Amplitude-Integrated/Continuous Electroencephalography for Early Detection of Low Cardiac Output After Chest Closure in an Infant
Alessandro Barbaria, Mariarita Capizzi, Federica Sperandeo, Gloria Castelli, Giuseppe Isgrò, Tommaso Aloisio, Angela Satriano, Alessandro Giamberti, Massimo Mastrangelo, Marco Ranucci

TL;DR
Amplitude-integrated/continuous EEG can detect early signs of low cardiac output in infants, even when other monitoring appears normal.
Contribution
This case demonstrates aEEG/cEEG's potential to identify cerebral compromise from LCOS earlier than conventional methods.
Findings
aEEG/cEEG showed early EEG abnormalities before clinical signs of LCOS recurrence.
Cerebral distress was resolved after chest reopening, confirming aEEG/cEEG's predictive value.
Standard monitoring failed to detect LCOS despite aEEG/cEEG showing early signs.
Abstract
Weaning from cardiopulmonary bypass in pediatric cardiac surgery is challenging, especially after prolonged procedures. Delayed chest closure may be necessary in cases of low cardiac output syndrome (LCOS) to support hemodynamic recovery. Although near-infrared spectroscopy is standard for neuromonitoring, amplitude-integrated electroencephalography (aEEG) and continuous electroencephalography (cEEG) are emerging tools. We report the case of a 6-month-old infant with transposition of the great arteries who required delayed chest closure after surgical repair. LCOS recurred after chest closure on postoperative day 3 despite stable near-infrared spectroscopy values. Retrospective aEEG/cEEG analysis, unintentionally initiated before closure, showed early EEG abnormalities preceding clinical signs, which were resolved after chest reopening. This case highlights the potential of aEEG/cEEG…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
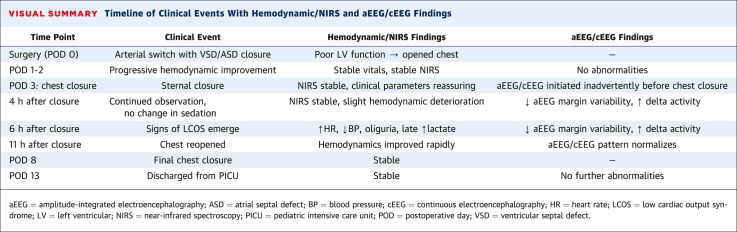 Figure 1
Figure 1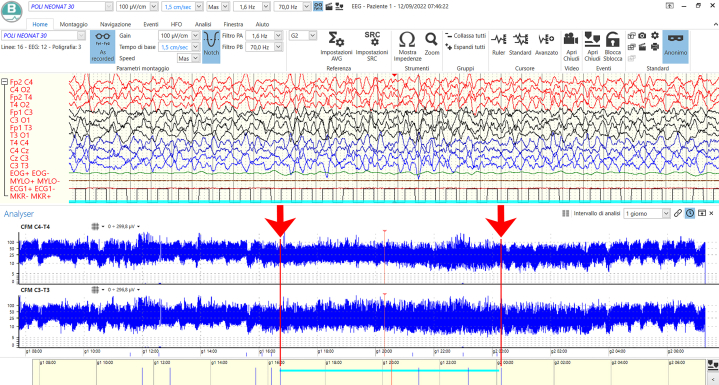 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrest and Resuscitation · Congenital Heart Disease Studies · Mechanical Circulatory Support Devices
Weaning from cardiopulmonary bypass in pediatric cardiac surgery can be challenging. Prolonged bypass time to repair complex congenital heart disease (CHD) heightens the risk of low cardiac output syndrome (LCOS) owing to myocardial dysfunction, systemic inflammation, and hemodynamic instability. Although standard management includes pharmacological support, fluid optimization, and, in severe cases, extracorporeal life support such as extracorporeal membrane oxygenation,1 delayed chest closure is a widely recognized strategy in facilitating successful weaning. Delayed chest closure is particularly beneficial in neonates and infants by mitigating the adverse effects of myocardial edema, diastolic dysfunction, excessive bleeding, and reduced pulmonary compliance.2
Accurate assessment of cardiac output, systemic oxygen delivery, and tissue oxygenation is crucial for optimizing hemodynamics and guiding the timing of chest closure, as an increase in intrathoracic pressure may elevate afterload, potentially impairing the cardiac output. In the pediatric intensive care unit, cardiac output is typically assessed using clinical evaluation and hemodynamic parameters, including heart rate, invasive arterial pressure, and right atrial pressure. However, studies have shown that these measures may not reliably reflect true physiological status, highlighting the potential for discrepancies between clinical assessment and actual hemodynamic parameters.3 Of note, direct measurement of cardiac output using a pulmonary artery catheter is not feasible in neonates owing to anatomical limitations.
Neonates with CHD have been identified as being at high risk for acute brain injury.4 For this reason, neuromonitoring with near-infrared spectroscopy (NIRS) and amplitude-integrated electroencephalogram (aEEG) combined with continuous electroencephalogram (cEEG) has become widely used.5 Cerebral NIRS measures regional oxygen saturation, serving as an indirect indicator of oxygen extraction in the underlying brain tissue (typically the frontal cortex). However, NIRS provides only relative measurements, making it most effective for monitoring trends rather than providing absolute values.6 Neuromonitoring with aEEG/cEEG has become widely adopted.7 The main indication is to assess both the background activity and the burden of electrographic seizures in patients with increased risk of abnormal neurologic outcome, as for example in neonates with CHD.8 In particular, aEEG has emerged as a straightforward bedside tool for continuous monitoring of cerebral electrical activity, with interpretations accessible even to nonneurology physicians. A recent prospective observational study9 demonstrated that early postoperative EEG background abnormalities in neonates undergoing cardiac surgery strongly correlated with brain lesions on magnetic resonance imaging and predicted adverse neurodevelopmental outcomes. Importantly, EEG patterns were predictive even in the absence of overt clinical signs or significant NIRS abnormalities.
Cerebral electrical activity is closely linked to cerebral oxygen delivery, which depends on optimal cardiac output and sufficient arterial pressure to ensure adequate cerebral blood flow. Of note, although continuous cerebral NIRS assessment is considered the gold standard in the setting of advance hemodynamic monitoring, the role of EEG as a surrogate parameter of cardiac performance is unknown. The aims of this case report are: 1) to demonstrate the occurrence of aEEG/cEEG background abnormalities closely associated with chest closure, with subsequent recovery after chest reopening; 2) to highlight that aEEG/cEEG alterations precede other clinical signs of LOCS; and 3) to explore the potential role of aEEG in the early detection of LCOS.
History of Presentation
We report the case of a 6-month-old male infant, born full-term via eutocic delivery without significant perinatal complications. At 2 months of age, he developed dyspnea and polypnea during feeding, accompanied by poor weight growth. A cardiologic evaluation was performed, leading to a diagnosis of complex CHD, including transposition of the great arteries, ventricular septal defect, pulmonary stenosis, and pulmonary hypertension. Given these findings, hospitalization was recommended for corrective heart surgery.
Investigations
On admission, the patient's examination revealed a weight of 6,105 g and a height of 67 cm. Vital signs included a blood pressure of 107/53 mm Hg, heart rate of 150 beats/min, and oxygen saturation of 85% on room air. The electrocardiogram revealed sinus rhythm with a heart rate of 150 beats/min and normal interventricular conduction. Echocardiography (Video 1) revealed situs solitus, levocardia, and atrioventricular concordance with ventriculoarterial discordance; a large atrial septal defect with low-velocity left-to-right shunt, and a large muscular ventricular septal defect with nonrestrictive right ventricle–pulmonary artery flow; a dilated, hypertrophic right ventricle with preserved function and moderate tricuspid regurgitation due to annular dilation; a normal-sized left ventricle with preserved systolic function; unobstructed right ventricular outflow tract, continent tricuspid aortic valve, and normal coronary origins; and mild left ventricle–pulmonary artery flow acceleration and pulmonary regurgitation indicating overflow, with elevated mean pulmonary pressure (58 mm Hg) and dilated pulmonary branches.
Management
After medical stabilization, the patient underwent surgical repair with arterial switch, atrial septal defect closure, and ventricular septal defect closure with heterologous pericardial patch and patent ductus arteriosus ligation (Video 2).
He was weaned off cardiopulmonary bypass with open chest and inotropic support (adrenaline) because of severe left ventricular disfunction. Monitoring in the pediatric intensive care unit was performed as usual in our center: electrocardiogram, invasive arterial pressure, central venous pressure, NIRS, peripheral oxygen saturation, and urinary catheter. Moreover, advanced neuromonitoring with cEEG (with electrodes placed according to the International 10-20 Reduced System for Neonates) and aEEG was positioned, according to the INNESCO (Italian Neonatal Seizure Collaborative Group) guidelines. After admission, inotropic support was improved with milrinone and levosimendan. Adequate sedation was maintained with continuous infusion of fentanyl and midazolam, and continuous neuromuscular blockade was administered as well. Over the following days, a gradual improvement in hemodynamic status was observed, as indicated by stable vital parameters and consistent NIRS values, accompanied by a reduction in the requirement for pharmacological inotropic support. The improvement led to chest closure on postoperative day 3. Six hours after closing the chest, the patient started developing signs of low cardiac output, with a progressive worsening of hemodynamics (tachycardia, shift from sinus rhythm to junctional rhythm, hypotension) and oliguria-anuria, which led to augmented inotropic support. A late increase in lactates was registered at the arterial blood gas. Notably, there was no modification in cerebral NIRS (Table 1). Eleven hours after chest closure, according to the cardiac surgeon, the chest was reopened, with a consequential improvement in clinical conditions.Table 1. Monitoring Parameters in the Pediatric Intensive Care Unit During Chest Closure and ReopeningTime8:0010:0012:0014:0016:0018:0020:0022:0023:3024:002:004:006:00Right cerebral NIRS (%)7978Chest closure8278758377Chest reopening81726972Left cerebral NIRS (%)8283657267737195939592Internal temperature (°C)37.337.73737383940.439.238.43838.1RhythmPMPMSRJRJRJRJRPMPMPMPMHeart rate (beats/min)150156163174176184199152154150149Systolic BP (mm Hg)8476697780868562769795Diastolic BP (mm Hg)4545394139404035455453CVP (mm Hg)1111131313111110101010ScvO_2_ (%)8786818372727463748280SpO_2_ (%)10010099100939595100100100100Urinary output (mL/Kg/h)1.671.250.832.90.830.830.421.52.11.670.83Lactates (mmol/L)0.88—1.71.32.933.652.752.03——SvO_2_ (%)——56——6770————BP = blood pressure; CVP = central venous pressure; JR = junctional rhythm; PM = pacemaker; NIRS = near-infrared spectroscopy; ScvO_2_ = venous oxygen saturation (PediaSat); SpO_2_ = peripheral oxygen saturation; SR = sinus rhythm; SvO_2_ = venous oxygen saturation.
On the same day, aEEG and cEEG monitoring were inadvertently initiated and continued because of a misunderstanding between the attending physician and the neurophysiology technician, resulting in an unintentional deviation from our protocol, which typically excludes EEG during chest closure for logistical and aseptic reasons; this allowed for the unexpected recording of perioperative cerebral activity. The recording was analyzed and turned out to be particularly significant. At the onset of the recording (Supplemental Figure 1A), the aEEG traces displayed a continuous pattern with good variability in both the lower and upper margins, whereas the cEEG pattern was characterized by continuous theta-delta activity intermingled with superimposed, pharmacologically related fast activity. Four hours after chest closure (Figure 1), aEEG analysis revealed a loss of variability in both margins. Concurrently, the cEEG pattern showed bilateral background slowing (predominantly anterior) associated with high-voltage delta activity and a disappearance of fast activity. This pattern persisted for 9 hours, suggesting diffuse cerebral dysfunction. One hour after sternal reopening (Supplemental Figure 1B), both aEEG and cEEG gradually returned to a reactive and variable baseline pattern. No changes in sedative drug dosing were made during the neuromonitoring period, minimizing pharmacological influence on the observed EEG changes.Figure 1. Continuous 23-Hour and 30-Minute Recording of Combined aEEG and cEEG Monitoring in a Patient After Delayed Chest ClosureThe upper panel displays the raw cEEG signal, while the lower panel shows bilateral aEEG traces (C4-T4 and C3-T3). At 16:24 (left arrow), a clear change in aEEG background is observed, with loss of both upper and lower margin variability, indicative of background suppression. Concurrently, the cEEG shows bilateral high-voltage delta activity (up to 200 μV), most prominent in the anterior regions, with disappearance of faster frequencies. This altered pattern persists until 00:05 (right arrow), suggesting diffuse cerebral dysfunction. The synchronization bar at 20:19:06 (8 hours after chest closure) marks the onset of background slowing on the raw cEEG trace. aEEG = amplitude-integrated electroencephalography; cEEG = continuous electroencephalography.
Outcome and Follow-Up
The patient's chest was definitively closed on postoperative day 8. No other significant aEEG/cEEG alterations were registered on subsequent analyses. The patient was dismissed from the pediatric intensive care unit on postoperative day 13.
Discussion
This case highlights the potential of aEEG combined with cEEG as a sensitive, noninvasive bedside tool for early detection of cerebral compromise secondary to LCOS in infants after complex congenital heart surgery. The use of aEEG/cEEG monitoring in this case (albeit initiated inadvertently) allowed for retrospective analysis and revealed a clear deterioration in cerebral electrical activity, with loss of normal cyclicity and emergence of a low-frequency, high-amplitude delta pattern. These findings resolved promptly upon chest reopening, underscoring the direct relationship between impaired cardiac output and cerebral function. This case report underscores a critical, often under-recognized, vulnerability during the postoperative course of infants recovering from cardiac surgery: The potential for sternal closure to induce acute hemodynamic compromise, even when other parameters appear stable. It also emphasizes the value of multimodal neuromonitoring, particularly the complementary role of aEEG alongside NIRS, in detecting early cerebral distress.
In the presented scenario, aEEG alterations anticipated the clinical and hemodynamic signs of LCOS that developed after delayed chest closure, despite stable cerebral NIRS values. This dissociation suggests that aEEG may detect subtle changes in cerebral function linked to impaired oxygen delivery before they are reflected in more conventional monitoring modalities.Visual SummaryTimeline of Clinical Events With Hemodynamic/NIRS and aEEG/cEEG FindingsTime PointClinical EventHemodynamic/NIRS FindingsaEEG/cEEG FindingsSurgery (POD 0)Arterial switch with VSD/ASD closurePoor LV function → opened chest—POD 1-2Progressive hemodynamic improvementStable vitals, stable NIRSNo abnormalitiesPOD 3: chest closureSternal closureNIRS stable, clinical parameters reassuringaEEG/cEEG initiated inadvertently before chest closure4 h after closureContinued observation, no change in sedationNIRS stable, slight hemodynamic deterioration↓ aEEG margin variability, ↑ delta activity6 h after closureSigns of LCOS emerge↑HR, ↓BP, oliguria, late ↑lactate↓ aEEG margin variability, ↑ delta activity11 h after closureChest reopenedHemodynamics improved rapidlyaEEG/cEEG pattern normalizesPOD 8Final chest closureStable—POD 13Discharged from PICUStableNo further abnormalitiesaEEG = amplitude-integrated electroencephalography; ASD = atrial septal defect; BP = blood pressure; cEEG = continuous electroencephalography; HR = heart rate; LCOS = low cardiac output syndrome; LV = left ventricular; NIRS = near-infrared spectroscopy; PICU = pediatric intensive care unit; POD = postoperative day; VSD = ventricular septal defect.Equipment ListaEEG/cEEG for early detection of LCOS after chest closure in an infant following cardiac surgery Device used for newborn/infant EEG video-registration • BRAIN QUICK® Clinical EEG Video Equipment Software for aEEG/cEEG analysis • Software version 1.02.02, “Micromed Group S.p.A.”, Rev. 6.0
Conclusions
Despite its potential, the role of aEEG as a surrogate marker of cardiac performance remains poorly explored in the current literature, particularly in the context of postoperative LCOS. Incorporating aEEG into standard postoperative monitoring protocols, especially in high-risk patients or during critical transitions such as chest closure, may enhance clinical decision-making and improve outcomes. Further research is warranted to validate the predictive value of aEEG in this context. We are currently developing a prospective observational study to investigate the role of early aEEG/cEEG monitoring in infants undergoing chest closure after cardiac surgery.
Funding Support and Author Disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.Take-Home Messages
- •Amplitude-integrated EEG can detect early cerebral dysfunction due to low cardiac output before clinical or hemodynamic signs emerge, even when near-infrared spectroscopy values remain unchanged.
- •Routine integration of amplitude-integrated EEG into postoperative monitoring may enhance early recognition of low cardiac output syndrome and guide timely interventions in high-risk pediatric cardiac patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Varrica A.Cotza M.Rito M.L.Post cardiotomy extracorporeal membrane oxygenation in pediatric patients: results and neurodevelopmental outcomes Artif Organs 481220241525153510.1111/aor.1484239152646 · doi ↗ · pubmed ↗
- 2Kanakis M.Samanidis G.Kolovou K.Outcomes of delayed chest closure after congenital heart surgery in neonates Pediatr Med Chir 461202410.4081/pmc.2024.32838389487 · doi ↗ · pubmed ↗
- 3Tibby S.M.Hatherill M.Marsh M.J.Murdoch I.A.Clinicians' abilities to estimate cardiac index in ventilated children and infants Arch Dis Child 776199751651810.1136/adc.77.6.5169496187 PMC 1717412 · doi ↗ · pubmed ↗
- 4Ortinau C.M.Smyser C.D.Arthur L.Optimizing neurodevelopmental outcomes in neonates with congenital heart disease Pediatrics 150Suppl 22022 e 2022056415 L 10.1542/peds.2022-056415 LPMC 1043501336317967 · doi ↗ · pubmed ↗
- 5Pardo A.C.Carrasco M.Wintermark P.Newborn Brain Society, Guidelines and Publications Committee Neuromonitoring practices for neonates with congenital heart disease: a scoping review Pediatr Res 9720251492150610.1038/s 41390-024-03484-x 39183308 PMC 12119335 · doi ↗ · pubmed ↗
- 6Bronicki R.A.Chang A.C.Management of the postoperative pediatric cardiac surgical patient Crit Care Med 39820111974198410.1097/CCM.0b 013e 31821 b 82a 621768801 · doi ↗ · pubmed ↗
- 7Wusthoff C.J.Numis A.L.Pressler R.M.The American clinical neurophysiology society guideline on indications for continuous electroencephalography monitoring in neonates J Clin Neurophysiol 421202511110.1097/WNP.000000000000112039752571 · doi ↗ · pubmed ↗
- 8El-Naggar W.I.Keyzers M.Mc Namara P.J.Role of amplitude-integrated electroencephalography in neonates with cardiovascular compromise J Crit Care 252201031732110.1016/j.jcrc.2008.11.00819327328 · doi ↗ · pubmed ↗