Extensive Lymphadenopathy in an HIV‐Negative Patient With Multidrug‐Resistant Tuberculosis
Tomoyuki Araya, Toshiyuki Kita, Kazuhiko Iwasaki, Takayuki Higashi, Ryo Hara, Hazuki Takato

TL;DR
An HIV-negative patient with drug-resistant tuberculosis developed severe lymph node swelling, showing that this can happen even without HIV.
Contribution
Demonstrates that extensive lymphadenopathy can occur in HIV-negative patients with multidrug-resistant tuberculosis.
Findings
An HIV-negative patient with multidrug-resistant tuberculosis had severe lymph node involvement.
Extensive lymphadenopathy was observed in multiple extrapulmonary regions.
This case shows that marked lymph node disease can occur in HIV-negative individuals with TB.
Abstract
Tuberculous lymphadenitis is generally more severe in patients with HIV infection. We present an HIV‐negative patient with multidrug‐resistant tuberculosis who developed severe, extensive lymphadenitis involving multiple extrapulmonary regions. This clinical image highlights that marked lymph node involvement may occur in HIV‐negative patients presenting with pronounced systemic symptoms. Extensive lymphadenopathy is uncommon in HIV‐negative patients with tuberculosis. This clinical image highlights the striking CT appearance of extensive extrapulmonary lymph node involvement in symptomatic multidrug‐resistant tuberculosis, even in the absence of HIV infection.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
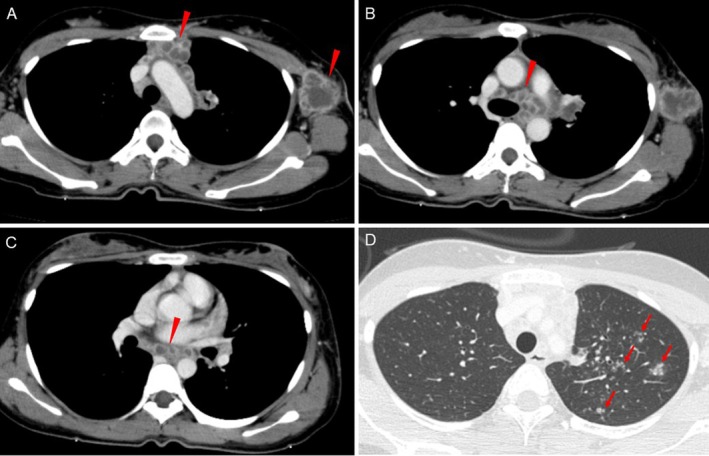 Figure 1
Figure 1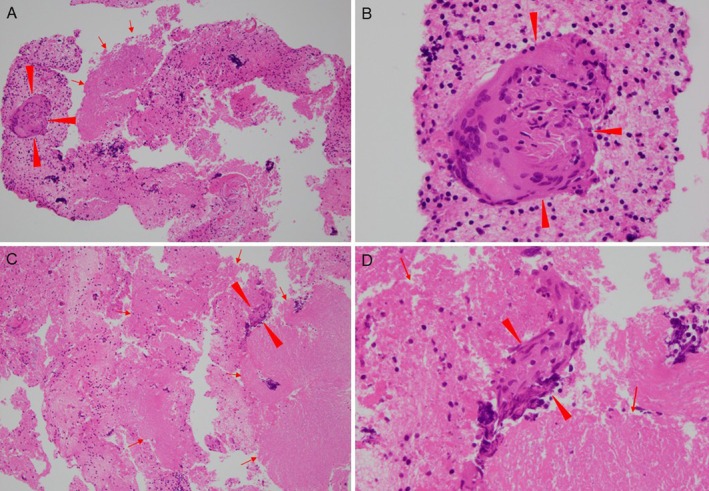 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphadenopathy Diagnosis and Analysis · Diagnosis and treatment of tuberculosis · Infectious Diseases and Tuberculosis
Tuberculous lymphadenitis is often more severe in patients with HIV infection [1]. However, extensive lymphadenopathy has also been reported in HIV‐negative patients with tuberculosis presenting with marked systemic symptoms, such as fever and weight loss [2].
A 26‐year‐old woman presented with a 2‐month history of persistent fever, a 10‐kg weight loss and painful swelling of the left axillary lymph nodes. Contrast‐enhanced chest computed tomography revealed extensive lymphadenopathy involving the mediastinal, hilar and left axillary regions, along with multiple fine nodules in the left upper lobe (Figure 1). Lymph node enlargement was also noted in part of the upper abdomen.
Laboratory testing showed leukocytosis and elevated C‐reactive protein levels. The interferon‐gamma release assay was positive, while HIV antigen/antibody testing was negative. Sputum smears and polymerase chain reaction testing for Mycobacterium tuberculosis were negative. Endobronchial ultrasound‐guided transbronchial needle aspiration of mediastinal lymph nodes (#4L and #7) demonstrated granulomas with caseous necrosis (Figure 2), and cultures from lymph node aspirates and sputum grew Mycobacterium tuberculosis . Drug susceptibility testing confirmed multidrug‐resistant tuberculosis (MDR‐TB).
The patient was treated with an 18‐month multidrug regimen including bedaquiline, delamanid and linezolid. This case highlights that MDR‐TB presenting with marked systemic symptoms may be associated with extensive extrapulmonary lymphadenopathy even in HIV‐negative patients.
Author Contributions
Tomoyuki Araya drafted the manuscript and verified the clinical data. Toshiyuki Kita supervised the work and critically reviewed the manuscript. Kazuhiko Iwasaki, Takayuki Higashi, Ryo Hara and Hazuki Takato reviewed the manuscript and contributed to data verification. All authors read and approved the final manuscript.
Funding
The authors have nothing to report.
Ethics Statement
The case report was approved by the ethics committee of the NHO Kanazawa Medical Center (Approval No. R07‐058). The study was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Consent
The authors declare that written informed consent was obtained for the publication of this manuscript and accompanying images using the consent form provided by the Journal.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1C. F. von Reyn , R. D. Arbeit , and C. R. Horsburgh , “HIV‐Associated Tuberculosis,” New England Journal of Medicine 391 (2024): 1662–1663, 10.1056/NEJ Mc 2411285.39476355 · doi ↗ · pubmed ↗
- 2C. Collu , A. Fois , P. Crivelli , et al., “A Case‐Report of a Pulmonary Tuberculosis With Lymphadenopathy Mimicking a Lymphoma,” International Journal of Infectious Diseases 70 (2018): 38–41, 10.1016/j.ijid.2018.02.011.29477363 · doi ↗ · pubmed ↗