70%; | Before | 6 | Mouthwash | ② | ②↑ |
| Alvarenga | Brazil | 12 | 34.3 ± 6.2 | Recreational | TT: 20 km | 50 | 5 | Capsule | ①②④ | ①↓②↑④↓ |
| Tomazini | Brazil | 11 | 33 ± 7 | Well-trained | TT: 4 km | 50 | 5 | Capsule | ①②④ | ①↓②↑④↓ |
| Lei | China | 16 | 20 ± 2 | Recreational | VO2 max 80%, 60 rpm | 60 | 6 | Capsule | ① | ①↓ |
| Colmena | Spain | 11 | 22 ± 3 | Recreational | TT: 13.9 km | 60 | 3 | Solution | ①③④ | ①↓③↑④↔ |
| John | Australia | 12 | 23 ± 4 | Recreational | 35 °C, 40%RH | 60 | 5 | Capsule | ① | ①↓ |
| Santos | Brazil | 8 | 34.6 ± 5.0 | Well-trained | TT: 4 km | 60 | 5 | Capsule | ①②③ | ①↓②↑③↑ |
| Hewitt | Usa | 10 | 28 ± 9 | Na | 20minVO2max 60%; | 60 | 6 | Capsule | ①②③④ | ①↓②↑③↔④↑ |
| Spence | Australia | 10 | 30 ± 2 | Well-trained | TT: 40 km | 60 | 2.5 | Capsule | ①②③④ | ①↓②↑③↑④↔ |
| Skinner | Australia | 14 | 31.0 ± 5.2 | Well-trained | TT: 40 km | 60 | 6 | Capsule | ①② | ①↓②↑ |
| Kilding | New Zealand | 10 | 24.2 ± 5.4 | Well-trained | TT: 3 km | 60 | 3 | Capsule | ①②③④ | ①↓②↑③↑④↓ |
| Hodgson | Uk | 8 | 41 ± 7 | Well-trained | 30 mi | 60 | 5 | Capsule | ①② | ①↓②↑ |
| Bortolotti | Brazil | 13 | 26 ± 10 | Well-trained | TT:20 km | 60 | 6 | Capsule | ①②③ | ①↓②↑③↔ |
| Felippe | Brazil | 11 | 34 ± 4 | Recreational | TT:4 km | 75 | 5 | Capsule | ① | ①↓ |
| Subgroup |
|
| SMD [95%CI] |
| |
|---|---|---|---|---|---|
| TIME | |||||
| ≤3 mg/kg | 5 | 57 | −0.42[−0.81,-0.02] | <0.05 | 0 |
| 4 ~ 6 mg/kg | 12 | 143 | −0.34[−0.59,-0.10] | <0.01 | 2.48 |
| Well-trained | 12 | 138 | −0.38[−0.63,-0.13] | <0.01 | 0 |
| Recreational | 5 | 62 | −0.32[−0.71,−0.06] | 0.09 | 26.62 |
| MPO | |||||
| ≤3 mg/kg | 4 | 43 | 0.27[−0.20,0.73] | 0.24 | 0 |
| 4 ~ 6 mg/kg | 10 | 112 | 0.29[0.02,0.57] | <0.05 | 0 |
| Well-trained | 11 | 123 | 0.25[−0.01,0.51] | 0.06 | 0 |
| Recreational | 3 | 32 | 0.44[0.10,0.98] | <0.10 | 0 |
| HR | |||||
| ≤3 mg/kg | 5 | 54 | 0.41[−0.01,0.82] | 0.05 | 24.66 |
| 4 ~ 6 mg/kg | 6 | 65 | 0.07[−0.29,0.42] | 0.69 | 0 |
| Well-trained | 9 | 96 | 0.21[−0.09,0.51] | 0.15 | 0 |
| Recreational | 2 | 23 | 0.23[−0.42,0.87] | 0.46 | 46.53 |
| RPE | |||||
| ≤3 mg/kg | 5 | 54 | -0.06[−0.47,0.35] | 0.75 | 0 |
| 4 ~ 6 mg/kg | 5 | 61 | −0.004[−0.37,0.36] | 0.95 | 6.35 |
| Well-trained | 7 | 80 | 0.01[−0.30,0.33] | 0.92 | 0 |
| Recreational | 3 | 35 | −0.15[−0.67,0.37] | 0.55 | 0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoffee research and impacts · Muscle metabolism and nutrition · Pharmacology and Obesity Treatment
Introduction
1
In recent years, nutritional supplementation has been widely recognized as an important ergogenic aid to enhance athletic performance, delay fatigue, and improve metabolic regulation (1, 2). Among the numerous supplements, caffeine has become one of the most popular due to its accessibility and well-documented efficacy in both elite and recreational sports (3, 4). Acute caffeine ingestion exerts its ergogenic effects through multiple mechanisms, including antagonism of adenosine receptors, increased central nervous system excitability, enhanced muscle contractility, promotion of fat mobilization and utilization, and reduced perceived exertion during exercise (5–7). These mechanisms make caffeine particularly promising in endurance-based sports (8–10).
Cycling, due to its standardized format and strong experimental controllability, has been widely used as a model for evaluating the ergogenic effects of nutritional interventions, including caffeine (11–13). Although numerous studies have investigated the acute effects of caffeine on cycling performance (14–16), the findings remain inconsistent. Several studies reported that caffeine significantly reduced time trial completion time and improved power output (17–19), whereas others failed to observe significant effects and even noted large inter-individual variability in responses (20). A recent meta-analysis summarized the effects of caffeine ingestion on cycling time trials and demonstrated significant improvements in completion time and mean power output (21).
However, considering that the previous review included a limited number of studies, did not comprehensively cover endurance-related performance outcomes, and did not clearly evaluate the certainty of evidence using GRADE, it is necessary to conduct a more rigorous synthesis of the literature—one that incorporates a broader range of endurance performance indicators and employs more advanced analytical methods (three-level meta-analytic approach). Such an effort would allow for a more robust evaluation of the ergogenic effects of caffeine during cycling and enable further exploration of potential moderators, thereby providing stronger evidence to support nutritional strategies in athletic practice. Therefore, the present study aimed to systematically review and meta-analyze high-quality research on the acute effects of caffeine ingestion on cycling performance, with a focus on key outcomes including cycling completion time, power output, mean heart rate, and ratings of perceived exertion.
Materials and methods
2
Literature search
2.1
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 guidelines (22). The protocol was prospectively registered on the International Prospective Register of Systematic Reviews (PROSPERO; registration number: CRD420251016970). A comprehensive search was performed in five electronic databases—PubMed, Embase, Scopus, Cochrane Library, and Web of Science—from their inception to March 1, 2025. The search strategy was developed based on the PICOS framework (Population, Intervention, Comparator, Outcomes, Study design) (23). Details of the search terms are presented in Supplementary material A. Within each PICOS component, keywords were combined using the Boolean operator “OR,” and the components were linked using “AND” to execute the final search.
Study selection
2.2
One investigator (W. J. Y.) independently removed duplicate records using EndNote 21 software. Subsequently, two investigators (W. J. Y. and W. X. W) independently screened the titles and abstracts of the retrieved studies based on the inclusion and exclusion criteria. Full texts were reviewed when eligibility could not be determined from the title and abstract. Any disagreements were resolved through discussion, and a third investigator (D. X. M.) was consulted when necessary.
Inclusion and exclusion criteria
2.3
The inclusion and exclusion criteria were established according to the PICOS framework. Inclusion criteria: (1) Population: Healthy individuals, including well-trained and recreational cyclists. Well-trained athletes were defined as having ≥3 years of systematic training, cycling ≥4–5 times per week, with a total weekly training volume of ≥8–10 h. Recreational cyclists were defined as having some cycling experience but training ≤3 times per week, with a total weekly training volume <6 h, and lacking long-term systematic competitive training experience (24–26). (2) Intervention: Caffeine ingestion prior to formal exercise, Forms of ingestion include solutions, tablets, mouthwash, and capsules. (3) Comparator: The same protocol as the intervention group, except that participants ingested a placebo instead of caffeine. (4) Outcomes: At least one cycling performance-related outcome, such as completion time, mean power output, mean heart rate, or ratings of perceived exertion (RPE).(5) Study design: Randomized controlled or crossover trial. Exclusion criteria: (1) Studies involving participants with clinical conditions; (2) Animal studies; (3) Qualitative studies, systematic reviews, meta-analyses, study protocols, preprints, and conference abstracts not peer-reviewed. (4) Excluded all anaerobic maximal sprint tests (e.g., Wingate tests).
Data extraction
2.4
Two investigators (W. J. Y. and W. X. W) independently extracted data, including bibliographic details, participant characteristics, caffeine dosage, and primary outcome measures. A third investigator (D. X. M.) checked the extracted data, and any disagreements were resolved by a fourth investigator (X. N. K.) through arbitration. If essential data were missing, the corresponding authors were contacted. Studies with unavailable data were excluded from the analysis.
Risk of bias assessment
2.5
Two investigators (W. J. Y. and D. X. M) independently assessed the risk of bias for each included study using the Cochrane Risk of Bias 2 (RoB 2) tool (27), evaluating the randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selective reporting. Disagreements were first discussed and, if unresolved, adjudicated by a third investigator (X. N. K.).
Outcome measures
2.6
Two investigators (W. J. Y. and D. X. M) independently extracted data from each study and cross-verified the information for consistency. Extracted data included: (1) Study characteristics: Author(s), publication year, and country; (2) Participant characteristics: Sample size, sex distribution, mean age with standard deviation, health status (healthy adults), and training level; (3) Intervention details: Caffeine dosage (mg or mg/kg), timing of ingestion relative to exercise, administration form (capsule, beverage), and placebo control; (4) Study design features: Study type, blinding status, and type of cycling task; (5) Primary outcomes: Cycling completion time (seconds or minutes), mean power output (watts), mean heart rate (bpm), and RPE score. Given potential heterogeneity across studies regarding participant characteristics and caffeine dosage, subgroup analyses were pre-specified: (1) Caffeine dosage: Low dose (≤3 mg/kg) vs. moderate dose (3–6 mg/kg) (28, 29); (2) Training level: Well-trained vs. recreational cyclists (24–26).
Certainty of evidence
2.7
The certainty of evidence was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system (30), which classifies evidence as high, moderate, low, or very low. Two investigators (W. J. Y. and D. X. M) independently performed the GRADE assessment.
Statistical analysis
2.8
All statistical analyses were conducted using R software (version 4.5.0), primarily relying on the metafor (31), clubSandwich (32), and puniform (33) packages for data processing and model construction. Based on the means, standard deviations, and sample sizes of the intervention and control groups, the standardized mean difference (SMD) was calculated as the effect size to evaluate the impact of acute caffeine ingestion on cycling performance. Effect sizes were interpreted as trivial (SMD < 0.20), small (0.20 ≤ SMD < 0.50), moderate (0.50 ≤ SMD < 0.80), or large (SMD ≥ 0.80) (34). To account for the nested structure of effect sizes within studies, a three-level random-effects model was constructed, with the study as level 3, individual effect sizes (id) as level 2, and residuals as level 1. The random-effects structure was specified as ~1|study/id (35, 36). Model parameters were estimated using the restricted maximum likelihood (REML) method (37), and robust variance estimation (RVE) was applied with the CR2 correction matrix from the clubSandwich package to adjust for small-sample bias, providing robust confidence intervals and significance tests (38, 39). Heterogeneity among studies was assessed using Cochran’s Q statistic, which evaluates the variability of the main effects across studies (40). I^2^ was also calculated to quantify heterogeneity, classified as low (I^2^ < 25%), moderate (25% ≤ I^2^ ≤ 50%), or high (I^2^ > 50%) (41). Statistical significance was set at p < 0.05. Effect size calculations were performed using the escalc function (31), and results were visualized with forest plots showing individual study effects and pooled estimates. Publication bias was assessed using funnel plots and Egger’s regression test (42, 43). To examine the robustness of pooled effect sizes, leave-one-out sensitivity analyses were conducted to evaluate the influence of individual studies (31). Considering potential variability in caffeine dosage, training status, and age among participants, subgroup analyses were performed by dosage and training level, and meta-regression analyses were conducted to explore the moderating effects of age on the intervention outcomes.
Results
3
Literature search results
3.1
A total of 2,359 records were identified through searches of PubMed (n = 441), Embase (n = 515), Scopus (n = 818), Cochrane Library (n = 318), and Web of Science (n = 267). Based on the predefined inclusion and exclusion criteria, 20 studies (44–63) were ultimately included in the meta-analysis. The study selection process is illustrated in Figure 1.
PRISMA flow diagram for study selection.
Characteristics of included studies
3.2
All 20 studies (44–63) employed randomized crossover trial designs, encompassing a total of 226 participants, of whom 207 (91.6%) were male. Individual study sample sizes ranged from 6 to 20 participants, with a mean age between 20 and 48 years. Among the participants, 134 were well-trained cyclists (59.3%), 82 were recreational cyclists with some training experience (36.3%), and one study (10 participants, 4.4%) did not report training status. The performance outcomes assessed across studies included cycling completion time, mean power output, mean heart rate, and ratings of perceived exertion (RPE). Additional details are provided in Table 1.
Risk of bias assessment
3.3
The risk of bias in the included trials was primarily concentrated in the randomization process, outcome measurement, and selective reporting domains, each potentially contributing to some degree of bias. Overall, the proportion of studies rated as low risk, some concerns, and high risk was 35, 40, and 25%, respectively. Detailed results are presented in Supplementary material C.
Meta-analysis results
3.4
Cycling completion time
3.4.1
Seventeen studies were included to examine the effect of caffeine ingestion on cycling completion time. Importantly, all 17 studies reported improvements in completion time following caffeine ingestion, consistently supporting its ergogenic benefit. The pooled effect size indicated that caffeine significantly reduced completion time (SMD = −0.36, 95% CI: −0.57 to −0.15, p < 0.01). Heterogeneity among studies was low, with no significant inconsistency observed (Q = 13.60, df = 19, p = 0.80, I^2^ = 0%).
Mean power output
3.4.2
Data from 14 studies were analyzed to assess the effect of caffeine on mean power output during cycling. The pooled results showed that caffeine significantly increased mean power output (SMD = 0.29, 95% CI: 0.05 to 0.52, p < 0.05). Heterogeneity was low (Q = 4.90, df = 16, p = 1.00, I^2^ = 0%).
Mean heart rate
3.4.3
Eleven studies were included to evaluate the effect of caffeine on mean heart rate during cycling. The pooled effect size was not statistically significant (SMD = 0.21, 95% CI: −0.06 to 0.48, p = 0.11). Heterogeneity was low, with good consistency among studies (Q = 10.99, df = 14, p = 0.69, I^2^ = 0%).
Ratings of perceived exertion (RPE)
3.4.4
Ten studies examined the effect of caffeine on subjective fatigue (RPE) during exercise. The pooled effect size indicated a slight reduction in RPE in the caffeine group compared with the control, but the difference was not statistically significant (SMD = −0.03, 95% CI: −0.30 to 0.24, p = 0.82). Heterogeneity was low (Q = 10.38, df = 14, p = 0.73, I^2^ = 0%).
Publication bias
3.5
To assess potential publication bias, Egger’s regression test was conducted for the four outcome measures. The results indicated potential publication bias for cycling completion time (p < 0.05), with the corresponding funnel plot shown in Figure 2. No significant publication bias was observed for mean power output (p = 0.12), mean heart rate (p = 0.41), or ratings of perceived exertion (RPE) (p = 0.80), with funnel plots also presented in Figure 3.
Meta-regression analysis of the effect of age on cycling performance.
Effects of caffeine ingestion on cycling performance: time, power, HR, and RPE. K, number of studies; N, sample size; SMD, standardized mean difference; REML, restricted maximum likelihood: CI, confidence interval; TIME, completion time; MPO, mean power output; HR, mean heart rate; RPE, ratings of perceived exertion.
Certainty of evidence
3.6
The certainty of evidence for the results of this systematic review is presented in Figure 3, with more detailed information available in Supplementary material E.
Sensitivity analysis
3.7
Leave-one-out sensitivity analyses demonstrated that exclusion of any single study did not alter the direction or statistical significance of the primary outcomes, indicating high robustness of the overall findings. Specifically: Completion time: SMD ranged from −0.33 to −0.45, all statistically significant (p < 0.01). Mean power output: β ranged from 0.22 to 0.30, approaching significance (p = 0.05–0.11). Mean heart rate: β ranged from 0.12 to 0.27, not significant (p > 0.11). RPE: β ranged from −0.04 to 0.08, not significant (p > 0.63).
Subgroup analyses
3.8
Caffeine dosage subgroup analysis (Table 2) revealed: Cycling completion time (TIME): Both ≤3 mg/kg (SMD = −0.42) and 4–6 mg/kg (SMD = −0.34) groups showed small reductions in completion time. Mean power output (MPO): 4–6 mg/kg group (SMD = 0.29) showed a small increase, whereas the ≤3 mg/kg group (SMD = 0.27) exhibited a smaller effect. Mean heart rate (HR): ≤3 mg/kg group (SMD = 0.41) showed a small increase, while the 4–6 mg/kg group (SMD = 0.07) exhibited a weaker effect. RPE: Both groups showed minimal effects (≤3 mg/kg: SMD = −0.06; 4–6 mg/kg: SMD = −0.004).
Training level subgroup analysis (Table 2) indicated: Completion time: Well-trained cyclists (SMD = −0.38) showed a small effect, slightly higher than recreational cyclists (SMD = −0.32). Mean power output (MPO): Both well-trained (SMD = 0.25) and recreational cyclists (SMD = 0.44) showed small improvements. Mean heart rate (HR): Both groups demonstrated small effects (well-trained: SMD = 0.21; recreational: SMD = 0.23). RPE: Effects were negligible (well-trained: SMD = 0.01; recreational: SMD = −0.15).
Meta-regression analysis
3.9
Meta-regression analyses indicated that age significantly moderated the effect of caffeine on cycling completion time (β = −0.0501, 95% CI: −0.09 to −0.01, p = 0.02), suggesting that the ergogenic effect of caffeine on completion time increases with age (Figure 2A). In contrast, age did not significantly moderate the effects of caffeine on mean power output, mean heart rate, or ratings of perceived exertion (RPE) (Figures 2B–D).
Discussion
4
Based on a systematic review and three-level mixed-effects meta-analysis, this study comprehensively examined the effects of acute caffeine ingestion on cycling performance, yielding the following main findings: acute caffeine intake significantly reduced cycling completion time and increased mean power output, indicating a clear ergogenic effect of caffeine on cycling performance. In contrast, caffeine had no significant impact on mean heart rate or ratings of perceived exertion (RPE). Importantly, the results also indicated a potential publication bias for cycling time-trial outcomes, suggesting that studies with null or unfavorable results may be underrepresented in the literature, which could lead to an overestimation of the true effect. Subgroup analyses further indicated that low-dose caffeine (≤3 mg/kg) produced a reduction in completion time that was comparable to, and may potentially be slightly greater than, the effect observed with moderate-to-high doses (4–6 mg/kg). Meta-regression analysis demonstrated that age significantly moderated the effect on completion time, with older athletes deriving greater benefits from caffeine ingestion.
Compared with the recent meta-analysis by Chen et al. (21), our findings show both consistency and notable differences. Similar to Chen et al. (21), we observed a significant ergogenic effect of caffeine on cycling time-trial performance and mean power output. However, in contrast to their report—where moderate doses (4–6 mg/kg) produced significant improvements and low doses (1–3 mg/kg) showed no clear effect—our results demonstrated significant benefits across all included studies, with both low and moderate doses producing small but meaningful reductions in completion time. Additionally, Chen et al. found no moderating effect of age, whereas our meta-regression indicated that older athletes may derive greater performance benefits. The observed improvements in completion time and power output further support caffeine’s ergogenic effects, and the low heterogeneity across included studies strengthens the reliability of these findings. The lack of significant effects on heart rate and RPE suggests that caffeine primarily enhances exercise efficiency and neuromuscular function, rather than directly affecting cardiovascular responses or subjective fatigue perception, which aligns with earlier reports (5–7).
Dose–response subgroup analyses indicated that low-dose caffeine may provide slightly superior reductions in completion time compared to moderate-to-high doses, supporting the notion that low doses can still elicit meaningful performance benefits (64, 65). Lower doses also minimize the risk of adverse effects and enhance long-term applicability, which has practical implications for athletic performance. Subgroup analyses based on training status showed that both well-trained and recreational cyclists benefited from caffeine supplementation, with slightly greater effects observed in well-trained athletes, suggesting that training level may modulate supplement efficacy.
The significant moderating effect of age is particularly noteworthy. Meta-regression results suggest that the ergogenic effect of caffeine on cycling completion time increases with age, possibly due to age-related declines in neuromuscular function, differences in caffeine metabolism, or heightened sensitivity. It is also possible that older participants in the included studies had longer training histories and higher fitness levels, contributing to greater benefits (66). These findings highlight the importance of considering individual age when designing nutrition supplementation strategies to achieve personalized, optimized interventions.
Strengths of this study include the inclusion of a substantial number of high-quality randomized crossover trials, the use of a three-level random-effects model to account for dependent effect sizes, which enhances statistical power and result robustness, and the detailed exploration of dose, training status, and age as moderating factors through subgroup and meta-regression analyses, providing deeper insights into the mechanisms underlying caffeine’s ergogenic effects.
However, several limitations should be acknowledged. First, the sample sizes in the included studies were relatively small, particularly for some subgroups and regression analyses, limiting statistical power. Future large-scale, high-quality trials are needed to confirm these findings. Second, factors such as caffeine administration form (capsules vs. beverages), exercise task type, and participants’ habitual caffeine intake were not fully controlled, potentially influencing outcomes. Additionally, most studies focused on short-duration, high-intensity cycling, so future research should extend to different endurance modalities and longer-duration performance assessments.
Nonetheless, this study still has several limitations. First, although the inclusion and exclusion criteria were defined according to the PICOS framework to ensure the specificity and focus of the research question, they may also introduce a certain degree of selection bias. For example, the exclusion of studies conducted under special experimental conditions—such as hypoxia, heat exposure, low-glycogen states, time-to-exhaustion (TTE) tests, and Wingate anaerobic sprint protocols—as well as studies involving combined supplementation protocols, may limit the generalizability of our findings to more complex or varied exercise contexts. Second, the overall sample size of the included studies remains relatively small, and the statistical power of certain subgroup analyses and multilevel meta-regression models may therefore be constrained. Moreover, 91.6% of the total sample (207 out of 226 participants) consisted of male cyclists, and no studies exclusively examined female cyclists. As a result, the results derived from the statistical analyses are more appropriately applied to male populations, and caution is required when attempting to generalize these findings to female cyclists. Third, variations in caffeine administration forms (e.g., capsules, beverages, mouth rinse), exercise task characteristics, and participants’ habitual caffeine intake were not fully controlled across studies, which may introduce additional heterogeneity into the results (67). Furthermore, most existing studies have focused on short-duration, high-intensity, or time-trial cycling tasks. Future research should extend to different endurance modalities, longer exercise durations, and populations with varied training backgrounds to more comprehensively assess the acute effects of caffeine.
Future investigations should integrate additional physiological markers and explore the mechanisms and individual variability in caffeine response, including genetic and sex-related differences, to facilitate the development of personalized supplementation strategies (11, 12). In practice, caffeine intake should be tailored based on athlete age, training status, and dose–response characteristics to maximize performance benefits while minimizing risk.
Conclusion
5
Caffeine ingestion significantly reduces cycling completion time and enhances mean power output, demonstrating its clear ergogenic effect on cycling performance. At the same time, current evidence shows that caffeine ingestion does not produce significant effects on heart rate or ratings of perceived exertion (RPE). Subgroup analysis showed that the ergogenic effect of low-dose caffeine was comparable to that of higher doses, indicating that lower doses can achieve comparable performance enhancement. Both well-trained and recreational athletes showed similar responses across outcome measures. Age was identified as an important moderator, with older athletes experiencing greater improvements in performance. Compared with previous studies, this review incorporated more high-quality trials and employed a three-level meta-analytic approach, enhancing the robustness and interpretability of the findings. Based on these results, it is recommended that athletes and coaches design caffeine supplementation strategies considering individual differences, including age, training status, and dietary habits, to optimize exercise performance outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Beck KL Thomson JS Swift RJ Von Hurst PR. Role of nutrition in performance enhancement and postexercise recovery. Open Access J Sports Med. (2015):259–67.26316828 10.2147/OAJSM.S 33605 PMC 4540168 · doi ↗ · pubmed ↗
- 2Peeling P Castell LM Derave W de Hon O Burke LM. Sports foods and dietary supplements for optimal function and performance enhancement in track-and-field athletes. Int J Sport Nutr Exerc Metab. (2019) 29:198–209. doi: 10.1123/ijsnem.2018-0271, 30299192 · doi ↗ · pubmed ↗
- 3Burke LM. Caffeine and sports performance. Appl Physiol Nutr Metab. (2008) 33:1319–34. doi: 10.1139/H 08-130, 19088794 · doi ↗ · pubmed ↗
- 4Guest NS Van Dusseldorp TA Nelson MT Grgic J Schoenfeld BJ Jenkins ND . International society of sports nutrition position stand: caffeine and exercise performance. J Int Soc Sports Nutr. (2021) 18:1. doi: 10.1186/s 12970-020-00383-4, 33388079 PMC 7777221 · doi ↗ · pubmed ↗
- 5Davis J-K Green JM. Caffeine and anaerobic performance: ergogenic value and mechanisms of action. Sports Med. (2009) 39:813–32. doi: 10.2165/11317770-000000000-00000, 19757860 · doi ↗ · pubmed ↗
- 6Davis JM Zhao Z Stock HS Mehl KA Buggy J Hand GA. Central nervous system effects of caffeine and adenosine on fatigue. Am J Physiol Regul Integr Comp Physiol. (2003) 284. doi: 10.1152/ajpregu.00386.2002, 12399249 · doi ↗ · pubmed ↗
- 7Jones G. Caffeine and other sympathomimetic stimulants: modes of action and effects on sports performance. Essays Biochem. (2008) 44:109–24.18384286 10.1042/BSE 0440109 · doi ↗ · pubmed ↗
- 8Ganio MS Klau JF Casa DJ Armstrong LE Maresh CM. Effect of caffeine on sport-specific endurance performance: a systematic review. J Strength Cond Res. (2009) 23:315–24. doi: 10.1519/JSC.0b 013e 31818 b 979a, 19077738 · doi ↗ · pubmed ↗