An Unusual Presentation of an Epidermoid Cyst Near the Nasolabial Fold: A Case Report
Abira Chattopadhyay, Md Arif Hossain, Aritra Chatterjee, Nayana De, Basabdatta Ghosh

TL;DR
A 31-year-old man had a rare epidermoid cyst near his nose-lip fold, which was successfully removed with no recurrence after a year.
Contribution
This case report presents an unusual location for an epidermoid cyst and demonstrates the effectiveness of an intraoral surgical approach.
Findings
The lesion was confirmed as an epidermoid cyst through histopathology.
The intraoral approach provided good aesthetic and functional outcomes with no recurrence.
The case emphasizes the need to consider epidermoid cysts in cheek mass diagnoses.
Abstract
Epidermoid cysts are benign, slow-growing lesions arising from epidermal cell proliferation within the dermis. Although common on the scalp and trunk, they rarely occur in the head and neck region, particularly the cheek. We report a 31-year-old male with a painless, progressive swelling lateral to the right nasolabial fold for two years. Ultrasonography and fine-needle aspiration yielded keratinous material suggestive of an epidermoid cyst. The lesion was excised entirely via an intraoral approach under general anesthesia. Histopathology showed a cyst lined by orthokeratinized stratified squamous epithelium without adnexal structures, confirming an epidermoid cyst. Healing was uneventful, and no recurrence was noted after one year. This case highlights the importance of considering epidermoid cysts in the differential diagnosis of cheek masses and demonstrates that an intraoral…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3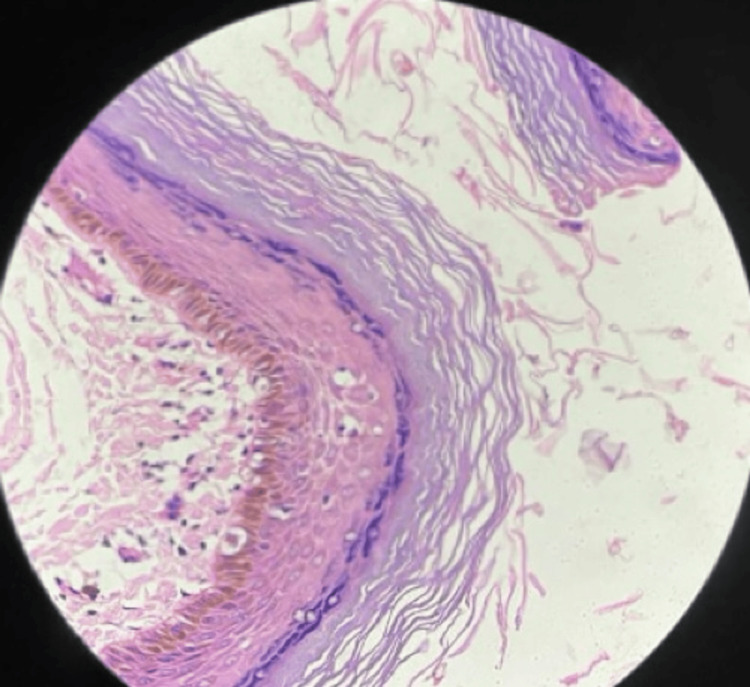 Figure 4
Figure 4 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTeratomas and Epidermoid Cysts · Head and Neck Anomalies · Cancer and Skin Lesions
Introduction
Epidermoid cysts, also termed epidermal inclusion or infundibular cysts, are benign developmental lesions resulting from the proliferation of epidermal cells within the dermis [1]. They account for approximately seven percent of cysts in the head and neck region, with only about 1.6% presenting intraorally [1-3]. These cysts may be congenital, due to ectodermal entrapment during embryonic fusion, or acquired following trauma or surgery [4,5].
In the oral and maxillofacial region, dermoid and epidermoid cysts typically occur along midline structures such as the floor of the mouth. Localization to areas such as the cheek or the nasolabial fold is considerably less common, likely due to the absence of embryologic fusion planes that predispose to congenital cyst formation [2,5]. Most cases are diagnosed in young or middle-aged adults, and many lesions remain unnoticed until they reach a cosmetically or functionally significant size. The differential diagnosis includes dermoid cyst, lipoma, nasolabial (Klestadt’s) cyst, and schwannoma, which should be excluded based on imaging, cytology, and histology [2,3]. When evaluating cheek swellings, differential diagnoses include dermoid cysts, lipomas, schwannomas, and nasolabial cysts.
In the head and neck region, the submental and submandibular spaces and the floor of the mouth are most commonly affected, whereas cheek or nasolabial presentations are rare [2,5]. Accurate assessment and preservation of facial soft-tissue contours are particularly important in aesthetically sensitive regions such as the nasolabial fold. Advances in three-dimensional imaging have significantly improved the evaluation of facial soft-tissue changes [6,7]. This report presents an uncommon epidermoid cyst near the nasolabial fold, successfully managed via an intraoral approach, emphasizing diagnostic considerations and aesthetic outcomes [1-5].
Case presentation
A 31-year-old male presented to the Department of Oral and Maxillofacial Surgery with a painless, gradually enlarging swelling on the right cheek near the nasolabial fold, present for two years (Figure 1). There was no history of trauma, infection, or discharge, and the patient reported cosmetic concern and mild discomfort while smiling.
Preoperative clinical photograph.Distinct oval swelling lateral to the right nasolabial fold
On extraoral examination, the swelling was oval, firm, mobile, and non-tender, measuring approximately 4 × 3 cm. The overlying skin was normal in colour and texture. Intraoral mucosa appeared normal. Orthopantomogram (OPG) revealed no bony involvement (Figure 2). Ultrasonography demonstrated a well-defined, heterogeneously hyperechoic subcutaneous lesion with minimal internal vascularity, and fine-needle aspiration produced thick keratinous material containing anucleate squames-findings consistent with an epidermoid or dermoid cyst.
Preoperative orthopantomogram.Orthopantomogram with specifications of 12.70 seconds, 74.00 kV and 6.00 mA showing soft-tissue shadow over the right canine-premolar region without bony changes.
The intraoral approach was preferred as it allows satisfactory exposure of the lesion while avoiding external scarring, thereby ensuring a better cosmetic outcome. An intraoral vestibular incision was placed under general anesthesia in the right maxillary buccal sulcus below the parotid duct orifice (Figure 3A). Careful, sharp, and blunt dissection permitted enucleation of the cyst in toto (Figure 3B). Accidental puncture released thick, cheese-like keratinous debris; the cavity was irrigated with saline and closed with 3-0 vicryl sutures. The specimen was sent for histopathological examination (Figure 3C).
Intraoral approach for cyst excision via the right maxillary buccal sulcus.(A) Placement of incision extending from anterior (A) to posterior (P) region in the right maxillary buccal sulcus. (B) Dissection and enucleation of the cystic lesion through the intraoral approach. (C) Excised cystic specimen measuring approximately 3 × 2 cm.
Microscopy revealed a cystic lumen lined by orthokeratinized stratified squamous epithelium lacking adnexal structures, and a lumen filled with laminated keratin debris, confirming an epidermoid cyst (Figure 4).
Histopathological findings confirming epidermoid cyst.Photomicrograph showing a cystic cavity lined by orthokeratinized stratified squamous epithelium without adnexal structures and a lumen filled with laminated keratin debris (H&E stain, 40×).
Postoperative recovery was uneventful. Because the approach was intraoral, there was no visible facial scar. At one-year follow-up, the patient remained asymptomatic with no recurrence (Figure 5).
Postoperative images after one year.(A) Frontal, (B) Lateral, (C) Basal, and (D) Superior views showing symmetrical facial contour and complete healing with no visible scar or recurrence one year after intraoral excision of the epidermoid cyst.
Discussion
Epidermoid cysts account for only a small fraction of cystic lesions in the head and neck region and are infrequently encountered in the cheek or nasolabial area [1-3]. They are histologically classified as epidermoid (lined by squamous epithelium only), dermoid (epithelium plus adnexal structures), or teratoid (elements from multiple germ layers) [5,8].
Their origin may be congenitally caused by ectodermal entrapment during embryogenesis, or acquired via implantation of epidermal elements after trauma or surgery [4,9,10]. Clinically, epidermoid cysts present as slow-growing, well-circumscribed, painless masses with intact overlying skin; the absence of a punctum may render diagnosis challenging. Ultrasonography and fine-needle aspiration cytology are helpful preliminary investigations for superficial lesions, while CT or MRI may be needed for deep or atypical presentations [1]. Definitive diagnosis rests on histopathology [2].
The differential diagnosis includes dermoid cyst, lipoma, nasolabial (Klestadt’s) cyst, and schwannoma, which should be excluded based on imaging, cytology, and histology [2,3]. When evaluating cheek swellings, differential diagnoses include dermoid cysts, lipomas, schwannomas, and nasolabial cysts. Complete surgical excision is the treatment of choice, and recurrence is uncommon when the excision is thorough [11]. While extraoral access is conventional for cheek lesions, the intraoral approach offers cosmetic superiority for nasolabial or midfacial cysts by avoiding visible scars and preserving aesthetics [2,11]. Although benign, epidermoid cysts have been reported to undergo malignant transformation into squamous cell carcinoma, basal cell carcinoma, or Merkel cell carcinoma in rare cases [11]. The incidence of malignant change from an epidermal cyst to cutaneous squamous cell carcinoma is 0.011-0.045% [12]
The cheek is an uncommon location because it does not correspond to a recognized embryologic fusion line, unlike the midline structures of the oral cavity [13]. Nasolabial cysts in particular may resemble epidermoid cysts but usually occur more superficially and contain mucous rather than keratinous material [14]. Recognition of these distinctions is paramount in devising an appropriate treatment plan.
Conclusions
Epidermoid cysts of the cheek are rare and can clinically mimic other benign soft-tissue swellings. A systematic clinical assessment, supported by imaging and confirmed by histopathology, ensures accurate diagnosis and management. When anatomically feasible, intraoral excision provides effective, scar-free removal with excellent cosmetic and functional outcomes and minimal recurrence risk. Although this report describes a single case, it highlights an uncommon clinical presentation and underscores the need for larger case series with longer follow-up to better define optimal management and outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Overview of epidermoid cyst Eur J Radiol Open Hoang VT Trinh CT Nguyen CH Chansomphou V Chansomphou V Tran TT 291301620193151691610.1016/j.ejro.2019.08.003PMC 6732711 · doi ↗ · pubmed ↗
- 2Epidermoid cyst of submandibular region J Oral Maxillofac Pathol Janarthanam J Mahadevan S 4354371620122324848210.4103/0973-029X.102511 PMC 3519225 · doi ↗ · pubmed ↗
- 3Epidermoid cyst arising in the buccal mucosa: case report and literature review Acta Stomatol Croat Costa FW Carvalho FS Chaves FN 2963044820142768837910.15644/asc 48/4/8PMC 4872814 · doi ↗ · pubmed ↗
- 4Epidermoid cyst of the buccal mucosa-An uncommon entity: case report and literature review Clin Case Rep Dammak N Chokri A Slim A 09202110.1002/ccr 3.4853 PMC 845595934584716 · doi ↗ · pubmed ↗
- 5Epidermoid cysts in head and neck: our experiences, with review of literature Indian J Otolaryngol Head Neck Surg Dutta M Saha J Biswas G Chattopadhyay S Sen I Sinha R 14216520132442760910.1007/s 12070-011-0363-y PMC 3718960 · doi ↗ · pubmed ↗
- 6Three-dimensional assessment of facial soft-tissue asymmetry before and after orthognathic surgery Br J Oral Maxillofac Surg Hajeer MY Ayoub AF Millett DT 3964044220041533676410.1016/j.bjoms.2004.05.006 · doi ↗ · pubmed ↗
- 7A new three-dimensional method of assessing facial volumetric changes after orthognathic treatment Cleft Palate Craniofac J Hajeer MY Mao Z Millett DT Ayoub AF Siebert JP 1131204220051574810110.1597/03-132.1 · doi ↗ · pubmed ↗
- 8Cysts of the Oral and Maxillofacial Regions Shear M Speight MP 291295 Hoboken, New Jersey Wiley-Blackwell 2022 https://onlinelibrary.wiley.com/doi/book/10.1002/9780470759769?utm_medium=article&utm_source=researchgate.net