A black macule on the male nipple
Noriyoshi Fujii, Akemi Fukuda, Nozomi Kawahara, Keiko Kobayashi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
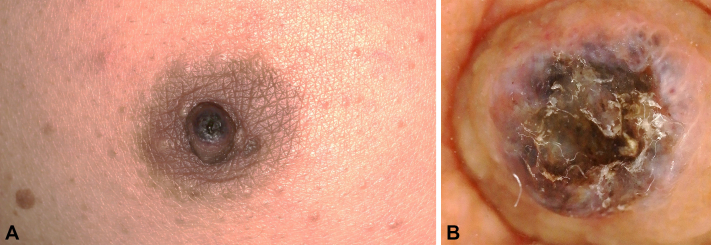 Figure 1
Figure 1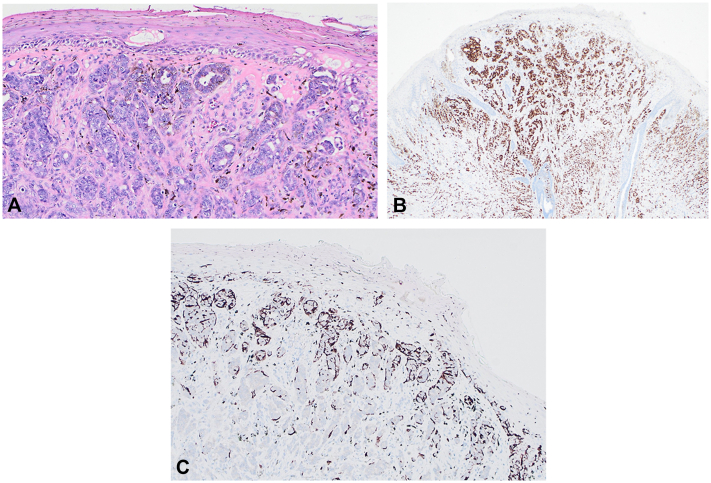 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer and Skin Lesions · Male Breast Health Studies · Vascular Tumors and Angiosarcomas
Case presentation
A 55-year-old man with no significant medical history presented with a 2-month history of a pigmented macule and intermittent scaling on the right nipple–areola complex (Fig 1, A). He denied pain, discharge, bleeding, fever, weight loss, and trauma. Examination revealed a well-demarcated 5 × 5 mm dark macule with a thin adherent crust; no subareolar mass or axillary lymphadenopathy was detected. Dermoscopy showed blue-gray globules and irregular dark dots with central surface erosion/ulceration; arborizing vessels were not clearly identified (Fig 1, B). Baseline laboratory tests (including carcinoembryonic antigen and cancer antigen 15-3) and axillary ultrasonography were unremarkable. A complete excisional biopsy was performed in a circular manner with 2-mm clinical margins, including full-thickness dermis to the superficial subcutis.Fig 1A, 5 × 5 mm black macule with thin crust on the right nipple–areola complex. B, Dermoscopy: blue-gray globules and irregular dark dots with central surface erosion/ulceration; no clear arborizing vessels.
Histopathology shows a superficial crust with focal basal vacuolar alteration and, beneath it, a dermal cellular proliferation with nested/cord-like architecture, accompanied by dendritic melanocytes and melanin-laden melanophages (Fig 2, A). Immunostains for estrogen receptor (Fig 2, B) and Melan-A (Fig 2, C) are provided for clinicopathologic correlation.Fig 2A, H&E: superficial crust over dermal nests/cords; dendritic melanocytes and melanophages. B, ER immunohistochemistry: strong nuclear staining. C, Melan-A immunohistochemistry: dendritic melanocytes around nests. ER, Estrogen receptor; H&E, hematoxylin and eosin.
Question: What is the most likely diagnosis for this patient?
- **A.**Pigmented nodular basal cell carcinoma
- **B.**Pigmented eccrine porocarcinoma
- **C.**Nodular malignant melanoma
- **D.**Invasive ductal carcinoma
- **E.**Pigmented mammary Paget disease
Answer discussion
The correct answer is D.
Male breast cancer is an uncommon entity, representing approximately 1% of all breast malignancies.1 It most frequently arises in the central retroareolar region, often involving the nipple.1 Clinically, a painless mass is the typical presentation; pigmented epidermal change is exceedingly rare, and overall management generally mirrors that in women.1 When pigmentation is present, bedside impression may resemble melanoma or basal cell carcinoma, and reported male cases describe deceptive dermoscopic patterns—including blue-gray areas, blue-white structures, and occasionally corkscrew vessels—supporting biopsy of even small pigmented nipple lesions.2^,^3
The patient in this case had a small, sharply demarcated black macule with blue-gray structures and central surface erosion on dermoscopy, features that can confound clinical judgment. The lesion was excised circularly with a narrow 2-mm margin to secure diagnostic accuracy, consistent with melanoma biopsy recommendations, while minimizing cosmetic deformity of the nipple–areola complex. Histopathology revealed a predominantly dermal tubule-forming epithelial neoplasm with minimal epidermal involvement, absence of Paget cells, or pagetoid spread, leading to a diagnosis of invasive ductal carcinoma. Immunohistochemically, tumor nuclei demonstrated strong estrogen receptor positivity. Notably, Melan-A failed to stain the neoplastic cells, instead highlighting dendritic melanocytes at the periphery of carcinoma nests. These findings support a diagnosis of a nonmelanocytic malignancy with secondary pigmentation, as opposed to primary melanoma or pigmented mammary Paget disease.
The most plausible basis for pigmentation is melanocyte colonization: disruption of the dermoepidermal junction permits epidermal melanocytes to migrate into and around carcinoma nests and transfer melanin via dendritic processes to adjacent tumor cells, producing intracellular melanin.4 Paracrine signaling is also likely to contribute, as breast carcinoma can express basic fibroblast growth factor, which promotes melanocyte migration and proliferation.5 In male patients with a pigmented nipple macule, integration of dermoscopy, histopathology, and immunohistochemistry is indispensable to prevent diagnostic errors and to facilitate timely definitive therapy.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Giordano S.H.Breast cancer in men N Engl J Med 3782420182311232010.1056/NEJ Mra 170793929897847 · doi ↗ · pubmed ↗
- 2Yanagishita T.Tamada Y.Tanaka M.Pigmented mammary Paget disease mimicking melanoma on dermatoscopy J Am Acad Dermatol 6462011 e 114e 11610.1016/j.jaad.2010.09.71721571155 · doi ↗ · pubmed ↗
- 3Takizawa K.Yamamoto Y.Kiyohara T.Pigmented male breast carcinoma: dermoscopic features and histopathological correlation Australas J Dermatol 5832017 e 117e 11910.1111/ajd.12671 · doi ↗
- 4Azzopardi J.G.Eusebi V.Melanocyte colonization and pigmentation of breast carcinoma Histopathology 111977213010.1111/j.1365-2559.1977.tb 01641.x 615831 · doi ↗ · pubmed ↗
- 5Konomi K.Imayama S.Nagae S.Terasaka R.Chijiiwa K.Yashima Y.Melanocyte chemotactic factor produced by skin metastases of a breast carcinoma J Surg Oncol 5011992626610.1002/jso.29305001171573897 · doi ↗ · pubmed ↗