A case of necrotizing pneumonia leading to respiratory failure and tracheostomy
Nurul 'Aifaa Mohd Azmi, Shao Keong Koeh, Tuan Sharifah Syuwaibah Tuan Zainal, Mohd Zulfakar Mazlan

TL;DR
A 58-year-old woman with necrotizing pneumonia required tracheostomy and intensive care, highlighting the disease's severity and lack of targeted treatments.
Contribution
This case report highlights the challenges in managing necrotizing pneumonia and emphasizes the need for supportive care in critical cases.
Findings
Necrotizing pneumonia can lead to respiratory failure requiring tracheostomy.
Treatment with carbapenem, oxazolidinone, and corticosteroid led to recovery.
Current management focuses on supportive care due to lack of specific anti-inflammatory treatments.
Abstract
Necrotizing pneumonia is a severe lung infection characterized by pulmonary necrosis and high mortality rates of up to 50 %. It is typically caused by toxin-producing pathogens, such as Staphylococcus aureus and Klebsiella pneumoniae. Limited guidelines exist for its management, making its treatment challenging. Case report: We discuss a case of a 58-year-old Malay woman with no significant comorbidity but developed necrotizing pneumonia. The diagnosis was confirmed using computed tomography (CT) of the thorax. Treatment with carbapenem, oxazolidinone and corticosteroid led to significant recovery. Conclusion: To date, no specific anti-inflammatory treatments exist for severe necrotizing pneumonia. Since systemic inflammation and multi-organ failure drive mortality, management focuses on supportive care aimed at maintaining oxygenation and hemodynamic stability to improve outcomes in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
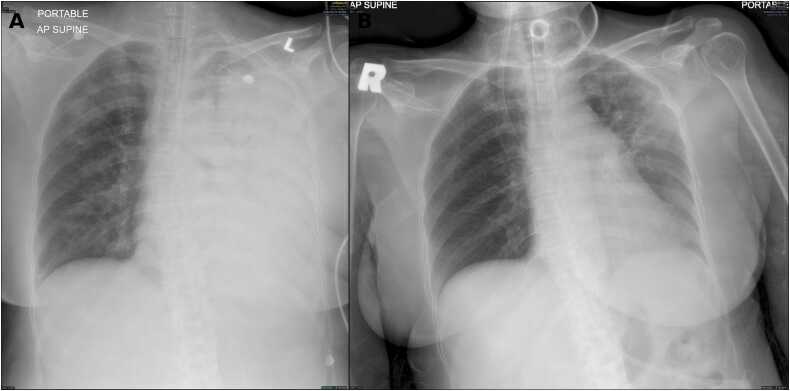 Figure 1
Figure 1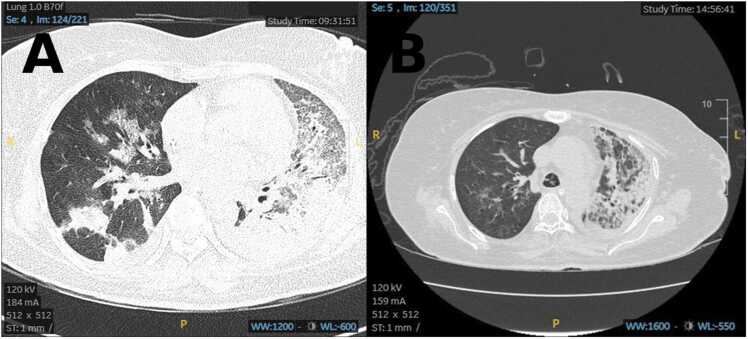 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNosocomial Infections in ICU · Pneumonia and Respiratory Infections · Pleural and Pulmonary Diseases
Introduction
Necrotizing pneumonia is a life-threatening form of severe pneumonia characterized by pulmonary necrosis and often associated with severe sepsis. Necrotizing pneumonia has a reported incidence of 1 % of pneumonia with a mortality rate of up to 50 % [1]. The causative organisms are usually toxin-producing, such as Staphylococcus aureus, Streptococcus pneumoniae, and Klebsiella pneumoniae. To date, there are limited guidelines for the management of necrotizing pneumonia, and its treatment is mainly based on severe pneumonia treatment. The postulated pathogenesis is severe lung parenchymal infection triggering a systemic inflammatory response, leading to tissue necrosis and liquefaction of infected tissue. Its complications are pulmonary tissue destruction, thrombus formation, and empyema.
Case report
A 58-year-old Malay woman with a history of well-controlled childhood asthma, working as a schoolteacher, presented to the emergency department with a 5-day history of fever, chills, rigor, and productive cough. She had no known history of COVID-19 infection. On day 2 of her illness, she visited an outpatient clinic where hypotension was noted, but she declined hospital admission. Her condition subsequently worsened with increasing breathlessness, prompting presentation to our facility.
On arrival, she was conscious but tachypneic with a respiratory rate of 39 breaths per minute and oxygen saturation of 83 % on room air. Her blood pressure was 120/56 mmHg, and heart rate was 115 beats per minute. Physical examination revealed lethargy, fever, and coarse crepitations over the left lung; other systemic examinations were unremarkable. SARS-CoV-2 polymerase chain reaction testing performed on admission was negative. Arterial blood gas analysis showed severe hypoxic respiratory failure with lactic acidosis. Laboratory investigations revealed hemoglobin 14.6 g/dL, white cell count 8.7 × 10^9/L (neutrophils 91 %, lymphocytes 7.6 %), and platelets 168 × 10^9/L. Initial chest radiograph demonstrated heterogeneous opacities in the left lower and upper lung fields and right perihilar region (Fig. 1(a)). Electrocardiogram was unremarkable.Fig. 1. Portable anteroposterior chest radiographs obtained during hospitalisation. (a) Chest radiograph on Day 3 of admission demonstrating near-complete opacification of the left hemithorax. (b) Chest radiograph on Day 50 showing marked interval radiographic improvement with re-expansion of the left lung.Fig. 1
She was diagnosed with severe pneumonia and started on high-flow nasal cannula oxygen therapy (fraction of inspired oxygen (FiO_2_) 0.9, 60 L/min) and fluid resuscitation (20 mL/kg over 2 h). Empiric intravenous antibiotics included intravenous ceftazidime 2 g stat and azithromycin 500 mg once daily. Blood cultures were obtained. Despite treatment, repeated arterial blood gases showed persistent hypoxia with a partial pressure of oxygen in arterial blood (PaO_2_)/FiO_2_ ratio (P/F) of 58. Due to respiratory distress and failure to improve on high-flow oxygen, she was intubated. Intubation was uneventful, but ventilation was difficult, with a P/F ratio of 100 and a downward trend in blood pressure requiring norepinephrine infusion. She was admitted to the intensive care unit (ICU).
In the ICU, she required high ventilator support, with a P/F ratio improving to 160. Repeat chest X-ray on day 2 admission showed worsening and persistent pneumonic infiltrates on the left lung (Fig. 1(b)). Antibiotics were escalated to intravenous levofloxacin and cloxacillin to cover possible Staphylococcus infection. Bronchoscopy on days 2 and 3 revealed minimal mucus plugs and mucosal erythema; bronchial alveolar lavage cultures were negative. Nasal swabs for respiratory viral panels were also negative. Given chest radiographs showed progressive consolidation in the left lung, prompting contrast-enhanced CT thorax on day 4 of illness, which demonstrated severe necrotizing pneumonia with radiological features suggestive of secondary organizing pneumonia and acute respiratory distress syndrome changes in the left upper and lower lobes (Fig. 2(a)).Fig. 2. Axial computed tomography images of the thorax obtained during hospitalisation. (A) CT scan on Day 5 of admission demonstrating extensive bilateral parenchymal opacities with predominant left-sided involvement. (B) CT scan on Day 26 showing interval radiological improvement with partial resolution of parenchymal changes.Fig. 2
During this period, blood investigations reflected a severe systemic inflammatory response with involvement of multiple organ systems, including markedly raised inflammatory markers (peak C-reactive protein 550 mg/L and procalcitonin 17.51 ng/mL), worsening acute kidney injury with serum creatinine rising to 325 µmol/L, and deranged liver biochemistry with elevated bilirubin and alkaline phosphatase levels (Table 1, Table 2).Table 1. Timeline of clinical events during hospitalisation. Chronological summary of major clinical events and interventions during the course of illness and hospitalisation.Table 1Day of Admission****Event SummaryDay −5Onset of fever, chills, rigor, productive coughDay −2Outpatient visit: hypotension noted; patient declined admissionDay 0 (Admission)Presented to Emergency Department (ED) with severe respiratory distress; diagnosed with severe pneumonia; started High Flow Nasal Canula (HFNC) oxygen and IV antibiotics (ceftazidime, azithromycin); blood cultures taken; intubated due to worsening hypoxia and respiratory failure; admitted to Intensive Care Unit (ICU)Day 1–2Bronchoscopy performed; minimal mucus plugs; lavage bacterial cultures negative; respiratory viral panel negative. Antibiotics were escalated to intravenous levofloxacin and cloxacillin to cover possible Staphylococcus infection.Day 4CT thorax showed severe necrotizing pneumonia with radiological features suggestive of organizing pneumoniaDay 10Repeat bronchoscopy and cultures negative; deterioration notedDay 10–19IV dexamethasone 6 mg daily administeredDay 10–23Antibiotics escalated to IV linezolid and meropenemDay 21Tracheostomy performed due to prolonged ventilationDay 24Repeat in-hospital CT thorax showed resolution of necrotizing pneumoniaDay 32Successfully weaned off mechanical ventilationDay 40Transfer to medical HDU wardDay 43Blood culture grew Klebsiella Pneumonia and Enterococcus FaeciumDay 57Discharge homeTable 2Serial laboratory investigations during hospitalisation. Serial laboratory investigations recorded during hospitalisation, demonstrating changes in haematological, inflammatory, renal, and liver parameters over time.Table 2A Haematological parametersDayWCCPLTHb****HCTDay 110.7910111.234.6Day 215.0210511.736.3Day 313.989510.833.2Day 512.0421410.330.5Day 814.813559.929.9Day 109.724137.221.8Day 1510.7936610.230.4Day 259.1516610.030.9Day 4511.33218.426.1B Inflammatory markersDayCRPPCTDay 1550—Day 2471—Day 3—17.51Day 5——Day 8——Day 101405.99Day 1566.4—Day 2528.7—Day 453.78—C Renal functionDayUreaCreatinineDay 112.1133Day 214.6150Day 317.8165Day 533.3262Day 833.8246Day 1031.2293Day 1527.5325Day 2519.3129Day 4512.052D Liver functionDayALTASTALPTB****ALBDay 1791311943321Day 2801362123424Day 3681202465125Day 5721262725029Day 853572765224Day 1042593213422Day 1537585691225Day 252328362930Day 452122161433Abbreviations: WCC, white cell count; PLT, platelet count; Hb, haemoglobin; HCT, haematocrit; CRP, C-reactive protein; PCT, procalcitonin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; ALP, alkaline phosphatase; TB, total bilirubin; ALB, albumin. Missing values indicate tests not performed on that day.
Due to clinical deterioration and worsening chest x-ray, bronchoscopy was repeated on day 10; cultures and polymerase chain reaction (PCR) for bacterial and viral pathogens remained negative. She received intravenous dexamethasone 6 mg daily for 10 days and antibiotic escalation to intravenous linezolid 600 mg twice daily and meropenem 1 g three times daily for two weeks. Subsequently, ventilator support gradually weaned pressure support by day 20. However, renal function worsened during ICU stay, necessitating regular dialysis (Table 2).
Given prolonged ventilation, tracheostomy was performed on day 21. Repeat in-hospital CT thorax was performed on day 24 (Fig. 2(b)) after completing antibiotics, showed resolution of necrotizing pneumonia. She was successfully liberated from mechanical ventilation by day 32 and transferred to the high dependency unit (HDU) on day 40 with tracheostomy oxygen mask at 15 L/min and discharged home on day 50 with marked improvement on chest radiograph (Fig. 1(b)). In HDU, her blood culture grew Klebsiella pneumoniae and Enterococcus faecium which is sensitive to cefuroxime and vancomycin and treated with those antibiotics prior to discharge.
Discussion
Necrotizing pneumonia is a rare yet life-threatening spectrum of severe pneumonia. This diagnosis is rather unexpected in this patient, considering her healthy premorbid function as a teacher with no significant comorbidity. Commonly quoted risk factors include alcohol use, and diabetes mellitus [1]. However, none of these risk factors were present in our patient upon presentation. β-lactams and macrolides were initially prescribed in accordance with international guidelines in the treatment of severe pneumonia [2], [3]. Its poor clinical and radiographic response despite antibiotic and bronchoscopic lavage leads to suspicion of malignancy, interstitial lung disease, and lung abscess as differential diagnoses. CT of the thorax was subsequently done on day 4 of illness and unveiled this rather unexpected diagnosis of necrotizing pneumonia. CT thorax imaging typically reveals disruption of the normal lung structure accompanied by areas of reduced contrast uptake in the lung tissue, indicating liquefactive necrosis [1], [4]. These findings reflect impaired perfusion and tissue destruction characteristic of necrotizing pneumonia. Chest X-ray imaging was insufficient to confirm necrotizing pneumonia due to its low sensitivity and specificity [1].
β-lactams and macrolides are first-line treatments as recommended by the latest guidelines to empirically treat Streptococcus pneumoniae, Klebsiella pneumoniae, Staphylococcus, and atypical organisms [2]. The CT thorax findings and poor clinical response during the first week of treatment raised suspicion of poor response with the levofloxacin and cloxacillin. Although no microbiological isolation of methicillin-resistant Staphylococcus aureus (MRSA) was identified, the radiological pattern of bilateral cavitating and necrotizing infiltrates, together with the lack of clinical response to levofloxacin and subsequent marked clinical, biochemical, and radiographic improvement following initiation of linezolid, strongly suggests MRSA as the most likely causative pathogen. Resistance to fluoroquinolones is well described in MRSA pneumonia, making poor response to levofloxacin plausible. Intravenous meropenem and linezolid were therefore empirically started in this patient for two weeks.
Following that, she had significant clinical, biochemical, and radiographic improvement. Linezolid was chosen over vancomycin for two reasons: it is effective at neutralizing toxin [5], [6], [7] produced by MRSA and does not require regular therapeutic monitoring (TDM) [8], especially vital since the patient had acute renal failure requiring dialysis.
To date, there is no optimal duration of antibiotic treatment recommended for severe necrotizing pneumonia [4]. However, C-reactive protein (CRP) and procalcitonin (PCT) are often recommended to guide antibiotic duration [9], [10], [11]. As for this patient, her CRP and point of care PCT were decreased after 2 weeks of meropenem and linezolid. Thus, we decided to stop antibiotics in view of the good clinical and biochemical response. Although PCT couldn't discriminate between viral and bacterial infection, the higher titer suggests an increased likelihood of bacterial pneumonia. Furthermore, PCT is well studied to guide the duration of antibiotics [12], [13], potentially shortening the antibiotic course, especially in such patients with life-threatening necrotizing pneumonia. Studies show antibiotic duration guided by PCT associated with a reduction of 1–2 days of treatment [10], [11], [14]. In contrast, Klebsiella pneumoniae isolated later in the clinical course was most consistent with a secondary nosocomial infection, likely related to prolonged intensive care unit stay and invasive devices, rather than the primary cause of the initial severe necrotizing pneumonia.
Radiological features suggestive of secondary organizing pneumonia were noted on her contrast-enhanced CT thorax. Histopathologically, organizing pneumonia is characterized by patchy filling of the alveoli and bronchioles with plugs of granulation tissue [15]. On CT imaging, it most commonly appears as bibasal, peribronchovascular, and/or peripheral areas of consolidation [16]. However, these radiological features may overlap with changes seen in the acute phase of severe pneumonia, and a definitive diagnosis requires histopathological confirmation or interval follow-up imaging [15]. In this patient, tissue biopsy was not performed as she responded well to broad-spectrum antibiotics and corticosteroid treatment, and follow-up CT imaging at 3–6 months after discharge was not available as the patient did not return for follow-up.
Corticosteroid treatment remains controversial. The Dexamethasone for the acute respiratory distress syndrome (DEXA-ARDS) trial (2020) demonstrated that early administration of dexamethasone significantly reduced the duration of mechanical ventilation and ICU mortality in patients with moderate to severe ARDS [17]. In contrast, the Early Steroid Administration in Community-Acquired Pneumonia with High Inflammatory Response (ESCAPE) trial, which involved 586 patients, found no difference in ICU mortality when using methylprednisolone at 0.75 mg/kg/day for 10 days [18].
Our center used IV dexamethasone 6 mg OD for 10 days for this patient after weighing the risk of immunosuppression, potential secondary infection, and previous experience in treating COVID-related organizing pneumonia. This dose regimen is also like the Randomised Evaluation of COVID-19 Therapy (RECOVERY) trial, which used IV dexamethasone in COVID-19 pneumonia [19]. Given the apparent clinical response to corticosteroid therapy, systemic vasculitis was also considered as a differential diagnosis. However, the absence of extrapulmonary manifestations, normal renal parameters and urinalysis, and sustained clinical recovery without relapse on follow-up make active systemic vasculitis unlikely in this patient.
The patient showed excellent clinical and biochemical improvement following broad-spectrum empirical antibiotics and a short course of intravenous dexamethasone. At follow-up reviews at 3 and 6 months after discharge, she remained clinically well with no constitutional symptoms, skin lesions, haematuria, neurological deficits, or other features suggestive of systemic vasculitis. Therefore, it is important to adhere to pneumonia guidelines to improve patient outcomes [20]. Early surgical referrals are paramount for the timely detection and management of complications such as empyema and bronchopleural fistula [21].
Conclusion
This case highlights the rarity and complexity of severe necrotizing pneumonia in a patient without clear predisposing risk factors. Radiological features suggestive of organizing pneumonia were observed during the disease course; however, these findings should be interpreted with caution given the overlap with acute and subacute pneumonia. Accurate assessment using advanced imaging such as CT thorax remains vital in guiding management. Tailored empirical antibiotic therapy, guided by biomarkers including C-reactive protein and procalcitonin, together with judicious use of corticosteroids, contributed to a favourable clinical and radiological outcome. Further studies are needed to better define optimal antimicrobial strategies, treatment duration, and the role of corticosteroids in severe necrotizing pneumonia.
Author contributions
ZF, KH, SS, and FA contributed to the analysis and interpretation of the patient data for this case and played major roles in drafting the manuscript. They were also involved in the conception of the study and in critically revising the manuscript. All authors reviewed and approved the final version of the manuscript.
Declarations
Ethics approval and consent to participate are not applicable.
CRediT authorship contribution statement
Shao Keong Koeh: Writing – original draft. Mohd Azmi Nurul 'aifaa: Writing – review & editing, Supervision, Resources. Mohd Zulfakar Mazlan: Writing – review & editing, Visualization, Supervision, Methodology, Formal analysis, Data curation, Conceptualization. Tuan Sharifah Syuwaibah Tuan Zainal: Writing – review & editing.
Consent
Written informed consent was obtained from the next of kin for publication of this case report and accompanying images during ICU admission. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Consent for publication
Consent for publication was not required because the study did not involve any identifiable or personal data.
Ethical approval
Not required for Case report in my institution.
Funding
This work was supported by 10.13039/501100004595Universiti Sains Malaysia external grant R504‑LR‑GAL008‑0006150268‑N109 and short-term grant R501-LR-RND002-0000001210-0000.
Declaration of Competing Interest
All authors have no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kapania E.M.Cavallazzi R.Necrotizing pneumonia: a practical guide for the clinician Pathogens 13112024 Nov 109843959953710.3390/pathogens 13110984 PMC 11597800 · doi ↗ · pubmed ↗
- 2Metlay J.P.Waterer G.W.Long A.C.Anzueto A.Brozek J.Crothers K.Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America Am J Respir Critic Care Med 20072019 Oct 1e 45e 6710.1164/rccm.201908-1581 STPMC 681243731573350 · doi ↗ · pubmed ↗
- 3Alhazzani W.Møller M.H.Arabi Y.M.Loeb M.Gong M.N.Fan E.Surviving Sepsis Campaign: guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19)Intensive Care Med 462020 May 8548873222281210.1007/s 00134-020-06022-5PMC 7101866 · doi ↗ · pubmed ↗
- 4Chatha N.Fortin D.Bosma K.J.Management of necrotizing pneumonia and pulmonary gangrene: a case series and review of the literature Can Respir J 2142014 Jul-Aug 2392452479125310.1155/2014/864159 PMC 4173892 · doi ↗ · pubmed ↗
- 5Diep B.A.Equils O.Huang D.B.Gladue R.Linezolid effects on bacterial toxin production and host immune response: review of the evidence Curr Ther Res Clin Exp 7332012 Jun 861022464859610.1016/j.curtheres.2012.04.002PMC 3954010 · doi ↗ · pubmed ↗
- 6Stevens D.L.Wallace R.J.Hamilton S.M.Bryant A.E.Successful treatment of staphylococcal toxic shock syndrome with linezolid: a case report and in vitro evaluation of the production of toxic shock syndrome toxin type 1 in the presence of antibiotics Clin Infect Dis 4252006 Mar 17297301644712410.1086/500265 · doi ↗ · pubmed ↗
- 7Kato H.Hagihara M.Asai N.Shibata Y.Koizumi Y.Yamagishi Y.Meta-analysis of vancomycin versus linezolid in pneumonia with proven methicillin-resistant Staphylococcus aureus J Glob Antimicrob Resist 242021 Mar 981053340101310.1016/j.jgar.2020.12.009 · doi ↗ · pubmed ↗
- 8Verma A.K.Bauer C.Yajjala V.K.Bansal S.Sun K.Linezolid attenuates lethal lung damage during postinfluenza methicillin-resistant Staphylococcus aureus pneumonia Infect Immun 87102019 Oct 1012810.1128/IAI.00538-19PMC 675930831383747 · doi ↗ · pubmed ↗