The development of a therapeutic strategy for post-acute sequelae of COVID-19 should be based on an efficient classification of pathogenesis
Heng Wang, Li Shen, Song Xue

TL;DR
This paper suggests that treating long-term effects of COVID-19 needs better classification based on disease causes.
Contribution
The paper introduces a classification framework for PASC based on distinct pathogenesis types.
Findings
Symptom-based classification may overlook recovery potential in specific PASC subgroups.
Future research should categorize PASC by underlying pathogenesis for better treatment strategies.
Four key pathogenesis types are identified for guiding patient enrollment in clinical trials.
Abstract
The treatment of post-acute sequelae to COVID-19 (PASC) remains challenging. Defining PASC solely based on symptoms and disease duration in clinical trials can mask the potential for recovery in specific patient subgroups. A good design for future research requires a clear classification of various PASC according to different pathogenesis under the general diagnosis. Here, we discuss four key types of pathogenesis that should be recognized to determine the enrollment of PASC patients.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
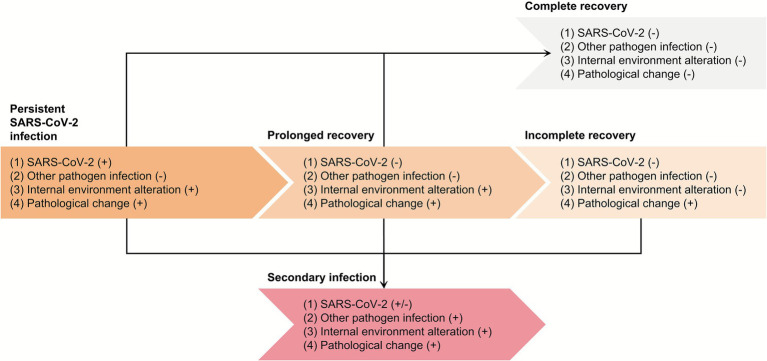 Figure 1
Figure 1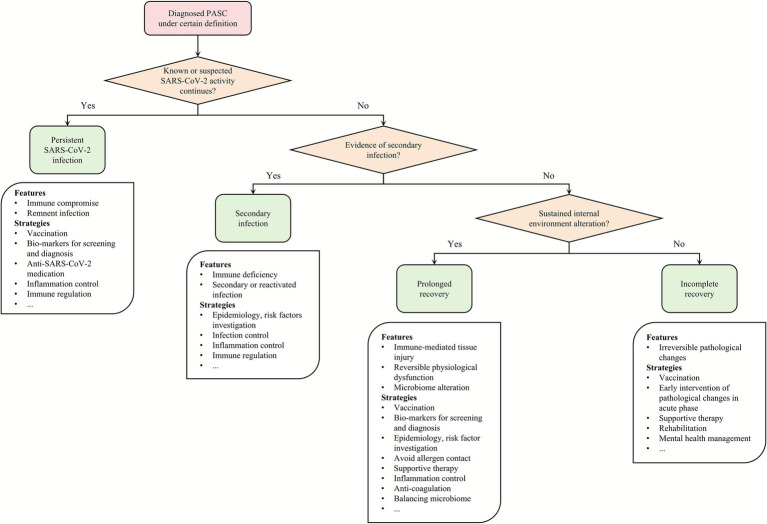 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLong-Term Effects of COVID-19 · Pharmacological Receptor Mechanisms and Effects · Intensive Care Unit Cognitive Disorders
Introduction
1
Patients with coronavirus disease 2019 (COVID-19) can have persistent health issues, including new-onset or enhanced symptoms or signs that are beyond the course of the acute disease after severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection. These conditions are referred to as post-acute sequelae/syndrome of COVID-19 (PASC), long-term condition/complication of COVID-19, long COVID, etc.
The average symptom duration of the COVID-19 acute phase in mild to moderate cases, which is characterized by fever and respiratory symptoms, is 10 days, and the viral RNA shedding can no longer be detected using a nasopharyngeal swab in 2–4 weeks in most cases (1). The incidence of PASC is heterogeneous and estimated to be 10%–15% (2). A widely accepted definition of long COVID can be interpreted as “a condition lasts for at least 2 months, usually 3 months after the acute symptom onset, which is presumably caused by SARS-CoV-2 infection and cannot be explained by an alternative diagnosis” (3). The definition from the U.S. Centers for Disease Control and Prevention regards persistent conditions over 4 weeks after symptom onset with uncharacteristic viral test and antibody profile as late sequelae of COVID-19 (4). Approximately 70%–90% of certain PASC conditions can be recovered in 1 year, but are able to cause a delayed resumption of study (5, 6). There are patients suffering from PASC for a longer period. A considerable prevalence of PASC could still be found 3 years after the symptom onset (7).
Currently, PASC represents a group of symptom-centered conditions with mixed subjects investigated, which baffles standard evaluation and therapy. A classification of PASC based on the underlying disease pathogenesis can promote precision medicine. Here, we discuss four types of PASC pathogenesis based on the disease course, with typical examples that require different therapeutic strategies.
PASC pathogenesis
2
Persistent SARS-CoV-2 infection
2.1
Persistent SARS-CoV-2 infection, resulting from immune compromise and viral reservoirs in tissues, is not uncommon and is a suspected cause of PASC (8).
It was estimated that 0.7%–3.5% and 0.5%–1% infections can last persistently for at least 30 days and 60 days, respectively, and a risk of more than 50% higher odds of long COVID-19 was found in these cases compared with non-persistent ones (9). The commonly used approaches for pathogen detection, e.g., rapid antigen test for virus antigens and reverse transcription polymerase chain reaction for virus RNA, usually collect samples from the upper respiratory tract, which underestimates the incidence or prevalence of persistent infections in the population. In autopsies, SARS-CoV-2 RNA was found in the vagus nerve, providing evidence of virus-induced inflammation that can cause symptoms related to autonomic nervous system disorders, e.g., postural orthostatic tachycardia syndrome after COVID-19 (10, 11). A study reported an elevation of SARS-CoV-2 antigens by 10.6, 8.7, and 5.4% between 3 and 6 months, between 6 and 10 months, and between 10 and 14 months after diagnosis, respectively, compared with pre-pandemic samples in plasma, and the replicating virus was hypothesized to hide in organs and seed viral components through the bloodstream (12). COVID-19-related myocarditis can happen weeks or months after the acute phase (13). Although evidence suggested that myocarditis in the post-acute period is largely caused by inflammation, virus infection in cardiomyocytes, endothelial cells, and macrophages can last for up to 18 months, which is consistent with the conception of persistent infection (14).
Given that the virus is still active, this type of PASC can be considered a continuous remnant infection after the acute phase.
Secondary infection
2.2
Secondary infection is a commonly reported complication that constitutes PASC.
Immune deficiency is a featured perturbation found in long COVID-19 patients, and manifestations caused by evidenced secondary infection should be defined as a unique PASC (15). In a cohort focusing on allergic diseases after the acute COVID-19 phase, an increased hazard of Aspergillus pneumonia was found (16). The increased prevalence of fungal infections during the pandemic was suspected to be a result of both SARS-CoV-2-induced immune deficiency and iatrogenic factors, e.g., using immunomodulatory agents and invasive procedures (17). In another large cohort with 2.4 million cases, researchers found that COVID-19 patients had a higher risk of 1.59 hazard ratio for developing herpes zoster at a 1-year follow-up (18). The activation of Epstein–Barr virus was suspected to be the cause of myalgic encephalomyelitis or chronic fatigue syndrome (ME/CFS) in PASC (19).
Secondary infection initiates a new disease course parallel to COVID-19 and its sequelae, which can be diagnosed as PASC for a period overlapping.
Prolonged recovery
2.3
The homeostasis of the internal environment is believed to be stabilized by the neurologic system, immune system, and endocrine system, forming a neuro-immuno-endocrinologic regulating net (20). The internal environment alteration can continue both when virus replication is active and after virus clearance. There are several mechanisms leading to such a prolonged recovery.
Hypersensitivity
2.3.1
Hypersensitivity, a mechanism underlying autoimmune diseases, also plays a significant role in PASC (21). There are four types of hypersensitivity, (1) type 1, mediated mainly by mast cells and immunoglobulin E (IgE), which is usually addressed as anaphylaxis; (2) type 2, mediated mainly by IgM and IgG, leading to tissue damage (2a) or stimulating reactions (2b); (3) type 3, mediated mainly by immune complexes, leading to local inflammation and tissue damage; and (4) type 4, mediated by T cells, and is divided into four sub-types according to the T cell subgroups (22). Hypersensitivity can be induced when SARS-CoV-2 replication and invasion are active and may continue to exert its effect for a long period after the virus turns negative. The duration of hypersensitivity-induced conditions can fall into the definitive range of PASC. Studies have reported a significant increase in the 30-day hazard of asthma, a typical type 1 hypersensitivity disease, along with other allergic diseases among COVID-19 patients compared with the general population and influenza patients (16, 23). Multi-system inflammatory syndrome that usually occurs in children (MIS-C) weeks or months after the acute phase can be mediated by immunopathology of cytokine storm and autoimmune response, where evidence has illustrated auto-antibodies interacting with endothelium, immune cells, and other host tissues (type 2a hypersensitivity), and immune complexes (type 3 hypersensitivity) trigger inflammation (24). In addition, cytotoxic T cell-induced β cell apoptosis is a typical type 4 hypersensitivity resulting in type 1 diabetes, which may contribute to the increased incidence of type 1 diabetes during the pandemic, as the relationship between type 1 diabetes and SARS-CoV-2 infection appears to be speculative (25, 26).
Cytokine-induced endocrine disruption
2.3.2
Some endocrine disruption can result from factors other than hypersensitivity. The inflammatory status can directly affect the endocrine organs. Hypothalamic–pituitary–adrenal axis plays a central role in multiple long COVID conditions, including cardiopulmonary dysfunction, musculoskeletal diseases, and gastrointestinal symptoms (27). SARS-CoV-2 can lead to arginine vasopressin release stimulated through elevated pro-inflammatory cytokines and dysregulates the hypothalamic–pituitary–adrenal axis (28, 29). Although SARS-CoV-2 vaccination can ameliorate thyroid dysfunction after infection, which indicates a causal influence of virus-induced abnormality, autoimmunity may not be the dominating mechanism with few evidence, and cytokine storm remains to be a validated explanation (30–32). IL1β, IL6, TNF-α, and IFN-γ secreted by dendritic cells and mononuclear macrophages are key mediators of thyroid dysfunction (33). Cytokines can also directly inhibit the secretion of melatonin from the pineal gland, causing disruption of the circadian rhythm (34). The duration for these endocrine disruptions to resolve after the primary inflammatory response to viral infection is unclear.
Hyper-coagulation
2.3.3
The coagulation and fibrinolysis system keeps a fragile balance in inflammation (35). The hyper-coagulation with Virchow’s triad, i.e., endothelial injury, abnormal blood flow, and hypercoagulability, can lead to an increased risk of thromboembolic diseases, e.g., pulmonary embolism and stroke (36). Currently, (1) activation of coagulating factors by inflammation and (2) virus direct cytopathic effect have been well concluded (37, 38), while the blood flow change may be underestimated in PASC hypercoagulation. A meta-analysis of large cohorts revealed that SARS-CoV-2 can twice the risk of atrial fibrillation, the main cause of stroke, in the recovered (39). In severe cases with long-term immobility and individuals suffering from ME/CFS, deep vein thrombosis can also be a life-threatening complication (40).
Microbiome imbalance
2.3.4
Growing evidence indicates that the gut microbiome can regulate the internal environment. The gut–brain axis alteration can cause ME/CFS, a common disease in PASC, through immune, neurological, and metabolic axes, and targeted interventions have shown considerable therapeutic efficacy (41). The microbiome can also be changed by SARS-CoV-2 infection or therapy using glucocorticoids for inflammation control and antibiotics for antibacterial treatment (42–45). The characterized microbiome change in increased Bacteroides, Flavonifractor, Ruminococcus gnavus, and decreased Bifidobacterium, Dorea, and Faecalibacterium prausnitzii, has been observed consistently in PASC patients (42). The emerging field of lung microbiome may provide novel choices for future research in PASC development (46). However, more discovery is needed to develop corresponding therapies for PASC with digital health systems, data science, and bioinformatics.
Incomplete recovery
2.4
Some PASC cases cannot be explained by active infection or undergoing pathophysiology, and their symptoms may result from permanent tissue damage, namely, incomplete recovery.
In the acute phase, SARS-CoV-2 causes severe inflammation that activates several fibrogenic cell pathways and biological axes, leading to fiber deposition (47). This pathological change can irreversibly impair respiratory function. Along with diagnosed diffusion capacity impairment and restrictive pulmonary dysfunction, persistent ground-glass opacities and pulmonary fibrosis in COVID-19 patients did not show recovery in a 1-year follow-up (48). An increased risk of acute myocardial infarction can be found in COVID-19 patients at the 8.5-month follow-up, which can also cause permanent cardiac dysfunction, as cardiomyocytes are not renewable (49).
In these cases, the course of COVID-19 reaches an end where no active infection or internal environment alteration can be reversed with currently available clinical interventions.
Challenges
3
Mechanism overlapping
3.1
Research in basic medicine and biology typically focuses on disease etiology; however, this approach may struggle to distinguish between mechanistic “sets” or “levels” due to their frequent intersection. Efforts were made to classify PASC pathogenesis on some bases. A common framework for describing disease mechanisms is structured around molecular and biological processes and their corresponding morphological (pathological) and functional (pathophysiological) manifestations (50, 51). Anatomical systems based on physiological functions are also a widely used view, which analyzes the pathological changes of each system with little overlapping and provides explanations for the chief complaints (52, 53). With the use of modern biomedical technologies, molecular patterns with machine learning algorithms have become a reliable view for classification, helping to elucidate the biological basis of PASC (54).
Basically, in the disease course, there are two clinical outcomes, recovery and death, where recovery is divided into incomplete recovery and complete recovery. Here, we define the word “prolonged recovery” as a continuous, active disease status that does not reach a clinical outcome (recovery or death), and “incomplete recovery” as one of the clinical outcomes. Our disease course-based classification of PASC groups patients into the following categories: non-recovered (prolonged recovery, with specified subcategories for viral persistence and secondary infection), and incompletely recovered. This system provides a basis for clinical trials by enabling the initial stratification of patients by the underlying pathogenesis, thus minimizing confounding (Figure 1).
Classification of PASC based on pathogenesis. The subtypes of PASC are determined by three characters: SARS-CoV-2 positivity, secondary infection, and reversible internal environment alteration. SARS-CoV-2, severe acute respiratory syndrome coronavirus-2.
Diagnostic uncertainty
3.2
More studies are needed for the individual identification of pathogenesis. After the initial diagnosis of PASC, whether SARS-CoV-2 is still active should be confirmed. Since the upper respiratory tract may test negative in persistent infection, further testing for biopsies, plasma, excreta, etc., may be considered (55). If direct evidence of virus existence cannot be obtained, risk assessment based on autopsy and epidemiological factors may be carried out. Given that co-infections occur in approximately 26% of COVID-19 patients (56), secondary infections likely constitute a substantial proportion of PASC mechanisms; however, the spectrum of secondary infection in PASC patients is yet to be explored. Considering that (1) active SARS-CoV-2 replication and invasion can maintain the immunodeficiency status, and (2) secondary infection is often hard to identify, identification and clearance of SARS-CoV-2 should be prioritized. In prolonged recovery, the mechanisms form a highly interconnected spiderweb, maybe requiring biomarkers with high sensitivity and specificity, including cytokines, immune cells, nutrients, metabolites, and hormones (57, 58), and gut and lung microbiome. Objective results from electro- and/or echocardiography, respiratory examination, ultrasonic, and radiographic imaging should be considered. Only when intervenable changes are excluded can physicians classify the PASC patient into incomplete recovery, to avoid masking underlying recovery (Figure 2).
Referenced workflow for patient enrollment. The flowchart illustrates the analysis and determination of PASC for patient enrollment with corresponding strategies for future investigations into prevention, diagnosis, therapy, and long-term management. PASC, post-acute syndrome of coronavirus disease 2019; SARS-CoV-2, severe acute respiratory syndrome coronavirus-2.
Clinical implementation
3.3
Trials on PASC can enrich severe cases with significant symptoms or signs, as many cases were missed in diagnosis (59). The PASC incidence and severity can also be different among SARS-CoV-2 lineages, e.g., MIS-C severity was highest during the Alpha (B.1.1.7) wave, followed by the Delta (B.1.617.2) wave, and was lowest in the Omicron (B.1.1.529) period (60, 61); the incidence of PASC was estimated to be 10.4, 9.5, 7.7% in Pre-Delta, Delta, and Omicron periods (62). Therefore, epidemiological research on large observational cohorts for the general population is still necessary. It is sometimes unlikely to divide all included PASC patients into the aforementioned pathogenesis types without appropriate diagnosis kits, while specific subgroups with detected remnant SARS-CoV-2 infection, secondary infection, or clear biomarkers indicating internal environment alteration may benefit from precision therapy. Given that PASC is characterized by non-severe baseline disease but remarkable treatment resistance, strict enrollment criteria inevitably shrink the sample size. This elevates the risk of type II statistical error in the outcome analysis. To mitigate this risk, the sample size calculation is indispensable (63). Furthermore, as mental health is an integral yet non-objective component of PASC, it should be formally evaluated with appropriate scales to mitigate the risk of unanticipated confounding (64–66). Considering that some factors in diagnostic results hardly contribute to the probability of necessity, meaning their reversal or re-normalization may not result in a significant reduction in disease severity, causal inference may be carried out before trial enrollment (67, 68).
Discussion
4
Targeting persistent SARS-CoV-2 infection is a promising strategy. Although small-molecule antivirals did not show a significant improvement in enrolled PASC patients (69), taking antivirals during the acute phase may reduce the risk of PASC (70), which may be explained by the effective limitation of virus replication and spreading during the acute phase. Consistently, both pre- and post-COVID-19 vaccination reduced the risk of developing PASC (71). The timing and methods of SARS-CoV-2 clearance should be further investigated in PASC.
Some studies have reported promising results when enrollment was based on specific internal environment alteration. In PASC patients with vitamin K2/D3 deficiency, vitamin intake improved the long COVID-19 index (72). The immunomodulatory therapy methylprednisolone and tocilizumab shortened the hospital stay of MIS-C (73). Convalescent patients with endothelial dysfunction benefited from sulodexide, an anti-thrombotic and pro-fibrinolytic drug (74).
Efforts have been made to treat lung fibrosis, and lung function can be improved by anti-fibrotic medications (75). However, most incomplete recoveries may need physical exercise and other rehabilitation (76).
In conclusion, PASC diagnosis based on symptoms and the duration of disease is commonly used to determine the inclusion criteria of clinical trials. However, PASC varies among different populations, making enrolled cases heterogeneous, thus masking the potential for recovery in subgroups of specific pathogenesis. Developing strategies according to PASC pathogenesis provides causal inference insights for effective ways of controlling symptoms and signs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Puhach O Meyer B Eckerle I. Sars-Cov-2 viral load and shedding kinetics. Nat Rev Microbiol. (2023) 21:147–61. doi: 10.1038/S 41579-022-00822-W, 36460930 PMC 9716513 · doi ↗ · pubmed ↗
- 2Nalbandian A Desai AD Wan EY. Post-COVID-19 condition. Annu Rev Med. (2023) 74:55–64. doi: 10.1146/Annurev-Med-043021-030635, 35914765 · doi ↗ · pubmed ↗
- 3Soriano JB Murthy S Marshall JC Relan P Diaz JV. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect Dis. (2022) 22:E 102–7. doi: 10.1016/S 1473-3099(21)00703-934951953 PMC 8691845 · doi ↗ · pubmed ↗
- 4Datta SD Talwar A Lee JT. A proposed framework and timeline of the spectrum of disease due to SARS-Cov-2 infection: illness beyond acute infection and public health implications. JAMA. (2020) 324:2251–2. doi: 10.1001/Jama.2020.2271733206133 · doi ↗ · pubmed ↗
- 5Chilunga FP Appelman B Van Vugt M Kalverda K Smeele P Van Es J . Differences in incidence, nature of symptoms, and duration of long COVID among hospitalised migrant and non-migrant patients in the Netherlands: a retrospective cohort study. Lancet Reg Health Eur. (2023) 29:100630. doi: 10.1016/J.Lanepe.2023.10063037261215 PMC 10079482 · doi ↗ · pubmed ↗
- 6Yang T Yan MZ Li X Lau E. Sequelae of COVID-19 among previously hospitalized patients up to 1 year after discharge: a systematic review and meta-analysis. Infection. (2022) 50:1067–109. doi: 10.1007/S 15010-022-01862-335750943 PMC 9244338 · doi ↗ · pubmed ↗
- 7Rahmati M Udeh R Kang J Dolja-Gore X Mcevoy M Kazemi A . Long-term sequelae of COVID-19: a systematic review and meta-analysis of symptoms 3 years post-Sars-Cov-2 infection. J Med Virol. (2025) 97:E 70429. doi: 10.1002/Jmv.70429, 40476637 PMC 12143191 · doi ↗ · pubmed ↗
- 8Machkovech HM Hahn AM Garonzik Wang J Grubaugh ND Halfmann PJ Johnson MC . Persistent Sars-Cov-2 infection: significance and implications. Lancet Infect Dis. (2024) 24:E 453–62. doi: 10.1016/S 1473-3099(23)00815-038340735 · doi ↗ · pubmed ↗