An affordable and optimized 3D biomodel for sinonasal surgery training
Marcelo Augusto Antonio, Sergio Lopes Fernandes Ramos, Fernando Augusto Lima Marson, Mariana Dalbo Contrera Toro, Eulalia Sakano

TL;DR
Researchers created a low-cost 3D surgical training model for sinonasal procedures that senior surgeons found realistic and useful for repeated practice.
Contribution
The study introduces a cost-effective and reproducible 3D biomodel for endonasal surgery training validated by senior rhinologists.
Findings
The biomodel's anatomical accuracy and haptic fidelity were rated highly by senior rhinologists.
The model's production cost was approximately US$43.37 per unit.
Most surgical tasks scored above 4.0 on a 5-point Likert scale for anatomical similarity.
Abstract
•An affordable set was developed for endonasal surgical training.•Senior rhinologists rated its anatomical accuracy and haptics as realistic.•The set offers a practical solution for repetitive surgical practice. An affordable set was developed for endonasal surgical training. Senior rhinologists rated its anatomical accuracy and haptics as realistic. The set offers a practical solution for repetitive surgical practice. To develop and evaluate the anatomical accuracy and haptic fidelity of an affordable kit consisting of a silicone head, a foam support, and a 3D-printed biomodel of the paranasal sinuses for surgical training. This single-center, technological, and interventional study detailed the development of a human sinus biomodel. Its anatomical and haptic evaluation was conducted by ten senior rhinologists, who performed 37 standard surgical tasks. Participants rated…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
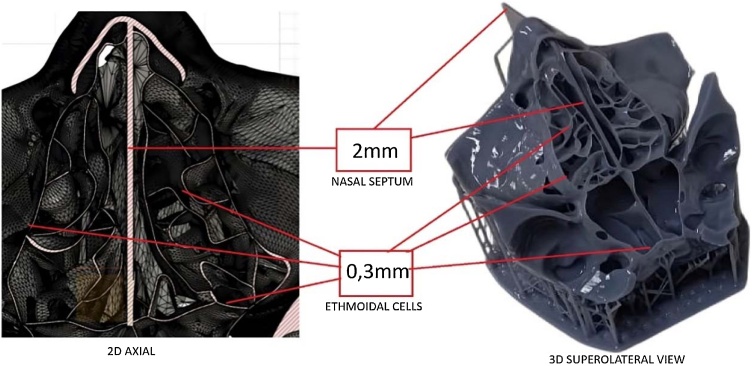 Figure 1
Figure 1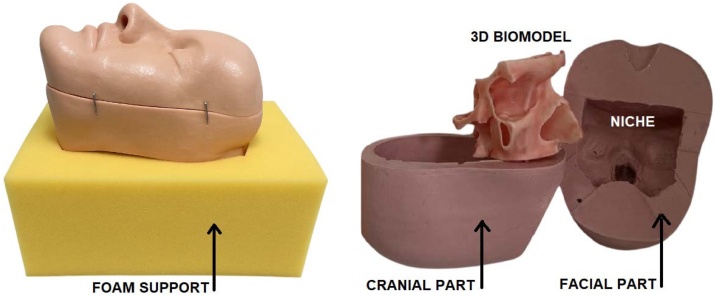 Figure 2
Figure 2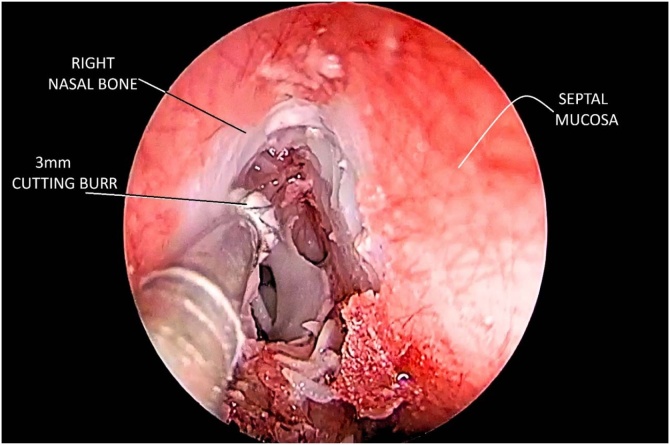 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSurgical Simulation and Training · Anatomy and Medical Technology · Sinusitis and nasal conditions
Introduction
Studies have shown that hands-on training enhances surgeons’ ambidextrous dexterity, contributing to greater procedural safety and reduced surgery time.1^,^2 Achieving proficiency in surgical learning and minimizing complications involves significant lifelong costs. It is essential to consider not only material resources but also the time dedicated to foundational scientific studies and continuing education necessary to keep knowledge current.2
From their inception to the present day, medical schools have continuously sought effective methods to teach and improve surgical skills. While cadaveric training remains the gold standard, it presents several drawbacks, including ethical, religious, sanitary, and financial concerns. Alternative training methods include animal models, virtual reality simulators, and silicone or resin biomodels, which may or may not be produced using 3D printing technology. Although both virtual and physical models offer distinct advantages, their high costs and anatomical limitations remain significant challenges.3
3D printing has emerged as a promising alternative, enabling the creation of increasingly detailed anatomical replicas. Also known as additive manufacturing, this technique constructs objects layer by layer. The first method, stereolithography, was introduced in 1984 by Charles Hull, using ultraviolet light to polymerize resins.4 3D-printed models are typically generated from computed tomography and magnetic resonance imaging scans using software such as Mimics 24.0 (Materialise; Leuven, Belgium) and OsiriX 14.1 (Pixmeo SARL; Geneva, Switzerland), which assist in converting medical image data into 3D-printable files. In otolaryngology, particularly rhinology, some 3D-printed models are designed to simulate internal carotid artery injury and bleeding control, allowing surgeons to refine their skills prior to real procedures.5^,^6
The most frequently used tool in rhinology and neurosurgery to assess the effectiveness of biomodels as simulators is the Likert scale, which evaluates aspects such as agreement, frequency, importance, similarity, probability, and quality. While biomodels benefit from technological advancements and often score highly on Likert scales, challenges remain regarding anatomical fidelity, tissue realism, and cost-effectiveness. In Brazil, where there are over 8,000 otolaryngologists and 298 first-year residents, the demand for accessible and high-quality training models is significant, underscoring the urgent need for continued innovation and investment in this area.7
Regardless of the standard operating protocol employed in biomodel creation, fundamental principles of health technology assessment ‒ such as efficacy, effectiveness, and efficiency ‒ should always be considered, along with continuous horizon scanning and technology monitoring. Fortunately, 3D printers are expected to become increasingly accessible, making biomodels more affordable and widely available.
Given the current scarcity and high cost of biomodels for Endoscopic Sinus Surgery (ESS) training ‒ such as those produced by Phacon (Leipzig, Germany)8 and Fusetec (Adelaide, South Australia)9 ‒ the authors aimed to develop and evaluate the anatomical accuracy and haptic realism of an affordable set for ESS. This set consists of a silicone head, a foam support, and a 3D-printed biomodel of the paranasal sinuses.
Methods
A single-center study was proposed the Department of Ophtalmology and Otorhinolaryngology at the Faculty of Medical Sciences of the State University of Campinas (UNICAMP). All participants provided written informed consent. The study was approved by the University of Campinas Ethical Committee (CAAE: 53904921.0.0000.5404).
Study design
This was a technological study aimed at creating a set consisting of a silicone head with a 3D biomodel of the paranasal sinuses and a head support, in addition to an interventional study involving evaluation by rhinologists.
Standard operating protocol for biomodel development
The authors have filed a patent application with the National Institute of Industrial Property (nº BR 10 2025010414 8), and all the protocols detailing the required steps, materials, and procedures are available in the Supplement section to ensure the reproducibility of the set.
Fig. 1 shows two-dimensional and three-dimensional representations of the ethmoidal labyrinth based on computed tomographic data used in the image modeling and 3D printing process.Fig. 1. Two-dimensional and three-dimensional representations of the ethmoidal labyrinth based on computed tomographic data. Left: Axial computed tomographic highlighting the anterior and posterior ethmoidal cells. Right: superolateral view of the corresponding 3D-printed model in gray resin. All ethmoidal walls were printed with a uniform thickness of 0.3 mm, and a 2.0 mm nasal septum separates the two sides centrally.Fig. 1
Peer evaluation by experts
The biomodel required hand-on manipulation for further validation. For this purpose, the study selected senior rhinologists from nine Brazilian universities: the State University of Londrina, the Federal University of Minas Gerais, the Federal University of São Paulo, the Federal University of Rio Grande do Sul, the Lutheran University of Brazil, the University of Brasília, the Santa Casa de São Paulo School of Medical Sciences, the State University of Rio de Janeiro, and the University of São Paulo (which contributed two participants).
Inclusion criteria required that evaluators be faculty members experienced in endoscopic nasal surgery and affiliated with a medical residency program. Exclusion criteria ruled out participants with known allergies to polyamide, rubber, or silicone, as well as those without access to a laboratory equipped for endoscopic nasal surgery simulation.
Each rhinologist received a package containing the set, along with a booklet titled Standard Operating Procedure for 3D Biomodel Dissection. The booklet outlined all the materials required for the dissection, followed by the sequence of tasks to be performed and evaluated using an answer sheet.
Initially, the rhinologist was informed: “Although there is no unique sequence for ESS, it is requested that each dissection step be followed in the stipulated order for methodological reasons. It is also advisable not to use surgical instruments other than those previously mentioned. Silicone cannot withstand cutting with sharp materials followed by traction; it tears easily. Rotations above 5.000 rotations per minute (r.p.m.) (or pressure above 4 Kgf/cm^2^ when using nitrogen), without irrigation, do not burn the silicone but can melt the 3D biomodel. The inferior turbinate will not be evaluated, nor will the nasal alae, which are only intended to support the endoscope”.
Once this was established, the rhinologist proceeded with tasks in the left nasal cavity, following the written instructions in the booklet: “Question #1: Start by positioning the head on the foam support as desired. Use the 30 ° endoscope. Check for any synechia between the middle turbinate and the nasal septum using the Cottle septum elevator or ball-seeker. Do not separate them yet. Gently medialize the middle turbinate using the Cottle septum elevator, avoiding the axilla. Check the uncinate process. Answer Question #1 and #2”.
Question #1 was designed to assess anatomic landmark accuracy, while Question #2 focused on the usefulness of the task for ESS training, as shown in Table 1. After each question, participants were asked to provide feedback using a 5-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree). This structure was applied to all 37 questions, which were grouped in Table 1 according to their focus on either anatomical accuracy or task relevance for surgical training.Table 1. Answers among evaluators regarding anatomical accuracy and biomodel’s usefulness.Table 1. QuestionAnatomic accuracyNumber of answers on likert scaleMean rating score (SD)123451Left paradoxical middle turbinate and uncinate process464.6 (0.49)3Left ethmoidal bulla and ethmoidal infundibulum space464.6 (0.49)7Left basal lamella1634.2 (0.60)10Left sphenoid sinus, carotic artery bulge, and optic nerve canal554.5 (0.50)19Left frontal sinus1544.2 (0.87)20Right concha bullosa and the prominent agger nasi644.4 (0.49)22Right uncinate process and ethmoidal infundibulum554.5 (0.50)34Final aspect of Draf III11354.2 (0.98)Usefulness of the task2Left middle turbinate medialization1634.2 (0.60)4Left uncinectomy21513.4 (1.02)5Left maxillary antrostomy12433.9 (0.94)6Left bullectomy and anterior ethmoidectomy1634.2 (0.60)8Left posterior ethmoidectomy914.1 (0.30)9Left transethmoidal sphenoidotomy1634.2 (0.60)11Left squeletization and fracture of the lamina papyracea1454.4 (0.66)12Left periorbit incision22513.5 (0.92)13Left lacrimal bone drilling/debulking for lacrimal sac exposure12253.1 (1.04)14Left use of a silver pin to mark the location of the lacrimal sac and common canaliculus2532.9 (1.04)15Left Draf I824.2 (0.40)16Left Draf IIA1724.1 (0.54)17Left Draf IIB1634.2 (0.60)18Left: use of an acrylic yarn to identify the first olfactory fibers13333.8 (0.98)21Right concha bullosa reduction2444.2 (0.75)23Right uncinectomy13423.7 (0.90)24Right maxillary antrostomy11354.2 (0.98)25Right anterior ethmoidectomy1544.3 (0.64)26Right posterior ethmoidectomy1634.2 (0.60)27Right transethmoidal sphenoidotomy554.5 (0.50)28Right excision of part of the lamina papyracea and periorbit incision554.5 (0.50)29Right lacrimal bone drilling/debulking for lacrimal sac exposure1544.3 (0.64)30Right Draf I12433.9 (0.94)31Right Draf IIA534.5 (0.50)32Right Draf IIB374.7 (0.46)33Draf III284.8 (0.40)Availability of biomodels and dexterity training35Lack of biomodels for Endoscopic Sinus Surgery (ESS) training in Brazil11534.0 (0.89)36Lack of affordable biomodels for ESS training in Brazil374.7 (0.46)37Bimanual dexterity is acquired through repetitive training rather than sporadic exposition284.8 (0.40)For each of the 37 basic items related to Endoscopic Sinus Surgery (ESS) training, note the number of times a score was assigned based on a 5-point Likert scale (columns from 1 to 5), along with the mean value and Standard Deviation (SD) of the responses.
The final three questions assessed agreement with the following statements: “There is a lack of biomodels for ESS training in Brazil (affordable or not)” and “Bimanual dexterity is acquired through repetitive training rather than sporadic exposure”. At the end of the answer sheet, participants were also invited to respond to an open-ended question: “Comment on how you could improve this biomodel” (Table 1). Responses were submitted anonymously via the phone number provided in the informed consent form.
Statistical analysis
Responses were compiled using Excel® (Microsoft Excel; Microsoft Corp., Redmond, WA, USA). The statistical analysis was performed using SPSS (Statistical Package for the Social Sciences) software (IBM SPSS Statistics, version 28; IBM Corp., Armonk, NY, USA). The mean and standard deviation were calculated for each response.
Results
A total of 10 rhinologists were included in the analysis, as they returned fully completed answer sheets. One rhinologist omitted a single response, which was subsequently considered neutral and assigned a score of “3”. Table 1 shows how many times each response option on the Likert scale was selected for each question.
Regarding anatomical accuracy of the bullous conchae, uncinate process, maxillary and sphenoid antrum, frontal recess, and the final aspect of the Draf III procedure, none of the 37-items described in Table 1 had a mean score below 4.0 ± SD on either sides.
Concerning the criterion of task usefulness, only one item received a mean score below 3 (neutral): 2.9 ± 1.04, which referred to the use of a silver pin to mark the location of the lacrimal sac and common canaliculus. Similarly, the rhinologists found the lacrimal bone drilling/debulking procedure suboptimal for exposing the lacrimal sac, with a mean score of 3.1 ± 1.04 on the left side. Uncinectomy was rated 3.4 ± 1.02 on the left and 3.7 ± 0.9 on the right, while the periorbit incision received scores of 3.5 ± 0.92 on the left and 4.5 ± 0.5 on the right. All other steps, whether performed with manual or powered instruments, scored above 4.0 ± SD.
There was consensus that bimanual dexterity is developed through repetitive training rather than sporadic exposure, as reflected by a mean score of 4.8 ± 0.4. Regarding the statement about the lack of biomodels for ESS training in Brazil, the initial mean score was 4.0 ± 0.89, which increased to 4.7 ± 0.46 after the word “affordable” was added to the statement.
In response to the open-ended question, “Comment on how you could improve this biomodel”, 9 out of 10 participants suggested improving the consistency of the mucosa, while 7 out of 10 recommended enhancing the elasticity of the nasal tip by using a more malleable silicone.
The costs for producing one complete set are detailed in Table 2.Table 2. Quantity and cost of supplies required to produce one head-biomodel-support set.Table 2. SupplyPrice (US)a3D printer800.00 (unit)1Permanent facilityWhite acrylate resin43.5 per L50 mL2.1770% alcohol1.74 per L1 L1.74Cristal acetic silicone2.45 per 50g50g2.45Liquid silicone5.5 per 300g20g0.36Crystal platinum silicone52.24 per Kg0.07 Kg3.65White silicone rubber12,19 per Kg2.7 Kg26.17Beige silicone dye5.22 per 100g15g0.78Red silicone dye3.87 per 100g2g0,07Foam support2.2612.26Stationery for Standard Operating Procedure3.4813.48Customization (materials)24.93/100 pieces10.24**Total gross US 0.24 per biomodel, based on the production of 100-units. For this quantity, the following materials were used: 200-pins (US 1.95), 8 m of red silicone-insulated wire (US 1.53), 200 round foam pieces (US 10.45), totaling US = R$ 5,74.
Discussion
The Likert scale responses in this study were based on comparisons each rhinologist made with their prior experiences using cadavers and other biomodels. A 5-point Likert scale was chosen over a 9-point version to simplify the decision-making process between opposing viewpoints, making it easier to interpret as approval or disapproval of the set. Upon approval, the set could be mass-produced for broader evaluation, assessing its impact on residents’ surgical training.
Overall, since most scores exceeded 4.0 ± SD on a scale ranging from 1 (strongly disagree) to 5 (strongly agree), the evaluation supports the biomodel’s anatomical accuracy and its suitability for ethmoidal and frontal sinus manipulation. As in previous studies,10, 11, 12, 13, 14 this model was based on tomography images. However, extensive digital sculpting was pivotal to achieving very thin, yet bone-like rigid, ethmoidal cells (Fig. 2). Reproducing the haptics of the ethmoidal labyrinth proved to be a trial-and-error process involving the testing of multiple wall thicknesses and different resins. This iterative approach required close collaboration between a Blender 3D (Blender Foundation; Amsterdam, Netherlands) modeler and the anatomical expertise of the authors, ultimately extending the development time. Each pilot model required further refinements after printing.Fig. 2. Three-piece assembly of the training set. On the left, the silicone head is secured by the foam support. On the right, the two silicone head segments and the central niche designed to accommodate the 3D-printed biomodel are shown.Fig. 2
Due to its low cost and ease of acquisition, acrylic resin was an accessible material for testing and demonstrated high applicability, even for very thin walls. It provided an ideal balance of hardness and flexibility for both manual and powered instruments, without melting or producing powder that could blur the lens, as observed with other materials like polyamide.12 However, no acrylic resin can withstand high-speed drilling indefinitely without beginning to melt. This limitation is not always disclosed by biomodel suppliers. In our study, drill speeds were limited to 5,000 rpm (or drilling pressure of up to 4 Kgf/cm^2^ using nitrogen) and required irrigation to prevent melting. (Fig. 3) (Video supplement).Fig. 3. Endoscopic view during the simulation of drilling access to the frontal sinus. The whitish area simulates exposed bone after detaching the red mucosal layer. A 3 mm cutting burr is drilling out the frontal beak region. Fragments of synthetic bone and mucosa are visible at the bottom.Fig. 3
Mucosal haptics, especially during uncinectomy and manipulation of the lacrimal bone, lacrimal sac, and periorbita incision, received the lowest scores among the 37 evaluated items, indicating limited utility for surgical training. Achieving realistic width and flexibility for mucosa and the lacrimal sac/duct remains a challenge. Multi-material printers offer potential by layering materials with different textures to simulate bone and mucosa.15 However, such printers are still expensive and not widely accessible. The authors tested materials such as VeroWhitePlus/TangoPlus (Stratasys; Eden Prairie, USA), as used in a previous study.15 Although the hardness of the bony components was partially satisfactory, several ethmoidal cells were overly rigid and had their lumens inadvertently filled with resin.
There are studies focused on 3D biomodels designed primarily for drilling, often without a mucosa layer.5^,^11^,^12^,^16 In contrast, our study tested different materials to simulate mucosa, including ultracentrifuged latex, platinum silicone, thermoexpandable paint, latex paint, and liquid rubber, either alone or in various combinations. We noted that some of these materials could not cure, be detached, or fill thin spaces, and even merged with the resin of the bony parts, compromising final hardness. However, the acetic silicone used for this biomodel did not compromise such aspects.
Although new simulators are often considered useful by residents and/or senior rhinologists, their limited availability likely stems from high production costs or lack of investment in large-scale manufacturing.5^,^6^,^11^,^17^,^18 The high price of biomodels limits opportunities for repeated practice. In this study, rhinologists agreed that repetition is essential for effective surgical training. From its inception, a key objective in developing this biomodel was to avoid techniques and materials that would unnecessarily increase costs. For example, the foam support needed to accommodate various head positions, contain fluids when necessary, and remain lightweight to reduce shipping costs. Many simulators require secure fixation to specific supports.8^,^9^,^12 Furthermore, materials were selected with long-term durability in mind, ensuring the model’s relevance amid technological advancements ‒ an important consideration before investing in more expensive solutions, such as augmented or virtual reality.3
Although the total production cost was significantly reduced, manual labor for head and support assembly and post-processing was not included, as it can vary depending on commercial scale. The head required artisanal work, but once its molds were finalized, mass production became feasible. Despite being the most expensive component, the 3D printer used was one of the simplest models, costing approximately US$ 800.00.
The relatively small number of evaluators is a limitation of the study. Additionally, relying solely on experienced specialists rather than including undergraduates or residents introduces potential bias. Nevertheless, their participation offered the advantage of drawing upon substantial experience with live surgeries, cadaver dissections, and widely used commercial biomodels. The absence of simulated blood and cerebrospinal fluid also represents a limitation.
It is worth noting that anatomical features or variations, such as tumor lesions or bone dehiscence/thickening, could be added to the file using Blender 3D, thereby enhancing its versatility for surgical simulation.
Conclusion
It is feasible to produce cost-effective 3D biomodels that incorporate anatomical variations, enhancing their value as educational tools, particularly for developing the psychomotor skills of Otolaryngology residents and contributing to the shortening of surgical learning curves.
ORCID ID
Marcelo Augusto Antonio: 0000-0002-5858-1229
Sergio Lopes Fernandes Ramos: 0009-0001-6931-453X
Fernando Augusto Lima Marson: 0000-0003-4955-4234
Mariana Dalbo Contrera Toro: 0000-0002-5294-369
Eulalia Sakano: 0000-0002-5963-912X
Funding
The research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. All expenses were covered by the first author, including the production of the video described in the Methods section, silicone heads, foam supports, dissection manuals, shipping to evaluators, as well as all the silicone used in the unsuccessful attempts to create the silicone head.
Data availability statement
We declare that all data is available in the repository.
Declaration of competing interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Naik V.N.Matsumoto E.D.Houston P.L.Fiberoptic orotracheal intubation on anesthetized patients: do manipulation skills learned on a simple model transfer into the operating room?Anesthesiology.9520013433481150610410.1097/00000542-200108000-00014 · doi ↗ · pubmed ↗
- 2Scott D.J.Bergen P.C.Rege R.V.Laparoscopic training on bench models: better and more cost effective than operating room experience?J Am Coll Surg.19120002722831098990210.1016/s 1072-7515(00)00339-2 · doi ↗ · pubmed ↗
- 3Arora H.Uribe J.Ralph W.Assessment of construct validity of the endoscopic sinus surgery simulator Arch Otolaryngol Head Neck Surg.13120052172201578176110.1001/archotol.131.3.217 · doi ↗ · pubmed ↗
- 4Muto J.Carrau R.L.Oyama K.Otto B.A.Prevedello D.M.Training model for control of an internal carotid artery injury during transsphenoidal surgery Laryngoscope.127201738432747042810.1002/lary.26181 · doi ↗ · pubmed ↗
- 5Maza G.Van Koevering K.K.Yanez-Siller J.C.Surgical simulation of a catastrophic internal carotid artery injury: a laser-sintered model Int Forum Allergy Rhinol.9201953593037660610.1002/alr.22178 · doi ↗ · pubmed ↗
- 6Associação Brasileira de Otorrinolaringologia e Cirurgia Cervicofacial. Censo ABORL-CCF [Internet]. 2023 [cited 2025 Jan 17]. https://aborlccf.org.br/wp-content/uploads/2023/12/aborl_censo_2023-2.pdf. Accessed May 29, 2025.
- 7Leong S.C.Strzembosz A.Tan N.C.Validation of a three-dimensionally printed simulator for training in endoscopic sinonasal surgery Rhinology.6120233763823709234110.4193/Rhin 22.442 · doi ↗ · pubmed ↗
- 8Suzuki M.Vyskocil E.Ogi K.Remote training of functional endoscopic sinus surgery with advanced manufactured 3D sinus models and a telemedicine system Front Surg.8202174683710.3389/fsurg.2021.746837 PMC 851710634660685 · doi ↗ · pubmed ↗