Antimicrobial effect of plantago major extract against streptococcus mutans in dental caries formation
Heide Mendonça Moreira De Souza, Ivana Suffredini Barbosa, Karen Cristina Comin Maldonado, Cristina Lúcia Feijó Ortolani

TL;DR
This study shows that Plantago major extract can inhibit Streptococcus mutans, a bacteria linked to tooth decay, suggesting it could be a natural alternative to traditional treatments.
Contribution
The study demonstrates the antimicrobial potential of Plantago major extract against Streptococcus mutans for dental caries control.
Findings
Plantago major extract produced inhibition zones with a mean diameter of 9.95 mm against Streptococcus mutans.
The extract's antimicrobial effect was statistically significant (p < 0.05) compared to chlorhexidine.
The findings suggest Plantago major could be a natural therapeutic agent with fewer side effects for caries control.
Abstract
This study evaluated the efficacy of Plantago major extract against Streptococcus mutans, a bacterium associated with biofilm formation and the development of dental caries, in search of natural alternatives to conventional methods of caries control. An experimental design was conducted using bioautography and broth microdilution techniques to assess the antimicrobial activity of the extract, with chlorhexidine serving as the comparative substance. The results demonstrated that Plantago major consistently produced inhibition zones with a mean diameter of 9.95 ± 0.41 mm, although smaller than those observed for chlorhexidine (CHX 1%) and CHX 0.12%, which averaged 14.98 ± 0.22 mm. Statistical analysis confirmed the significance of the antimicrobial effect of the extract (p < 0.05), suggesting its potential as a natural therapeutic agent. In conclusion, Plantago major extract showed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1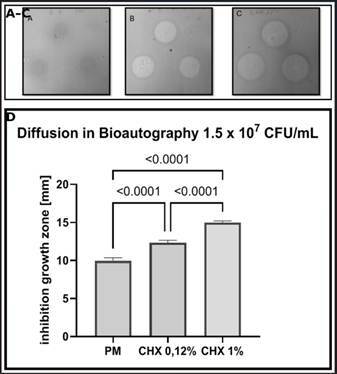 Figure 2
Figure 2- —CAPES
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPhytochemistry and Biological Activities · Medicinal Plant Extracts Effects · Sesquiterpenes and Asteraceae Studies
Introduction
The oral microbiota consists of approximately 700 species of prokaryotes, distributed across 185 genera and 12 phyla, of which 54% have an official name, 14% are anonymous (cultivable), and 32% are known only as uncultivable phylotypes1. The development of dental caries is associated with a complex microbial community that adheres to the tooth surface, forming dental biofilm2. This biofilm is a multilayered system composed of bacteria, bacterial products, and saliva in a hydrated state, with distinct mechanical and rheological properties3. Species of the Streptococcus genus, especially Streptococcus mutans (S. mutans), play a crucial role in biofilm formation and the production of extracellular polysaccharides from sucrose4. Studies indicate that S. mutans also promotes the adhesion of other harmful bacteria5 ^,^ 6.
The control of dental caries represents a significant challenge for global public health, impacting quality of life and productivity. According to the World Health Organization7, dental caries affects approximately 60 to 90% of school-aged children and nearly 100% of adults worldwide8 ^,^ 9 ^,^ 10. This condition impacts chewing, growth, and development, in addition to affecting emotional well-being. Moreover, it can lead to permanent tooth loss11 ^,^ 12.
The initial phase of dental caries is characterized by white spot lesions. In recent years, an increase in prevalence has been noted, with rates ranging from 10% to 49%. These lesions are frequently found in patients undergoing orthodontic treatment and are caused by plaque accumulation in the cervical region of the teeth13. The use of fluoride in various forms remains the cornerstone of dental caries prevention. Fluoride primarily acts by inhibiting enamel demineralization and enhancing remineralization; it promotes the formation of acid-resistant fluorapatite that reinforces the enamel’s resistance to acid attack14. However, current methods, such as the addition of fluoride to the water supply, are considered insufficient. Therefore, additional approaches are necessary to improve treatment efficacy15
Dental biofilm can be mechanically controlled through practices such as brushing and flossing. Additionally, chemical approaches, mainly using substances like chlorhexidine, have been extensively studied due to their effective antimicrobial action16. For example, chlorhexidine (CHX) is a cationic bisbiguanide antiseptic that binds to negatively charged bacterial cell membranes, causing membrane disruption and leakage of cytoplasmic components4. At higher concentrations or with prolonged exposure, CHX causes cytoplasmic coagulation and precipitation of intracellular compounds, resulting in irreversible bacterial cell death5. Its positive charge also enables it to adsorb to oral surfaces, interfering with bacterial adhesion and inhibiting biofilm formation6. Although chlorhexidine is considered the gold standard for bacterial control, prolonged use can produce adverse effects, including taste alterations (dysgeusia), tooth staining, and, in rare cases, allergic reactions17 ^,^ 18 ^,^ 19. Furthermore, bacterial resistance to chlorhexidine is a growing concern, highlighting the need to explore safe and effective alternatives20.
In this context, herbal medicines have emerged as promising alternatives for controlling dental biofilm and preventing dental caries. They offer advantages such as lower toxicity, reduced cost, and easy accessibility21 ^,^ 22 ^,^ 23. However, the safety and efficacy of phytotherapeutic agents depend on factors such as dosage, preparation method, and individual patient response; some herbal constituents may be toxic at high concentrations or if improperly formulated8. Among the medicinal plants studied, Plantago major L. (Plantaginaceae), commonly known as Broadleaf Plantain, has drawn attention for its antibacterial, anti-inflammatory, and antioxidant properties24. Plantago major (P. major) is a plant known for its abundance of bioactive compounds, including flavonoids, terpenoids, iridoid glycosides, and fatty acids25. These compounds confer anti-inflammatory, wound-healing, and antioxidant properties to the plant, along with significant antibacterial activity. Studies have indicated that aucubigenin, derived from iridoid glycosides and present in Broadleaf Plantain, exhibits antibacterial activity, especially against gram-positive microorganisms such as Streptococcus mutans 26. In addition to these general effects, P. major contains flavonoids and phenolic compounds that can directly interfere with bacterial physiology. Flavonoids in P. major have been reported to intercalate into bacterial DNA and RNA, inhibiting nucleic acid synthesis and altering membrane fluidity. Tannins from the extract can bind to bacterial adhesins and enzymes, impairing S. mutans adhesion and metabolic activity. These multi-target actions likely contribute to the observed inhibition of S. mutans growth and cariogenic biofilm formation by the extract. 27
The present study aimed to evaluate the efficacy of P. major as an antibacterial agent against Streptococcus mutans, one of the primary pathogens involved in dental caries. The hypothesis of this study is that the extract of Plantago major L. possesses antimicrobial activity against Streptococcus mutans, potentially serving as an effective alternative in the prevention of dental caries, with potential applications in contemporary dentistry.
Materials and Methods
An in vitro study was conducted to evaluate the antimicrobial activity of aqueous and ethanolic extracts of Plantago major L. against Streptococcus mutans. The minimum inhibitory concentration (MIC) and the minimum bactericidal concentration (MBC) were determined using the broth microdilution test, according to the guidelines of the Clinical and Laboratory Standards Institute (CLSI, 2008)28, with adaptations.
Antimicrobial activity was also investigated through the bioautography test associated with thin-layer chromatography, allowing the identification of inhibition zones and the evaluation of the extracts' efficacy. Both methods provided complementary data for characterizing the antimicrobial action of the tested extracts.
Study Site
The present study was conducted at the Biodiversity Research Center (NPBio) of Universidade Paulista (UNIP), São Paulo, Brazil.
Plant Material and Controls
The Plantago major L. (Plantaginaceae) extract, obtained from aerial parts, was purchased from Heide Extratos Vegetais, Pinhais, Paraná, Brazil (batch 2168, manufactured on 04/27/2023, valid until 05/2025, quality control nº 84929-431). In addition, 1% and 0.12% chlorhexidine gluconate solutions provided by Fórmula & Ação, São Paulo-SP, Brazil (manufactured on 10/15/2023, valid until 10/2025) were used as positive controls.1.2 Preparation of Bacterial Inoculum
The Streptococcus mutans strain (ATCC 25175) was previously thawed and cultured on Brain Heart Infusion (BHI) agar (Oxoid®). A bacterial suspension was prepared in 0.9% saline solution, and the concentration was adjusted to 1.5 × 10⁸ CFU/mL for the pilot test and experiment 0129, 1.5 × 10⁷ CFU/mL for experiment 02, and 1.5 × 10⁶ CFU/mL for experiment 03. The concentrations were determined by viable colony counts through serial dilutions or by turbidity adjusted to the MacFarland scale.
Subcultures were generated from two master plates, each containing 100 μL of thawed bacterial culture. These subcultures were transferred to Petri dishes containing Oxoid® CM1136 BHI agar and incubated at 36°C for 48 hours30. A bacterial suspension was prepared from these subcultures by performing serial dilutions in seven tubes with 9 mL of saline solution each. After incubation, colonies were counted, and the average count was used to adjust the bacterial suspension concentration according to the MacFarland scale (0.5 MacFarland).
Evaluation of Plantago major Extract
The antimicrobial activity was evaluated by the agar disk diffusion method. S. mutans colonies were suspended in sterile saline solution and inoculated onto Petri dishes containing Oxoid® CM1136 BHI agar using disks impregnated with the extract and controls. Inhibition zones were measured after 48 hours of incubation at 36°C. When inhibitory zones were identified, their dimensions were measured precisely using a caliper and expressed in millimeters, as documented in previous studies31. Two measurements were taken for each inhibition zone-one vertically and one horizontally-to ensure precision.
Determination of minimum inhibitory concentration and minimum bactericidal concentration
Bacterial suspensions were incubated in BHI broth with different concentrations of the tested agents for 48 hours at 36°C. Turbidity was evaluated, and subcultures were performed.
A bacterial suspension in BHI broth was prepared from young S. mutans colonies at a concentration of 1.5 × 10⁷ CFU/mL, as described in section 1.3. In a 96-well U-bottom microplate, 190 µL of bacterial suspension was added to each well. 40 µL of plant extract or 1% chlorhexidine at different concentrations were added in triplicate32. The P. major extract was tested at concentrations ranging from 40 mg/mL to 0.3125 mg/mL, based on preliminary studies indicating this range as potentially effective against S. mutans. Chlorhexidine was tested at concentrations ranging from 1% to 0.12%, according to standard concentrations used in the literature.
Six wells were reserved for the negative control (culture medium only) and six wells for the positive control (culture medium with S. mutans inoculum)33. The microplates were incubated at 36°C for 48 hours. Turbidity was evaluated, and subcultures were performed from each well using 2 µL of supernatant, which were inoculated onto sterile BHI agar plates30.
Bioautography
Diffusion in Bioautography (DiB)
The ability of the Plantago major extract to inhibit bacterial growth was evaluated by bioautography, combining thin-layer chromatography with the disk diffusion test. The experiment was performed in triplicate for the extract samples and positive control (1% chlorhexidine).
Silica gel GF254 aluminum-backed plates (5 x 5 cm) were used. 10 µL of the plant extract or positive controls was applied per sample. Chromatograms were placed in 90 mm Petri dishes containing 5 mL of BHI agar previously inoculated with S. mutans (1.5 x 10⁸ CFU/mL for experiment 01 and 1.5 x 10⁷ CFU/mL for experiment 02). After gelification, 10 mL of BHI agar inoculated with the same bacterial concentrations was added.
Plates were incubated at 36°C for 48 hours. After this period, inhibition zones were identified using MTT viability dye (tetrazolium salt, 0.5 mg/mL). The inhibition zones were measured with a caliper in both horizontal and vertical directions.
Statistical Analysis
Statistical analyses were performed using GraphPad Prism version 10.1.2.324. Data are presented as mean ± standard deviation (SD) and 95% confidence intervals (CI). Normality was assessed by Shapiro-Wilk and Kolmogorov-Smirnov tests (Shapiro-Wilk W = 0.9332, 0.9516 and 0.8788 for P. major, CHX 0.12% and CHX 1%, respectively; corresponding p = 0.415, 0.6602 and 0.2638; Kolmogorov-Smirnov KS = 0.1478, 0.1458 and 0.2361, p > 0.10 for all groups), indicating that the samples did not deviate from normality at α = 0.05. Homogeneity of variances was evaluated with Brown-Forsythe and Bartlett tests and showed no significant differences between groups. Outlier detection using the ROUT method (Q = 5%) identified no outliers. For comparisons among the three treatment groups (P. major, CHX 0.12% and CHX 1%), one-way ANOVA was used followed by Tukey’s multiple comparisons. Sample sizes for the DiB experiments were n = 12 (P. major), n = 12 (CHX 0.12%), and n = 6 (CHX 1%); these arise from two independent experiments with three disks per treatment and two orthogonal measurements per disk (totaling six measurements per treatment per experiment).
Results
Determination of Minimum Inhibitory Concentration and Minimum Bactericidal Concentration**.** The determination of the minimum inhibitory concentration (MIC) was performed using the broth microdilution method, as described in the methodology. The MIC is the lowest concentration of the antimicrobial agent capable of interrupting the growth of the microorganism, reflecting its bacteriostatic capacity34. For the S. mutans strain, with an initial concentration of 1.5 × 10^7^ CFU/mL, the MIC of the extract was determined to be 25 mg/mL. This result indicates that, even at the highest dilutions tested, the extract maintained its inhibitory effect against the bacterium.
The 96-well plate microdilution tests confirmed the efficacy of the Plantago major extract in inhibiting the growth of S. mutans, with the MIC set at 25 mg/mL. Despite the 20-fold dilution in the microdilution technique, the extract demonstrated sustained antimicrobial activity, reinforcing the importance of the interaction between the chemical components of the extract for its efficacy. Although the MIC was established, the minimum bactericidal concentration (MBC) could not be determined with the tested concentrations, as even at the highest tested concentration of 40 mg/mL, no microorganism death was observed**.** In other words, under the conditions tested, Plantago major extract inhibited S. mutans growth (bacteriostatic effect) but did not kill the bacteria (no bactericidal effect). A bacteriostatic agent prevents bacterial proliferation (inhibiting growth) without causing irreversible cell death, whereas a bactericidal agent causes bacterial cells to die. After subculture, microbial growth was observed in all tested dilutions, confirming that the extract was bacteriostatic rather than bactericidal under the study conditions.
Analysis and Results of Antibacterial Activity by Bioautography
The bioautography diffusion technique was used to measure the inhibition zones formed by P. major and chlorhexidine (CHX) treatments against S. mutans. The results are presented in Figures 1A, 1B, and 1C and include detailed statistical analysis by one-way ANOVA and Tukey’s multiple comparisons test. The bar graph presents the mean inhibition zones for treatments with P. major, 0.12% chlorhexidine (CHX 0.12%), and 1% chlorhexidine (CHX 1%), with the standard error of the mean (SEM) represented by error bars. Significant differences between treatments are indicated by p-values above the bars (p < 0.0001). The descriptive values for the experimental groups were as follows: CHX 1%, mean = 14.98 ± 0.22 mm; CHX 0.12%, mean = 12.35 ± 0.31 mm; and P. major, mean = 9.95 ± 0.41 mm.
Figure 1. Antimicrobial activity of Plantago major extract and chlorhexidine measured by bioautography and diffusion assay.
One-way ANOVA revealed a significant difference among the groups (F2 ^,^ 27 = 449.8; p < 0.0001). Tukey’s post-hoc test confirmed statistically significant differences between all pairwise comparisons (p < 0.0001). The descriptive and comparative results are summarized in Table 1.
Table 1. Mean inhibition zones (mm) with descriptive statistics and Tukey's multiple comparisons for Plantago major (PM), 0.12% chlorhexidine (CHX 0.12%), and 1% chlorhexidine (CHX 1%).GroupnMean (mm)DP (mm)Standard Error (mm)CI 95% BottomCI 95% TopP. Major129.950.410.1186.68910.211CHX 0.12%1212.350.310.08912.15312.547CHX 1%614.980.220.0914.74915.211
The Tukey-adjusted pairwise comparisons between the treatment groups (Plantago major, CHX 0.12%, and CHX 1%), including mean differences, 95% confidence intervals, and adjusted p-values, are shown in Table 2.
Table 2. Statistical comparison of inhibition zones among treatment groups.GroupMean difference (mm)CI 95%p ValueP. Major vs CHX 0.12%-2.4-2.744 0 to -2.053<0.0001P. Major vs CHX 1%-5.03-5.452 to -4.605<0.0001CHX 0.12% vs CHX 1%-2.63-3.053 to -2.207<0.0001
Statistical results for dib analysis
The statistical analysis of the study was expressed by means, 95% confidence intervals, and p-values adjusted by Tukey's test for the samples of P. major, chlorhexidine (CHX 0.12%), and chlorhexidine (CHX 1%). The bioautography diffusion analysis at a concentration of 1.5 x 10⁷ CFU/mL. Statistical tests were conducted to evaluate the normal distribution of the data. The Shapiro-Wilk test produced W values of 0.9332, 0.9516, and 0.8788 for P. major, CHX 0.12%, and CHX 1%, respectively, with associated p-values of 0.415, 0.6602, and 0.2638, indicating that the data passed the normality test at the 0.05 significance level. Similarly, the Kolmogorov-Smirnov test showed KS distances of 0.1478, 0.1458, and 0.2361, with p-values above 0.1000 for all samples, confirming the normality of the data. Outlier analysis by the ROUT method (Q = 5%) did not identify any outlier values among the P. major, CHX 0.12%, and CHX 1% samples.
The statistical results of the bioautography diffusion analysis (DiB) revealed significant insights into the antibacterial activity of Plantago major extract compared to 0.12% and 1% chlorhexidine (CHX). Means, 95% confidence intervals, and p-values adjusted by Tukey's test were used for analysis. Although studies in the literature have investigated a variety of natural extracts for antimicrobial activity, the superiority of chlorhexidine is often observed, reinforcing the continued need for natural antimicrobial agents to mitigate side effects associated with conventional antimicrobials 36 ^,^ 37. The results of the present study highlight the importance of Plantago major as a potential source of antibacterial compounds, with its inhibition halos averaging 9.95 mm.
Discussion
The present study evaluated the antimicrobial effect of Plantago major extract against Streptococcus mutans and its capacity to reduce dental biofilm formation. Our results indicate that P. major produced significant inhibition of S. mutans growth and attenuated biofilm formation in vitro, findings that corroborate previous reports of antimicrobial activity for P. major and related phytotherapeutics20 ^,^ 34.
Mechanistically, the observed activity of P. major can be attributed to its complex phytochemical composition, which includes iridoid glycosides, flavonoids, and phenolic compounds. These constituents likely act through multiple, complementary routes: disruption of bacterial membrane integrity and membrane fluidity, inhibition of nucleic acid synthesis, and binding to bacterial adhesins and enzymes involved in adherence and extracellular polysaccharide production. Such multi-target effects plausibly impair S. mutans physiology and the organism’s ability to produce the extracellular matrix required for robust biofilm maturation 20 ^,^ 23 ^,^ 25. These mechanistic considerations are consistent with other in vitro reports demonstrating P. major’s antimicrobial and antibiofilm properties 25 ^,^ 34.
In the present study, the extract produced a measurable MIC (25 mg/mL), but an MBC was not demonstrable at the highest concentration tested (40 mg/mL). This result indicates a bacteriostatic action under the tested conditions: the extract inhibits bacterial proliferation without causing irreversible cell death at the concentrations assessed. Clinically, bacteriostatic agents can reduce microbial load and virulence, yet their effectiveness depends on adjunctive measures (host immune response, mechanical plaque removal, and topical fluoride), because residual viable cells may regrow if favorable conditions persist 7 ^,^ 26. Therefore, a bacteriostatic phytotherapeutic such as P. major would more appropriately be considered as a complementary strategy rather than a standalone replacement for established preventive measures.
Quantitative comparison in our bioautography assays showed larger inhibition zones for chlorhexidine than for P. major, reflecting the recognized in vitro potency of chlorhexidine 16. Nevertheless, chlorhexidine use is associated with adverse effects and tolerability concerns when used long-term (e.g., taste alteration, staining), and there are increasing discussions about resistance or reduced susceptibility following prolonged exposure 17 ^,^ 18. These issues motivate the search for adjunctive agents that may offer acceptable antimicrobial activity with different safety or tolerability profiles. In this context, P. major may provide antimicrobial benefit with a lower side-effect burden, but direct clinical comparisons require comprehensive evaluation of efficacy, safety, and long-term outcomes.
It is essential to emphasize that dental caries is a multifactorial disease: microbial colonization is only one determinant. Host factors (salivary flow and composition), dietary habits (frequency and quantity of fermentable carbohydrate intake), fluoride exposure, and the effectiveness of mechanical plaque control are all fundamental elements in caries risk and progression 6 ^,^ 17. Accordingly, any prospective role for P. major in caries control must be considered within an integrated preventive approach that addresses diet, fluoride use, and oral hygiene.
This study has several limitations that constrain direct clinical extrapolation. First, the work was performed in vitro using a single reference strain of S. mutans and therefore does not capture the ecological complexity of multispecies oral biofilms or host-microbe interactions 3 ^,^ 23. Second, the number of experimental replicates per group was limited, and the extract batch was not fully chemically standardized, factors that may affect reproducibility across laboratories 25 ^,^ 34. Third, safety assessments such as cytotoxicity or mucosal tolerance tests were not performed, so topical biocompatibility remains unknown. Fourth, while diffusion and dilution assays are established screening tools, translating MIC/MBC values into clinically effective formulations and concentrations requires pharmacokinetic, formulation, and in vivo evaluation26. Finally, although statistical analyses were applied to the present dataset, larger sample sizes and more robust experimental designs (e.g., blinded outcome assessment, pre-registered protocols) would strengthen future investigations.
To advance the evidence base, future research should: 1 use chemically standardized P. major preparations with complete phytochemical profiling; 2 evaluate antimicrobial and antibiofilm effects in multispecies biofilm models and in situ or in vivo systems that better mimic clinical conditions; 3 perform cytotoxicity and mucosal tolerance testing to assess safety for topical use; 4 explore potential synergistic interactions with fluoride or mechanical plaque control; and 5 design randomized clinical trials to determine clinical effectiveness in caries prevention or as an adjunct in periodontal or mucosal therapies. Methodological improvements such as larger sample sizes, blinded assessments, and robust statistical planning will increase reliability and reproducibility.
In summary, Plantago major extract demonstrated bacteriostatic antimicrobial activity against S. mutans and reduced biofilm formation in vitro. Given its multi-constituent mode of action and the global need for alternative antimicrobial strategies, P. major warrants further preclinical standardization and clinical evaluation as a complementary agent in oral care regimens. Nonetheless, current evidence supports a cautious interpretation: P. major is a promising adjunct but not yet a substitute for established preventive measures such as fluoride application, mechanical plaque control, and, when clinically indicated, short courses of conventional antimicrobials.
Conclusion
The present study demonstrated the significant antimicrobial activity of Plantago major extract, evidenced by its efficacy in diffusion and microdilution tests against Streptococcus mutans, a critical dental pathogen. Although the inhibition zones were smaller than those produced by chlorhexidine, P. major extract proved to be a promising natural alternative, with the potential to combat biofilm formation and the progression of dental caries.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Deo PN Deshmukh R Oral microbiome: Unveiling the fundamentals J Oral Maxillofac Pathol 201923112212810.4103/jomfp.JOMFP_304_18PMC 650378931110428 · doi ↗ · pubmed ↗
- 2Marsh PD Zaura E Dental biofilm: ecologicalinteractions in health and disease J Clin Periodontol 20174418122210.1111/jcpe.1267928266111 · doi ↗ · pubmed ↗
- 3Sterzenbach T Helbig R Hannig C Hannig M Bioadhesion in the oral cavity and approaches for biofilm management by surface modifications Clin Oral Investig 202024124237426010.1007/s 00784-020-03646-1Epub 2020 Oct 2733111157 PMC 7666681 · doi ↗ · pubmed ↗
- 4Ben-Zaken H Isolation and Characterization of Streptococcus mutans Phage as a Possible Treatment Agent for Caries Viruses 20212582582510.3390/v 13050825 PMC 814748234063251 · doi ↗ · pubmed ↗
- 5Boyd JDAJ Stromberg CS Miller ME Grady Biofilm and cell adhesion strength on dental implant surfaces via the laser spallation technique Dent Mater 202137485910.1016/j.dental.2020.10.01333208265 PMC 7775913 · doi ↗ · pubmed ↗
- 6Barbosa JO Rossoni RD Vilela SF De Alvarenga JA Velloso MDOS Prata MC Streptococcus mutans can modulate biofilm formation and attenuate the virulence of Candida albicans P Lo S One 2016113 e 015045710.1371/journal.pone.0150457 PMC 477498026934196 · doi ↗ · pubmed ↗
- 7World Health Organization Global oral health status report: towards universal health coverage for oral health by 2030[Internet]Geneva World Health Organization 2022[citedyearmonth day]Available from:
- 8Azeredo FN Guimarães LS Luís W Fialho S Antunes LAA Antunes LS Estimated prevalence of dental caries in athletes: an epidemiological systematic review and meta-analysis J Indian Soc Pedod Prev Dent 202038229729710.4103/ijdr.IJDR_764_1832436912 · doi ↗ · pubmed ↗