Wolf’s isotopic response of eczema after herpes zoster infection: case report and literature review
Yirui Zhao, Min Zhang, Xuanlin Chen, Shuping Guo, Hongye Liu

TL;DR
This paper reports a case of eczema developing at the site of a healed herpes zoster infection, suggesting a possible link between the two conditions.
Contribution
The novelty lies in presenting a new case of Wolf’s isotopic response with eczema and successful treatment with glucocorticoids.
Findings
Eczema developed at the site of a previously healed herpes zoster infection.
Systemic oral glucocorticoids led to significant improvement in skin lesions.
No recurrence was observed during a 3-month follow-up.
Abstract
Wolf’s post-herpetic isotopic response (PHIR) refers to the development of new cutaneous conditions, such as tumors, infections, or immune-mediated diseases, at the site of a previously healed herpetic eruption. The exact pathogenesis of Wolf’s PHIR remains incompletely understood. Four hypotheses have been proposed regarding the mechanism of postherpetic inflammatory isomorphic reactions: viral, immunological, vascular, and neurological. In this case, we show that a patient with eczema developed it at the original site following the resolution of the herpes zoster infection. After 2 weeks of systemic oral glucocorticoid treatment, the skin lesions improved significantly, and there was no recurrence during the 3-month follow-up.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
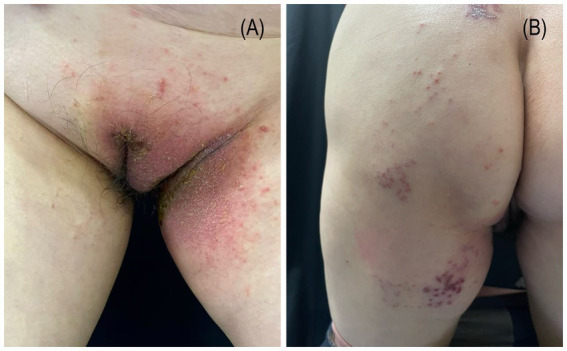 Figure 1
Figure 1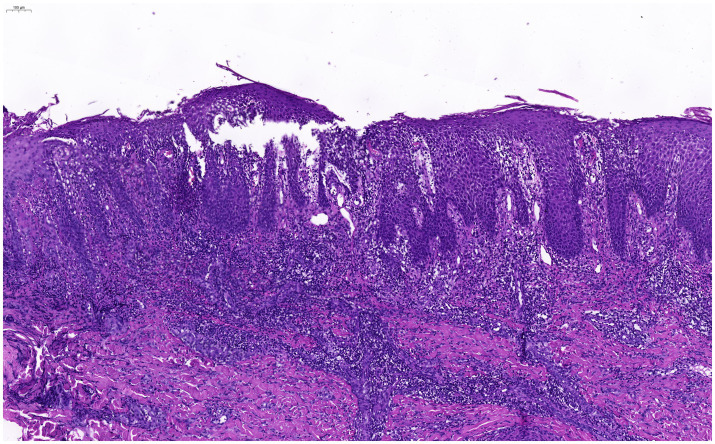 Figure 2
Figure 2| Time point | Clinical and intervention measures | Clinical results and findings |
|---|---|---|
| 40 days ago | Diagnosed with herpes zoster in the left perineum/lower limb, given antiviral treatment. | Herpes zoster lesions healed. |
| 5 days ago | New pruritic rash at the original site. | Eczema occurred. |
| Visit Day (day 0) | Found erythema, papules, and exudation; underwent pathology. | Diagnosed as eczema clinically/pathologically. |
| Days 1–14 | Treated with oral prednisone acetate (30 mg/d) and topical fluticasone propionate cream (twice daily). | Rash improved notably. |
| Days 15 to 3 months | Entered clinical follow-up phase. | Skin lesions resolved completely, no recurrence. |
| Source | Age/sex | Delay | Location | Relapse |
|---|---|---|---|---|
| Our case | 54/F | 4 weeks | Left perineum, groin, and buttocks | No |
| Zijia et al. (2021) ( | 55/F | 6 weeks | Lumbar/abdominal | No |
| Yijun et al. (2018) ( | 74/F | 6 weeks | Left groin | No |
| Ling et al. (2016) ( | 25/M | 4 weeks | Right thoracodorsal region | No |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSkin Diseases and Diabetes · Inflammatory Myopathies and Dermatomyositis · Parvovirus B19 Infection Studies
Introduction
The concept of Wolf’s isotopic response was introduced by Wolf et al. in 1995 and is defined as the development of a secondary disease with distinct characteristics at the same anatomical site following the resolution of the primary condition (1). This report presents a rare case of eczema arising as an isotopic response to herpes zoster infection.
Case reports
A 54-year-old woman presented to our department with a 5-day history of rash and pruritus on the left perineum and left lower limb (for a detailed timeline, see Table 1). She had no personal or family history of atopic diseases. Forty days earlier, she had been diagnosed with herpes zoster affecting the left perineum and left lower limb. Following antiviral treatment, the skin lesions healed. On physical examination, erythematous plaques and papules were observed at the previous site of herpes zoster infection, accompanied by exudation and crusting (Figure 1). Histopathological examination revealed spongiotic dermatitis (Figure 2). Based on the clinical presentation and histopathological findings, a diagnosis of non-specific eczematous dermatitis was established. After 14 days of oral administration of prednisone acetate tablets (30 mg per day) and topical application of fluticasone propionate cream (twice a day), the patient’s rash improved significantly. Three months later, the patient’s eczema did not recur.
Erythema, papules, exudation, and crusting observed on the left perineum (A) and left lower (B) extremity are localized to the previously healed site of a herpes zoster lesion.
Pathological findings indicate the presence of spongiotic changes consistent with spongiotic dermatitis (H&E200×).
Discussion
Wolf’s post-herpetic isotopic response (PHIR) refers to the development of new cutaneous conditions, such as tumors, infections, or immune-mediated diseases, at the site of a previously healed herpetic eruption (2). The exact pathogenesis of Wolf’s PHIR remains incompletely understood. Four hypotheses have been proposed regarding the mechanism of postherpetic inflammatory isomorphic reactions: viral, immunological, vascular, and neurological.
The patient had no history of specific contact with or eczema. Clinical and histopathological findings confirmed eczematous changes, consistent with an isotopic response to prior herpes zoster infection at the same site. We hypothesize that the viral infection may damage A-δ and C nerve fibers in the mid-to-deep dermis, leading to reduced fiber density and the release of neuropeptides from local neural tissues. These neuropeptides include substance P, vasoactive intestinal peptide (VIP), bradykinin, serotonin, calcitonin gene-related peptide (CGRP), and α-melanocyte-stimulating hormone (α-MSH) (3). Studies indicate that substance P can induce mast cells and keratinocytes to release pruritogens via neurokinin 1 receptor activation, potentially activating Mas-related G protein-coupled receptor X2 (MRGPRX2) to trigger mast cell degranulation and pruritus transmission (4). CGRP enhances Th2-mediated immune responses (5). Type 2 inflammatory responses impair skin barrier function by inhibiting filaggrin gene expression and disrupting its reticular structure. The development of pruritus, compromised skin barrier integrity, and enhanced Th2-type immune responses collectively contribute to the onset of eczema.
Currently, cases of eczema secondary to herpes zoster infection are rarely documented in the literature. We reviewed four confirmed cases based on the existing reports. The time intervals between the onset of herpes zoster and the subsequent development of eczema were relatively short, as shown in the data (Table 2). These cases have a high proportion of females in terms of demographics and a wide age range; in terms of time, the delayed onset is mainly at 4 weeks and 6 weeks. The recurrence of erythema, papules, and pustules at the previously healed site of herpes zoster was histopathologically confirmed as eczema. However, such presentations are often misinterpreted as a recurrence of herpes zoster, potentially leading to unnecessary antiviral therapy.
Conclusion
However, this study has several limitations. The diagnosis primarily relies on histopathological examination and clinical presentation, and the causal relationship with the previous herpes infection remains inferential. As a single case report, the generalizability of the conclusions is limited. Although the proposed neuropeptide-mediated immune activation mechanism is supported by the existing literature, it lacks molecular-level validation in this particular case. Therefore, the precise molecular mechanisms underlying this rare phenomenon, particularly the pathway linking neuronal injury, neuropeptide release, and cutaneous inflammation, warrant further elucidation through more extensive basic and clinical research.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wolf R Wolf D Ruocco E Brunetti G Ruocco V. Wolf's isotopic response. Clin Dermatol. (2011) 29:237–40. doi: 10.1016/j.clindermatol.2010.09.015, 21396564 · doi ↗ · pubmed ↗
- 2Ruocco V Ruocco E Brunetti G Russo T Gambardella A Wolf R. Wolf's post-herpetic isotopic response: infections, tumors, and immune disorders arising on the site of healed herpetic infection. Clin Dermatol. (2014) 32:561–8. doi: 10.1016/j.clindermatol.2014.04.003, 25160097 · doi ↗ · pubmed ↗
- 3Liu XY Tan C. Postherpetic granuloma annulare: a Wolf's isotopic response. Med Clin (Barc). (2024) 163:e 109. doi: 10.1016/j.medcli.2024.02.028, 38705791 · doi ↗ · pubmed ↗
- 4Azimi E Reddy VB Pereira PJS Talbot S Woolf CJ Lerner EA. Substance P activates mas-related G protein-coupled receptors to induce itch. J Allergy Clin Immunol. (2017) 140:447–453.e 3. doi: 10.1016/j.jaci.2016.12.980, 28219706 PMC 5546940 · doi ↗ · pubmed ↗
- 5Misery L. Atopic dermatitis and the nervous system. Clin Rev Allergy Immunol. (2011) 41:259–66. doi: 10.1007/s 12016-010-8225-z, 21181506 · doi ↗ · pubmed ↗
- 6Zijia D Ying W Jiachen D Yueting C Guanglian Y Zhenghui Y . Two cases of postherpetic Wolf’s isotopic response. J Diagn Ther Dermatov. (2022) 29:362–5. (in Chinese).
- 7Yijun H Lin L Junlin Z. A case of eczema with infection following herpes zoster with Wolf's isotopic response. Chin J Dermatovenereol Integr Tradit West Med. (2019) 18:476–7. (in Chinese).
- 8Ling F Chengjun C Qifeng S. A case of eczematous changes after herpes zoster with Wolf's isotopic response. Chin J Dermatovenereol. (2016) 30:1089. (in Chinese).