Unexpected Aphonia: A Rare Complication of the Nasopharyngeal Airway (NPA) and Proposed Design Improvements
Akhil P Singh, Deepa Singh, Deepika Chaubey

TL;DR
A patient experienced unexpected loss of voice after a medical procedure, and the paper suggests a design change to prevent such complications.
Contribution
First reported case of prolonged aphonia after NPA use and a proposed design improvement to prevent it.
Findings
Aphonia occurred without respiratory distress after NPA use in a tongue cancer patient.
A design modification is proposed to prevent NPAs from slipping into the nasopharynx or larynx.
Abstract
Patients with airway foreign bodies typically present with difficulty breathing or stridor. Nasopharyngeal airway (NPA)-related complications are rarely reported. We present a case of a patient with carcinoma of the tongue who underwent nasal intubation for surgery using a flexible bronchoscope. This case is unique because the patient experienced prolonged aphonia without respiratory distress, representing a first-of-its-kind report. We also propose a minor modification to the NPA design to reduce the risk of it slipping into the nasopharynx or larynx.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
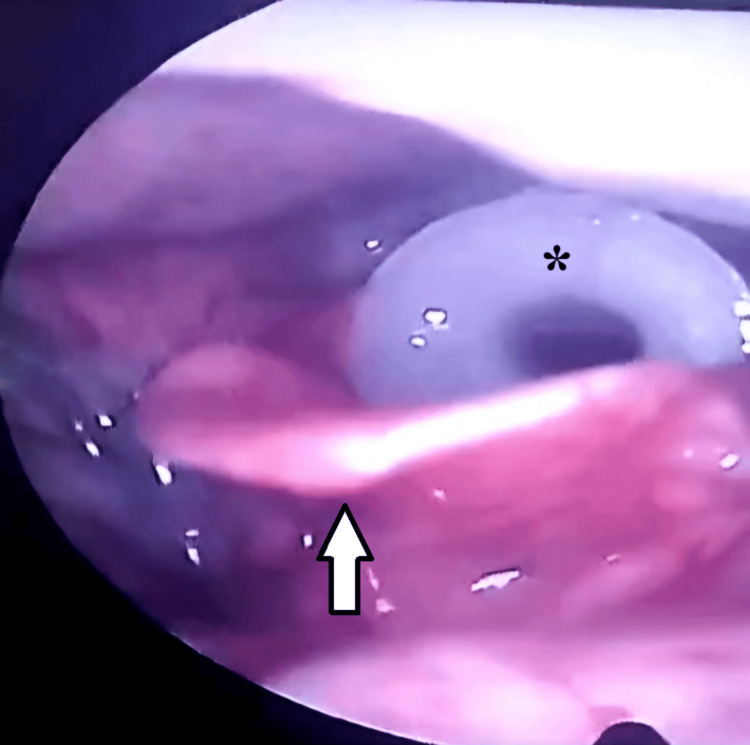 Figure 1
Figure 1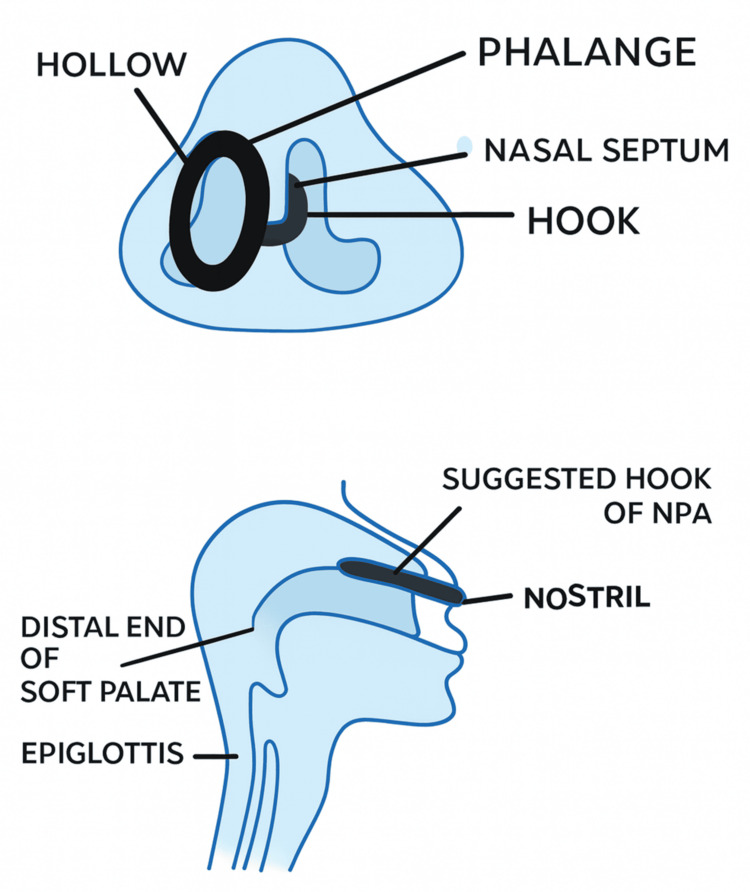 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAirway Management and Intubation Techniques · Tracheal and airway disorders · Foreign Body Medical Cases
Introduction
Foreign bodies in the airway are potential causes of acute and immediate airway obstruction, most commonly presenting with difficulty breathing or stridor [1]. Airway management is a critical consideration in head and neck cancer surgeries due to frequently restricted mouth openings, often necessitating the use of a nasopharyngeal airway (NPA). The NPA is a flexible tube made of soft material, usually silicone or latex, designed to be inserted through the nose into the nasopharynx to prevent or relieve upper airway obstruction and facilitate effective oxygenation and ventilation. NPA-related complications are rare [2-4], and the literature provides limited data, particularly regarding loss of voice as a potential complication. Here, we report a patient who experienced a misplaced NPA.
Case presentation
A 47-year-old male with carcinoma of the tongue underwent hemiglossectomy with supra-omohyoid neck dissection under general anesthesia. Nasal intubation was performed using a transnasal fiberoptic technique to secure the airway during surgery. An NPA was used to facilitate the passage of the flexible bronchoscope through the nasal cavity.
The surgery was uneventful, and the patient was extubated and transferred to the postoperative ward. From postoperative day 1, he reported throat irritation and discomfort, as well as difficulty in vocalization, initially attributed to pain, the presence of a Ryle’s tube, restricted tongue movements, altered tongue architecture, and sequelae of endotracheal intubation. His oxygen saturation remained stable on room air throughout.
The patient was discharged in satisfactory condition on day 5. On postoperative day 12, he returned with fever, chills, and chest pain, along with persistent aphonia. Vocal cord palsy was suspected, and endoscopic examination of the larynx revealed the NPA lodged in the larynx (Video 1).
Video laryngoscopy showing the NPA lodged in the larynxNPA, nasopharyngeal airway
To our surprise, a white plastic cannulated object (NPA) was found lodged in the glottis (Figure 1), persistently irritating the area and preventing the vocal cords from approximating at the midline. An IV dose of antibiotics was administered immediately, and the anesthesia team was consulted. The patient was taken to the operating room, and direct laryngoscopy was performed under sedation. An NPA of 7.5 mm size was removed, providing instant relief from throat discomfort and restoration of normal voice. The patient received two additional IV antibiotic doses over the next 24 hours, after which the chest pain subsided. He was subsequently discharged on a one-week course of oral antibiotics.
Endoscopic view of the larynx showing the NPA in the glottisThe asterisk indicates the NPA, while the white arrow points to the epiglottis.NPA, nasopharyngeal airway
Discussion
During fiberoptic bronchoscopy for nasotracheal intubation, the anesthesia team inadvertently advanced the NPA into the glottis while guiding the endotracheal tube over the bronchoscope. The NPA’s flange became lodged above the vocal folds, while its hollow tube slipped down toward the trachea. The NPA prevented the vocal folds from approximating, resulting in aphonia, which resolved immediately after removal of the device. The patient also aspirated oral secretions, leading to a secondary chest infection. Respiratory complications following NPA placement have rarely been reported [5-8]. Loss of voice as a complication of NPA has not been documented previously, making this the first case report to describe such an occurrence. Postoperative voice loss is generally classified as either direct (traumatic intubation) or indirect (desiccation of the vocal fold mucosa due to inhaled anesthetic gases) [9]. Inomata et al. described a case of temporary bilateral vocal cord paralysis associated with laryngeal mask airway placement [10].
In light of this case, we propose a modification to the NPA design (Figure 2) to reduce the risk of accidental slippage into the nasopharynx and upper aerodigestive tract. Adding a sharply curved hook to the NPA flange, designed to rest in the opposite nasal cavity, would anchor the device against the nasal septum and prevent displacement.
Proposed design modification for the NPANPA, nasopharyngeal airway
Conclusions
Given the frequent use of NPAs during airway management and intubation, we recommend improved communication between anesthesia and surgical teams. It is also advisable to count NPAs before and after surgery, similar to surgical gauze, to prevent accidental misplacement. Modifications to the NPA design could reduce the risk of accidental slippage into the nasopharynx and upper aerodigestive tract. Affixing a sharply curved hook to the NPA’s flange would not only prevent inward displacement but also serve as a visual reminder to both the anesthetist and surgeon of its presence in the nasal cavity. Additionally, postoperative endoscopic examination of the larynx is strongly recommended, even if the patient reports only minor throat discomfort.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Foreign body airway obstruction Stat Pearls [Internet] Dodson H Sharma S Cook J Treasure Island (FL)Stat Pearls Publishing 2025 https://pubmed.ncbi.nlm.nih.gov/31985979/31985979 · pubmed ↗
- 2Bilateral vocal cord paralysis secondary to head and neck surgery J Craniofac Surg Tekin M Acar GO Kaytaz A Savrun FK Çelik M Cam OH 1351372320122233739010.1097/SCS.0b 013e 3182413 d 71 · doi ↗ · pubmed ↗
- 3Voice loss following endotracheal intubation: the anesthesiologist's dilemma Airway Kotekar N Vyshnavi S 576322019
- 4The nasopharyngeal airway: dispelling myths and establishing the facts Emerg Med J Roberts K Whalley H Bleetman A 3943962220051591194110.1136/emj.2004.021402 PMC 1726817 · doi ↗ · pubmed ↗
- 5Intracranial placement of nasopharyngeal airways: is it all that rare?Emerg Med J Ellis DY Lambert C Shirley P 66123200610.1136/emj.2006.036541 PMC 256418516858116 · doi ↗ · pubmed ↗
- 6Middle turbinectomy as a complication of nasopharyngeal airway placement Am J Emerg Med Zwank M 51351427200910.1016/j.ajem.2008.09.03819555632 · doi ↗ · pubmed ↗
- 7One notable complication of nasopharyngeal airway: a case report Clin Pract Cases Emerg Med Briggs B Countryman C Mc Ginnis HD 584586420203321727810.5811/cpcem.2020.8.48811 PMC 7676774 · doi ↗ · pubmed ↗
- 8Retained nasal trumpet for 20 months: an unusual foreign body JAMA Otolaryngol Head Neck Surg Kim BJ Shoffel-Havakuk H Johns MM 3rd 939414520193045251310.1001/jamaoto.2018.2939 · doi ↗ · pubmed ↗