Clinical and Genotypic Features of Norovirus Enteritis in Children Complicated by Convulsions: A Retrospective Study in Kunming, China
Suqi Xu, Mingying Wang, Canchun Zhao, Jiahui Fang, Shumei He, Zhuoheng Li, Haoyu Ma, Qiangming Sun, Hongchao Jiang

TL;DR
This study explores the clinical and genetic features of norovirus enteritis in children who experience convulsions, identifying risk factors and genotypes in Kunming, China.
Contribution
The study provides new insights into the molecular epidemiology and clinical risk factors of norovirus enteritis complicated by convulsions.
Findings
Elevated serum CK-MB levels and fever are independent risk factors for convulsions in NoVE patients.
Lower frequency of diarrhea acts as a protective factor against convulsions in NoVE.
GII.4 genotype is the most prevalent in both NoVE and NoVE with convulsion groups.
Abstract
Although studies have described the clinical characteristics of norovirus enteritis (NoVE) associated with convulsions, research on its molecular epidemiology remains limited. Therefore, this study aimed to investigate both the clinical manifestations and genotypic features of NoVE complicated by convulsions. NoVE children admitted to our hospital between November 2021 and May 2022 were divided into NoVE complicated with convulsion group and NoVE group. Then, we screened the risk factors of NoVE complicated with convulsion based on multivariate regression analysis. The stool samples were collected, followed by amplification of VP1 sequences of GI and GII and phylogenetic analysis of VP1 in both groups. Logistic regression analysis showed that elevated serum CK‐MB levels and fever were independent risk factors for convulsions in NoVE patients, while a lower frequency of diarrhea was an…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
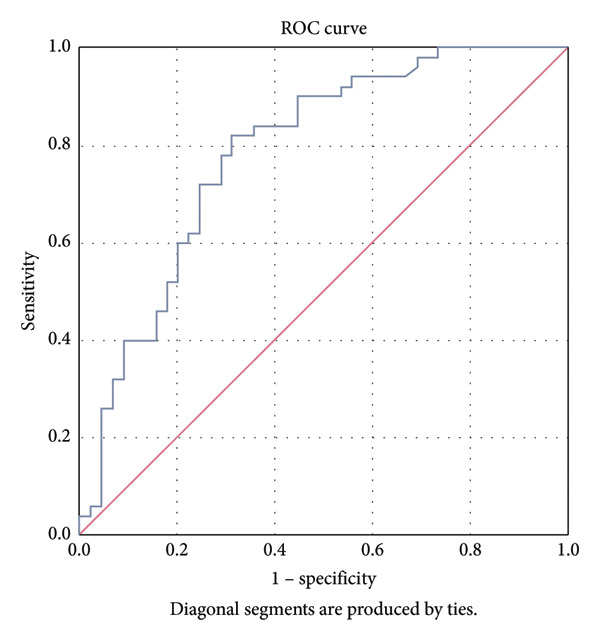 Figure 1
Figure 1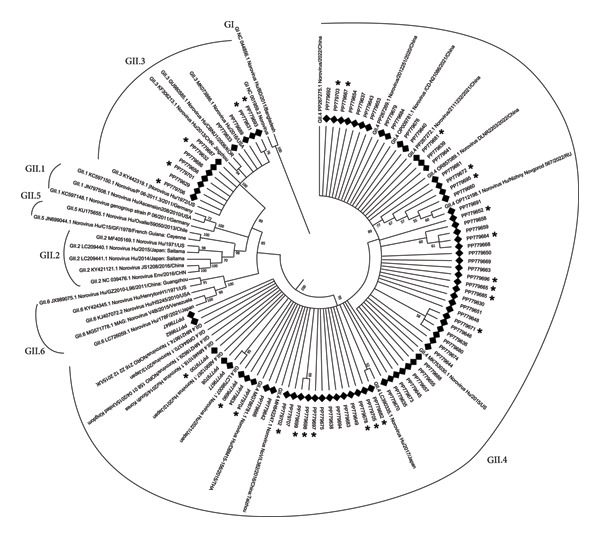 Figure 2
Figure 2| Variable | NoVE combined with convulsion group ( | NoVE group ( |
|
|
|---|---|---|---|---|
| Gender | 1.799 | 0.180 | ||
| Male | 22 (44.0%) | 26 (57.8%) | ||
| Female | 28 (56.0%) | 19 (42.2%) | ||
| Age | 9.021 | 0.011 | ||
| < 12 months | 4 (8.0%) | 12 (26.7%) | ||
| 12–36 months | 45 (90.0%) | 29 (64.4%) | ||
| > 36 months | 1 (2.0%) | 4 (8.9%) | ||
| Allergy | 2.887 | 0.089 | ||
| Yes | 4 (8.0%) | 9 (20.0%) | ||
| No | 46 (92.0%) | 36 (80.0%) | ||
| RV vaccination | 1.090 | 0.297 | ||
| Vaccinated | 7 (14.0%) | 10 (22.2%) | ||
| Nonvaccinated | 43 (86.0%) | 35 (77.8%) | ||
| Birth weight | 0.018 | 0.892 | ||
| Low birth weight | 6 (12.0%) | 5 (11.1%) | ||
| Normal weight | 44 (88.0%) | 40 (88.9%) | ||
| Preterm birth | 0.038 | 0.845 | ||
| Yes | 6 (12.0%) | 6 (13.3%) | ||
| No | 44 (88.0%) | 39 (86.7%) | ||
| Type of delivery | 0.007 | 0.931 | ||
| Vaginal delivery | 26 (52.0%) | 23 (51.1%) | ||
| Cesarean section | 24 (48.0%) | 22 (48.9%) | ||
| Rescue | < 0.001 | 1.000 | ||
| Yes | 10 (20.0%) | 9 (20.0%) | ||
| No | 40 (80.0%) | 36 (80.0%) | ||
| Fever | 17.504 | < 0.001 | ||
| Yes | 39 (78.0%) | 16 (35.6%) | ||
| No | 11 (22.0%) | 29 (64.4%) | ||
| Dehydration | 0.786 | 0.375 | ||
| Yes | 6 (12.0%) | 3 (6.7%) | ||
| No | 44 (88.0%) | 42 (93.3%) | ||
| Diarrhea | 4.00 (3.00, 6.00) | 6.00 (3.00, 10.00) | −2.597 | 0.009 |
| Vomiting | 4.00 (2.75, 7.00) | 6.00 (3.00, 10.00) | −1.643 | 0.100 |
| ALT | 23.00 (18.50, 28.50) | 23.00 (17.00, 41.00) | −0.023 | 0.982 |
| AST | 48.00 (41.00, 58.50) | 47.00 (37.50, 57.50) | −0.470 | 0.639 |
| BUN | 4.42 (2.37, 5.84) | 2.91 (1.70, 4.56) | −2.258 | 0.024 |
| Cr | 21.27 (18.29, 24.78) | 20.85 (18.00, 24.97) | −0.481 | 0.630 |
| CK | 96.00 (62.75, 187.75) | 57.00 (38.50, 97.00) | −3.675 | < 0.001 |
| CK‐MB | 35.00 (26.75, 44.00) | 27.00 (20.00, 37.50) | −2.726 | 0.006 |
| LDH | 258.50 (226.75, 302.00) | 275.00 (240.00, 337.00) | −1.469 | 0.142 |
| LDH‐MB | 67.50 (60.75, 78.00) | 61.00 (56.00, 74.00) | −2.114 | 0.034 |
| α‐HBDH | 199.00 (177.75, 227.25) | 201.00 (177.00, 241.50) | −0.037 | 0.970 |
| Na+ | 136.85 (135.25, 138.00) | 138.00 (137.00, 140.10) | −3.209 | 0.001 |
| K+ | 4.35 ± 0.44 | 4.43 ± 0.63 | −0.776 | 0.440 |
| Ca2+ | 2.49 ± 0.13 | 2.44 ± 0.13 | 1.605 | 0.112 |
| Mg2+ | 0.80 (0.75, 0.86) | 0.88 (0.80, 0.92) | −3.552 | < 0.001 |
| Glu | 4.00 (3.63, 4.52) | 3.90 (3.60, 4.40) | −0.567 | 0.571 |
| WBC | 7.07 (5.62, 8.80) | 7.32 (6.12, 12.50) | −1.483 | 0.138 |
| CRP | 1.01 (0.50, 5.50) | 0.54 (0.50, 2.38) | −1.020 | 0.308 |
| PCT | 0.24 (0.24, 0.24) | 0.24 (0.24, 0.28) | −0.868 | 0.385 |
| ESR | 2.00 (2.00, 3.00) | 2.00 (2.00, 6.00) | −2.169 | 0.030 |
| IgG | 5.05 ± 1.18 | 4.72 ± 1.55 | 1.117 | 0.267 |
| IgA | 0.29 (0.17, 0.47) | 0.37 (0.26, 0.66) | −1.932 | 0.053 |
| CD3 | 66.44 ± 6.90 | 62.05 ± 9.30 | 2.064 | 0.044 |
| CD4/CD8 | 2.35 (1.76, 2.84) | 2.05 (1.68, 2.91) | −1.181 | 0.238 |
| Variables |
| Standard error | Wald |
| OR value | 95% CI |
|---|---|---|---|---|---|---|
| CK‐MB | 0.075 | 0.033 | 5.205 | 0.023 | 1.077 | 1.011–1.149 |
| Fever | 3.567 | 1.225 | 8.478 | 0.004 | 35.415 | 3.209–390.846 |
| Less diarrhea frequency | −0.602 | 0.237 | 6.481 | 0.011 | 0.548 | 0.344–0.871 |
| Genotype | NoVE samples ( | NoVE + convulsion samples ( |
|
|---|---|---|---|
| GII.3 | 12 (14.81%) | 5 (15.19%) | 1.00 |
| GII.4 | 69 (85.19%) | 28 (84.85%) |
- —Xingdian Talent Support Program for Medical and Health Talents Project
- —Kunming Research Center for Pathogen Identification and Pathogenic Mechanism for Emerging and Unknown Infectious Diseases in Children
- —Kunming Science and Technology Plan Project
- —Kunming Health Commission
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral gastroenteritis research and epidemiology · Virus-based gene therapy research · Clostridium difficile and Clostridium perfringens research
1. Introduction
Norovirus (NoV), a highly contagious virus, is responsible for norovirus enteritis (NoVE) worldwide, particularly in the children under 2 years of age [1]. Typical clinical features of NoVE include diarrhea, vomiting, and abdominal pain. In some cases, the disease may progress to more severe manifestations, posing a significant public health challenge [2]. The NoV genome contains three open reading frames (ORFs) encoding a nonstructural polyprotein, the major capsid gene (VP1), and the minor capsid gene (VP2), with VP1 exhibiting high genetic variability [3]. It is classified into at least 10 genogroups, among which GI and GII are primarily responsible for human infections [4]. Specifically, GII genotype, particularly GII.4, accounts for the majority of outbreaks and sporadic cases worldwide [5].
While NoVE is generally self‐limiting, some children develop convulsions [6]. These convulsive episodes may lead to central nervous system (CNS) injury or even epilepsy in children, resulting in long‐term neurological sequelae. Despite this clinical significance, the pathogenesis of NoVE complicated by convulsions remains poorly understood [7]. Previous research studies have largely focused on describing clinical characteristics, whereas studies examining molecular epidemiology and genotype‐specific associations with convulsions are limited [8–11]. Furthermore, there are currently no approved drugs or vaccines targeting NoV infection complicated by convulsions [12].
These gaps highlight the need for a systematic investigation of both the clinical and molecular features of NoVE associated with convulsions. Specifically, the mechanisms remain unclear, including which clinical factors increase the risk of convulsions, how different NoV genotypes contribute to disease severity, and what evolutionary characteristics underlie their pathogenicity. Therefore, this study was designed to identify clinical risk factors associated with convulsions in children with NoVE and to characterize the genetic diversity of NoV strains as well as their associations with clinical manifestations through phylogenetic analysis.
2. Materials and Methods
2.1. Part I
2.1.1. Subjects
We retrospectively included children diagnosed with NoVE who were admitted to Kunming Children’s Hospital between November 2021 and May 2022. NoV infection was detected using real‐time PCR, consistent with the diagnostic approach recommended by the U.S. CDC for outbreaks and surveillance [13]. The inclusion criteria were as follows: (a) children younger than 5 years with a disease duration of less than 2 weeks; (b) laboratory‐confirmed NoV infection based on stool samples detected by real‐time PCR; (c) absence of coinfection with other opportunistic pathogens as determined by bacterial culture; and (d) met the Chinese clinical practice guideline for acute infectious diarrhea in children [14]. Exclusion criteria were as follows: (a) aged ≥ 5 years or illness duration ≥ 2 weeks; (b) evidence of infectious diarrhea caused by other pathogens, including bacteria (Salmonella, Shigella, Staphylococcus aureus, and Escherichia coli), fungi, parasites (roundworms, hookworms, pinworms), or other enteroviruses; and (c) history of epilepsy or presence of organic neurological lesions, autoimmune diseases, hematological disorders, inflammatory bowel disease, and food protein allergy.
2.1.2. Study Setting and Grouping
This was a retrospective case–control study in which patients were categorized into two groups: NoVE with convulsions group and NoVE without convulsions group (designated as NoVE group). Pediatric patients with confirmed NoVE but without convulsions were included in the NoVE group. For each participant, the following data were collected: (i) demographic characteristics: gender, race, and age; (ii) perinatal factors: birth weight, preterm status, mode of delivery (vaginal delivery or cesarean section), history of neonatal resuscitation, allergy, and rotavirus (RV) vaccination; (iii) clinical features: convulsive history, frequency of diarrhea and vomiting, fever, and dehydration; and (iv) laboratory parameters: routine hematology, serum biochemistry, inflammatory indices, and immune indices.
2.1.3. Screening for Risk Factors Associated With Convulsions
Comparisons between the two groups were first performed for demographic, perinatal, clinical, and laboratory variables. For biochemical analyses, 2 mL of fasting venous blood was collected, and serum was separated by centrifugation at 3500 r/min for 10 min. Levels of aspartate aminotransferase (AST), alanine aminotransferase (ALT), blood urine nitrogen (BUN), creatinine (Cr), creatine kinase (CK), CK‐MB, lactate dehydrogenase (LDH), alpha‐hydroxybutyrate dehydrogenase (α‐HBDH), and electrolytes were measured using an Olympus AU2700 analyzer. Routine hematology tests were performed on 2 mL of blood collected in EDTA‐2K tubes using a Sysmex XE5000 system. Variables with p < 0.05 in univariate logistic regression were entered into a multivariate logistic regression model to identify independent risk factors for convulsions. Model performance was assessed using receiver operating characteristic (ROC) curve analysis.
2.2. Part II
2.2.1. Reverse Transcription PCR
To determine the VP1 genotype of NoV, stool samples were collected from both the NoVE with convulsions and NoVE without convulsions groups. Solid stool (5–10 g) or watery stool (5–10 mL) was obtained from each subject. Virus RNA was extracted using the commercial E.Z.N.A Viral RNA kit (Cat. No. R6874‐02, Omega Bio‐tek), following the manufacturer’s instructions. Reverse transcription was performed with the PrimeScript RT Reagent Kit. PCR amplification targeted the VP1 region using specific primers for GI and GII genogroups: GI-SKF, 5′‐CTGCCCGAATTYGTAAATGA‐3′; GI-SKR, 5′‐CCAACCCARCCATTRTACA‐3′; GII-SKF, 5′‐CARGARBCNATGTTYAGRTGGATGAG‐3′; and GII-SKR, 5′‐CCRCCNGCATRHCCRTTRTACAT‐3′. Amplification conditions were as follows: 98°C for 2 min, followed by 35 cycles of 98°C for 10 s, 55°C for 15 s, and 72°C for 15 s.
2.2.2. Sanger Sequencing and Phylogenetic Analysis
Amplified PCR products were purified and sequenced by Tsingke Biotech (Kunming, China). Genogroup and genotype assignments were performed using the Norovirus Genotyping Tool Version 2.0 (https://www.rivm.nl/mpf/norovirus/typingtool). Sequences were further compared with the reference strains using BLAST (https://www.ncbi.nlm.nih.gov/blast). Representative NoV sequences of different genotypes were retrieved from GenBank. Multiple sequence alignments were generated with ClustalW software. Phylogenetic trees were constructed in MEGA X using the neighbor‐joining method with 1000 bootstrap replicates, as previously described [15]. Detection rates and VP1 positivity were calculated for both groups.
2.3. Statistical Analysis
Categorical variables were expressed as counts and percentages, while normally distributed continuous variables were presented as mean ± standard deviation (SD) and compared using Student’s t‐test. Skewed data were expressed as median (interquartile range) and analyzed using the Mann–Whitney U test. Group comparisons for categorical variables were performed using the chi‐square test. Logistic regression was used to identify risk factors associated with convulsions in NoVE patients, with variables selected using the forced‐entry method. All analyses were conducted with SPSS Version 26.0 (IBM Corp., Armonk, NY, USA). A two‐sided p value < 0.05 was considered statistically significant.
3. Results
3.1. Comparison of Demographic, Birth‐Related, Clinical, and Laboratory Characteristics
In total, 50 children were included in the NoVE with convulsion group, and 45 in the NoVE without convulsion group. All cases met the diagnostic criteria for acute infectious diarrhea, presenting with altered stool characteristics and/or increased stool frequency. There were no significant differences between groups in demographic characteristics (gender, race, allergy history, or RV vaccination) or birth‐related factors (preterm birth, delivery mode, or neonatal resuscitation) (all p > 0.05, Table 1). In terms of clinical features, fever and diarrhea frequency were significantly higher in the NoVE with convulsions group compared with the NoVE without convulsions group (all p < 0.001). No significant differences were observed in dehydration or vomiting frequency (p = 0.375). For the laboratory features, significant differences were detected between groups in BUN, CK, LDH‐MB, CK‐MB, Na^+^, Mg^2+^, and CD3 between the two groups (all p < 0.05).
3.2. Independent Risk Factors for NoVE With Convulsions
Logistic regression analysis identified that elevated serum CK‐MB and fever were independent risk factors for NoVE complicated by convulsions, while lower diarrhea frequency was a protective factor for convulsions in NoVE (Table 2). The simplified logistic regression formula was Logit(P) = 0.497 × CK‐MB‐1.71 × fever‐0.123 × diarrhea frequency. ROC analysis demonstrated good predictive performance of the model for NoVE with convulsions (AUC = 0.787, 95% CI = 0.694, 0.880; p < 0.001; Figure 1).
ROC curve for predicting model of the NoVE complicated with convulsions. The generated AUC was 0.787.
3.3. VP1 Genotypes in Both Groups
A total of 157 stool samples were collected from the NoVE and NoVE with convulsion groups. Of these, 114 samples (72.61%) tested positive for NoV, including 81 from the NoVE group and 33 samples from NoVE with convulsion group. Two VP1 genotypes were identified: GII.3 (17 samples) and GII.4 (97 samples). The GII.3 genotype was detected exclusively in 12 NoVE samples (14.81%) and 5 (15.19%) NoVE with convulsion group samples. The GII.4 genotype was present in 28 (84.85%) samples of the NoVE with convulsion group and 69 (85.19%) samples from NoVE group (Table 3).
3.4. Phylogenetic Analysis
After removing duplicate sequences, 80 unique sequences were obtained and submitted to GenBank database (Accession No. PP779629‐PP779708). Phylogenetic analysis revealed that 11 sequences belonged to genotype GII.3 and 69 sequences to GII.4 (Figure 2). The patient sequences complicated by convulsions were 5 GII.3 and 28 GII.4. Among the 80 sequences, 69 (86.25%) clustered with GII.4 strains, while 11 sequences (13.75%) clustered with GII.3 strains (Figure 2).
Phylogenetic tree analysis of VP1. The evolutionary tree was constructed using the neighbor‐joining method with 1000 bootstrap replicates in MEGA X. Evolutionary tree analysis showed that 11 of the 80 sequences had a genotype of GII.3, and 69 sequences were of GII.4. Bootstrap values ≥ 50% are shown; values < 70% indicate moderate support.
4. Discussion
NoV is recognized as a leading cause of acute gastroenteritis in children worldwide, responsible for considerable morbidity due to dehydration, electrolyte imbalance, and acid–base disturbances [16–18]. Beyond gastrointestinal manifestations, an increasing number of studies have reported neurological complications, most notably convulsions, in pediatric patients with NoV infection [19, 20]. Indeed, convulsion is caused by the transient synchronized discharge of a large number of neurons in the brain, resulting in uncontrollable twitching or changes in muscle tone of the voluntary muscles involved and even epilepsy [21, 22]. Frequent and prolonged convulsive attacks can cause nervous system injury in children, thereby affecting the growth and development. At present, the pathogenesis of NoVE complicated by convulsions is unclear as the reasons are complex. Some scholars believe that complicated convulsions are related to infection, high fever, young age, and genetic factors [6]. In this retrospective case–control study, we identified key clinical and laboratory predictors, including elevated CK‐MB levels, fever, and frequency of diarrhea, as independent influencing factors for NoVE complicated with convulsions. Furthermore, genotyping revealed that the majority of strains associated with convulsions belonged to the GII.4 genotype in the NoVE with convulsion group, underscoring its potential role in the pathogenesis of NoV‐related neurological complications.
Previous studies have primarily focused on identifying risk factors for convulsions in children with mild NoVE, such as RV infection, first seizure episode, and a history of convulsions [6, 23, 24]. However, limited research has addressed the specific risk factors associated with NoVE complicated by convulsions. In this study, NoV infection complicated with convulsions was used as the dependent variable, while age, BUN, CK, CK‐MB, LDH‐MB, Na^+^, Mg^2+^, CD3, fever, and diarrhea frequency were included as independent variables in the regression model. Multivariate logistic regression analysis revealed that elevated serum CK‐MB levels and fever were independent predictors of convulsions in NoVE, and lower frequency of diarrhea was a protective factor for convulsions in NoVE. Among these, CK‐MB is a well‐recognized marker of myocardial ischemia and injury [25]. Our findings demonstrated that children with NoVE complicated by convulsions had significantly higher CK‐MB concentrations compared with those without convulsions, suggesting that myocardial involvement may contribute to convulsive episodes. Additionally, the serum sodium Na + concentration in the NoVE with convulsion group was significantly lower than that in the NoVE group. Previous studies have indicated that hyponatremia reduces extracellular osmotic pressure, leading to fluid shifts in brain cells, cerebral edema, and subsequent convulsions. Furthermore, convulsions cause hypoxia and sodium pump dysfunction, which promote intracellular sodium influx and further decrease serum sodium concentrations [26, 27]. In our study, multivariate logistic regression identified that fever was an independent risk factor of convulsions after adjusting for CK‐MB level and diarrhea frequency. This suggests that while fever is common among all NoVE patients, within the broader context of other biological markers, the fever may distinguish those who are at higher risk for convulsions.
NoV infection combined with convulsions is associated with genomic variation. Previous studies have indicated that GII.4 genotype infection was an independent factor associated with convulsions [11, 28]. Globally, GII is the predominant genotype of NoV, particularly the GII.4 genogroup that has caused the majority of outbreaks and sporadic cases [29, 30]. In this study, 2 genotypes (GII.3 and GII.4) were isolated from the 114 stool samples. In the NoVE with convulsion group, GII.4 genotype was the major genotype. This may indicate that GII.4 genotype may associate with the onset of NoVE complicated with convulsion. Previous studies have occasionally detected NoV RNA in the bloodstream (viremia) and, rarely, in cerebrospinal fluid, suggesting the theoretical possibility of CNS involvement [31, 32]. Indeed, GII.4 was the predominant strain with a vast population susceptibility compared with GII.3 genotype. Besides a high similarity with some sequences in China in 2020–2022, the GII.4 sequences were also similar to the 2015 American strain (MK753030), the 2012, 2013, and 2017 Japanese strains (AB901267, OR844370, and LC390335), the 2014 South Korean strain (MN461018), and the 2015 UK strain (MH218629 and MH218674), presenting a high degree of similarity [33–35]. GII.3 sequences were closely related to strains from China (FK306213), USA (KY442319 and MK073886), and South Korea (GU980585) [36–38]. Recent molecular epidemiological studies from South Asia further support our findings. In a birth cohort in Dhaka, Bangladesh (2010–2013), a wide range of GI and GII VP1 genotypes were detected, with GII.4 constituting approximately 20% and GII.3 being among the frequent strains in pediatric gastroenteritis cases [39]. In Pakistan, a hospital‐based study reported a 16.1% prevalence of NoV among children under 5 years of age, with GII genogroup accounting for 73% of infections; both GII.3 and GII.4 were detected, though GII.4 proportions varied by setting [40]. Moreover, a systematic review across Asia highlighted the sustained dominance of GII.4 in India, Bangladesh, Taiwan, and Vietnam, while GII.3 remained more common in Malaysia, Russia, and Bangladesh [41]. These data align with our results, reinforcing the global epidemiological prominence of GII.4 strains and underscoring its potential role in NoVE‐associated convulsions.
Our study has certain limitations. The number of samples is small and it cannot cover all NoV genotypes. Besides, we still cannot identify the potential mechanisms of NoVE complicated with convulsions. We cannot perform the severity stratification (e.g., SCENARIO scores). In the future, more studies along with validation based on severity scores are required to validate our results.
5. Conclusions
Our findings indicate that elevated serum CK‐MB levels, fever, and frequency of diarrhea are independent influencing factors for NoVE complicated by convulsions. Moreover, genotyping revealed that the majority of strains associated with convulsions belonged to the GII.4 genotype, underscoring its potential role in the pathogenesis of NoV‐related neurological complications.
Ethics Statement
The study protocols were in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Kunming Children’s Hospital (approval no. 2022‐03‐009‐K01).
Consent
Written informed consent was obtained from the guardians of each child.
Conflicts of Interest
The authors declare no conflicts of interest.
Author Contributions
Suqi Xu: writing–original draft, validation, resources, methodology, and investigation. Mingying Wang: writing–original draft, data curation, visualization, and formal analysis. Canchun Zhao: methodology, data curation, and investigation. Jiahui Fang: methodology, investigation, and validation. Shumei He: software and investigation. Zhuoheng Li: methodology and visualization. Haoyu Ma: resources and data curation. Qiangming Sun: writing–review and editing, supervision, project administration, and conceptualization. Hongchao Jiang: writing–review and editing, supervision, project administration, and conceptualization. Suqi Xu and Mingying Wang contributed equally to this work.
Funding
This work was supported by the Xingdian Talent Support Program for Medical and Health Talents Project (XDYC‐YLWS‐2023‐0004; grant to Hongchao Jiang), Kunming Research Center for Pathogen Identification and Pathogenic Mechanism for Emerging and Unknown Infectious Diseases in Children (2023‐SW‐Research‐02; grant to Hongchao Jiang), Kunming Science and Technology Plan Project (2024‐1‐NS‐17; grant to Suqi Xu), and Health Research Project of Kunming Health Commission (2022‐06‐01‐015; grant to Suqi Xu).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Robilotti E. , Deresinski S. , and Pinsky B. A. , Norovirus, Clinical Microbiology Reviews. (2015) 28, no. 1, 134–164, 10.1128/cmr.00075-14, 2-s 2.0-84920938944.25567225 PMC 4284304 · doi ↗ · pubmed ↗
- 2Shah M. P. and Hall A. J. , Norovirus Illnesses in Children and Adolescents, Infectious Disease Clinics of North America. (2018) 32, no. 1, 103–118, 10.1016/j.idc.2017.11.004, 2-s 2.0-85041372766.29406972 PMC 6814392 · doi ↗ · pubmed ↗
- 3Hasing M. E. , Lee B. E. , Qiu Y. et al., Changes in Norovirus Genotype Diversity in Gastroenteritis Outbreaks in Alberta, Canada: 2012–2018, BMC Infectious Diseases. (2019) 19, no. 1, 10.1186/s 12879-019-3792-y, 2-s 2.0-85061855288.PMC 638181230782126 · doi ↗ · pubmed ↗
- 4Diao X. , Guo C. , and Li S. , Identification of a Novel Anoikis-Related Gene Signature to Predict Prognosis and Tumor Microenvironment in Lung Adenocarcinoma, Thoracic Cancer. (2023) 14, no. 3, 320–330, 10.1111/1759-7714.14766.36507553 PMC 9870742 · doi ↗ · pubmed ↗
- 5Haddadin Z. , Batarseh E. , Hamdan L. et al., Characteristics of GII.4 Norovirus Versus Other Genotypes in Sporadic Pediatric Infections in Davidson County, Tennessee, USA, Clinical Infectious Diseases. (2021) 73, no. 7, e 1525–e 1531, 10.1093/cid/ciaa 1001.32667045 PMC 8492161 · doi ↗ · pubmed ↗
- 6Kim G. H. , Byeon J. H. , Lee D. Y. , Jeong H. J. , and Eun B. L. , Norovirus in Benign Convulsions With Mild Gastroenteritis, Italian Journal of Pediatrics. (2016) 42, no. 1, 10.1186/s 13052-016-0303-2, 2-s 2.0-85009085841.PMC 509632527809881 · doi ↗ · pubmed ↗
- 7Hu M. H. , Lin K. L. , Wu C. T. , Chen S. Y. , and Huang G. S. , Clinical Characteristics and Risk Factors for Seizures Associated With Norovirus Gastroenteritis in Childhood, Journal of Child Neurology. (2017) 32, no. 9, 810–814, 10.1177/0883073817707302, 2-s 2.0-85025065776.28482763 · doi ↗ · pubmed ↗
- 8Fang Y. , Dong Z. , Liu Y. et al., Molecular Epidemiology and Genetic Diversity of Norovirus Among Hospitalized Children With Acute Gastroenteritis in Tianjin, China, 2018–2020, BMC Infectious Diseases. (2021) 21, no. 1, 10.1186/s 12879-021-06375-2.PMC 827798634261441 · doi ↗ · pubmed ↗