Development of a Prognostic Nomogram in Epithelial Ovarian Cancer Based on KELIM: A Retrospective Study at TuDu Hospital, Vietnam
Hoang T. Pham, Tuan M. Vo, Le N. N. Phan, Hien T. Nguyen

TL;DR
This study develops a survival prediction tool for ovarian cancer patients in Vietnam using factors like KELIM and tumor stage.
Contribution
A novel prognostic nomogram for epithelial ovarian cancer patients in Vietnam based on KELIM and clinical variables.
Findings
KELIM < 1, elevated CA-125, advanced tumor stage, and residual tumor were significant survival predictors.
The nomogram integrates these variables to provide personalized prognostic assessments for EOC patients.
Cumulative mortality rates increased from 1.4% at 1 year to 16.5% at 5 years.
Abstract
Background/Objectives: Epithelial ovarian cancer (EOC) constitutes the predominant form of ovarian malignancies. The primary goal of this study was to determine predictors of patient survival and construct a nomogram for survival prediction in individuals diagnosed with epithelial ovarian cancer. Methods: A retrospective cohort analysis was performed, including 418 patients who received treatment for epithelial ovarian cancer at Tu Du Hospital from January 2015 to December 2019. The median follow-up time was 77.1 months (range: 5.7–121.6 months). Survival analyses were conducted using the log-rank test and Cox proportional hazard regression analysis. A nomogram was developed, incorporating KELIM and other statistically significant variables. Results: The median follow-up time was 77.1 months. The observed cumulative mortality rates were 1.4% (95% confidence interval [CI]: 0.7–3.2),…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
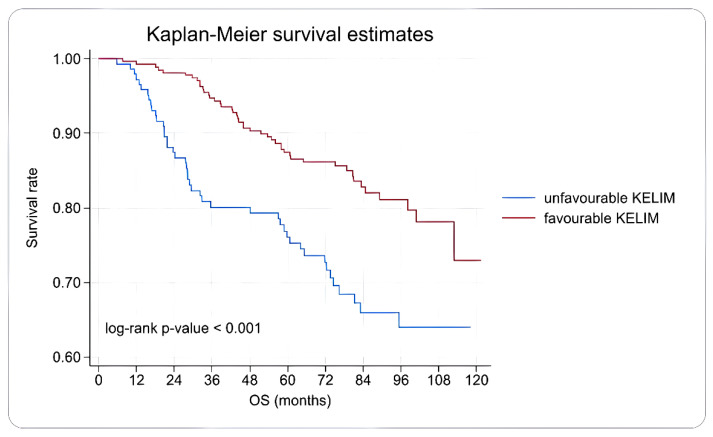 Figure 1
Figure 1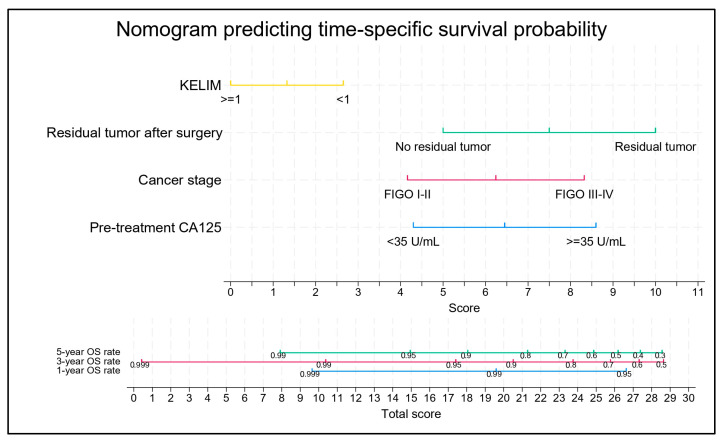 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOvarian cancer diagnosis and treatment · PARP inhibition in cancer therapy · Cancer Mechanisms and Therapy
1. Introduction
Epithelial ovarian cancer (EOC) is the predominant form of ovarian malignancy, accounting for 82% to 91% of all diagnoses [1]. The disease frequently manifests with a lack of early symptoms, resulting in approximately 70% of patients being diagnosed at an advanced stage (FIGO stage III-IV) [1], subsequently leading to a poor prognosis for survival. Global statistics from GLOBOCAN for 2022 documented 324,603 new occurrences and 206,956 fatalities stemming from ovarian cancer [2]. In Vietnam, in the same year, 1404 new diagnoses and 923 deaths were attributed to this disease [2].
Although therapeutic interventions have improved, the 5-year survival rate for EOC remains limited (35–57%), and the recurrence rate is elevated (>95%) [1,3]. Consequently, the identification of early and accurate prognostic indicators is critical for tailoring treatment strategies, thus enhancing both patient survival and overall quality of life.
Numerous established prognostic factors impact survival, including cancer stage, the amount of residual tumor following debulking surgery, and initial levels of cancer antigen (CA-125) [4,5]. More recently, the CA-125 Elimination rate constant K (KELIM), introduced by You et al. in 2013, has emerged as a dynamic marker that reflects the decrease in CA-125 levels during chemotherapy [6]. KELIM is a model-based kinetic parameter derived from the early longitudinal decline of serum CA-125 during first-line platinum-based chemotherapy and is considered an early surrogate of intrinsic tumor chemosensitivity. Practically, KELIM is estimated using at least three CA-125 measurements obtained during the first three chemotherapy cycles (within approximately the first 100 days after chemotherapy initiation), applying a validated population kinetic model implemented in an online calculator (Biomarker Kinetics™, was developed by a research team from Lyon University (Université Claude Bernard Lyon 1, France) and Lyon University Hospital (Hospices Civils de Lyon, France)). Higher KELIM values indicate faster CA-125 elimination and have been consistently associated with improved outcomes in epithelial ovarian cancer KELIM indicates an early response to chemotherapy and demonstrates a significant association with the survival duration of patients with EOC [6,7].
Tu Du Hospital, the foremost obstetrics and gynecology referral center in Southern Vietnam, manages approximately 250 ovarian cancer cases annually. Notably, the institution operates under a distinct referral framework, wherein patients initially diagnosed with advanced-stage epithelial ovarian cancer are routinely directed to tertiary oncology centers for comprehensive multimodal management. Consequently, the majority of ovarian cancer patients treated at Tu Du Hospital are diagnosed at an early stage and are typically suitable candidates for primary radical cytoreductive surgery. This institutional treatment model accounts for the predominance of early-stage disease in our study cohort. Despite the center’s high clinical volume, KELIM has not seen widespread application in early survival predictions at this facility. This research initiative aimed to assess the utility of KELIM and its associated elements in forecasting the survival outcomes of patients with EOC.
2. Materials and Methods
A retrospective cohort analysis was performed between June 2024 and March 2025, focusing on individuals diagnosed with epithelial ovarian cancer (EOC) treated at Tu Du Hospital, with initial surgical interventions occurring between January 2015 and December 2019. This study encompassed the entire available population within a specified timeframe. All cases confirmed with a histopathological diagnosis of EOC and subjected to a minimum of three cycles of carboplatin-paclitaxel chemotherapy constituted the inclusion criteria. Patients with concurrent malignancies or incomplete medical records were excluded from the study. The research protocol was approved by the Institutional Review Board of Tu Du Hospital (Approval Number: 610/QD-BVTD, 9 April 2024). Patient consent was waived due to the retrospective nature of the study.
The data collected included basic demographic information, pretreatment CA-125, cancer stage (FIGO 2021) [8], number of chemotherapy cycles, and surgical and pathological characteristics. KELIM was calculated using the website “Circulating tumor biomarker—Biomarker Kinetics™” (accessed on 4 December 2025) using CA-125 levels in the first three chemotherapy cycles. The KELIM was divided into two groups: favorable (KELIM ≥ 1) and unfavorable (KELIM < 1) [9,10]. Initial treatment response was defined according to the RECIST 1.1 criteria [11]. Three weeks after the end of the last chemotherapy cycle, patients were scheduled for follow-up visits to assess residual tumor tissue using imaging and CA-125 test results. Patients were defined as having responded to treatment when there was no residual tumor tissue after treatment and CA-125 was <35 U/mL; Patients did not respond to treatment when tumor tissue remained after treatment or CA-125 was ≥35 U/mL. Follow-up imaging was performed according to the treating physician’s clinical indication. In our institution, post-treatment assessment of residual disease was primarily conducted using pelvic/abdominal ultrasound, with pelvic MRI utilized when additional anatomic characterization was required or when ultrasound findings were equivocal. Imaging results were interpreted in conjunction with clinical evaluation and serum CA-125 levels to determine treatment response and the presence of residual tumor.
Time from surgery to start of chemotherapy (TTC) was defined as the interval (in days) from the date of surgery to the date of initiation of first adjuvant chemotherapy. The neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) were categorized using optimal thresholds identified via receiver operating characteristic (ROC) curve analysis, achieving 90% sensitivity in predicting 5-year mortality (NLR: 1.61; PLR: 114.43). Survival duration, measured in months, was calculated from the date of diagnosis to either all-cause mortality [12] the most recent documented survival date, or the study’s conclusion in March 2025.
Calculating sample size with survival research formula:
= 0.05; = 0.1. Pauline Corbaux’s 2023 systematic review study [7] found that the group with favorable KELIM had a longer progression-free survival than the unfavorable KELIM group with HR = 0.49. Substituting this into the formula, n = 98 was obtained as the minimum sample size to ensure sample power for the main objective.
Statistical Analysis: Data analysis was performed utilizing the Stata 17.0 software (Stata Corp LLC, Lakeway Drive College Station, College Station, TX, USA, April 2021). Descriptive statistics for the study cohort are presented using proportions or medians. The cumulative survival rate was calculated using the life table method. Between-group survival differences were assessed using the log-rank test. Univariate Cox regression models were implemented, followed by multivariate Cox regression models to identify factors correlated with mortality. Variables exhibiting a p-value less than 0.2 in the univariate analysis were incorporated into the multivariate Cox regression model. Statistical significance was set at a p-value of 0.05.
A nomogram model was constructed based on the statistically significant variables identified in the multivariate Cox regression. Pearson’s correlation coefficient was used to exclude highly correlated variables. A stepwise forward selection method was used, with a significance threshold of p < 0.05. Following the standardization of the regression coefficients, each patient’s total score was utilized to estimate the survival probability at 1, 3, and 5 years. The predictive performance of the nomogram was primarily assessed in terms of discrimination. We reported Harrell’s concordance index (C-index) and the corresponding Somers’ D statistic. In addition, time-specific discrimination was evaluated using receiver operating characteristic (ROC) analysis, and the areas under the curve (AUCs) were calculated at 1, 3, and 5 years.
3. Results
In total, 418 eligible patients were recruited. At the end of the study, 89 patients died, 215 were alive, and 114 were censored. The clinical characteristics of the patients are summarized in Table 1. The median age of the patients was 49 years (range: 16–74). More than 75% of the patients had CA-125 level of ≥35 U/mL. Nearly two-thirds of the patients had favorable KELIM results. More than three-quarters of the patients were diagnosed at an early stage (FIGO stage I-II). Most patients (90%) underwent primary debulking surgery (PDS) and radical surgery. The response rate to the primary treatment was very high (93.8%). The median time from surgery to initiation of adjuvant chemotherapy (TTC) was 20 days (IQR 7; range 5–229), consistent with our institutional 3-week scheduling protocol.
The median follow-up time was 77.1 months (range: 5.7–121.6 months). The cumulative mortality rates at 1, 3, and 5 years were 1.4% [95% CI: 0.7–3.2], 10.4% [95% CI: 7.8–13.8], and 16.5% [95% CI: 13.2–20.6] respectively (Table 2).
Ten covariates that demonstrated a significant association with survival were identified using the univariate Cox regression analysis. To maintain model stability and prevent overfitting, the subsequent multivariate model’s variable selection adhered to the guidelines of a minimum of ten events per predictor variable. Given the observed 89 instances of mortality, a set of eight variables was incorporated into the multivariate model. To preserve the model’s ability to offer early prognostic information, variables pertaining to treatment response and total chemotherapy cycles were excluded, as the determination of these factors necessitates completion of the primary treatment regimen.
Multivariate Cox model results showed that factors increasing the risk of death included unfavorable KELIM, HR = 1.78 [95% CI: 1.16–2.72]; pre-treatment CA-125 ≥ 35 U/mL, HR = 2.47 [95% CI: 1.10–5.55]; advanced-stage cancer (FIGO III-IV), HR = 2.40 [95% CI: 1.36–4.21]; and residual tumor tissue after debulking surgery, HR = 3.14 [95% CI: 1.75–5.65] (Table 3).
Overall survival in the favorable KELIM group was better than that in the unfavorable KELIM group. This difference was statistically significant, with p < 0.001 (log-rank test). At 1 year, the survival rates in the favorable KELIM group and the unfavorable KELIM group were 99.3% and 97.2%, respectively. At 3 years, the survival rates in the favorable KELIM group and the unfavorable KELIM group were 94.7% and 80.1%, respectively. At 5 years, the survival rates in the favorable KELIM group and the unfavorable KELIM group were 87.4% and 76.1%, respectively (Figure 1).
Pearson’s correlation coefficients were computed for factors exhibiting significant associations in the multivariate Cox regression model. These analyses revealed negligible collinearity among the identified predictors. Employing a stepwise forward selection strategy, all variables demonstrated statistical significance, with p-values below 0.05. Consequently, these four contributing factors were incorporated into the multivariate Cox regression model, which was subsequently utilized in the nomogram (Figure 2). The predictive performance of the model was evaluated using Harrell’s C-index and Somers’ D statistic. The C-index was 0.7628 and the associated Somers’ D value was 0.5256. These findings suggest a noteworthy ability to differentiate patients based on their survival prospects.
4. Discussion
The modeled KELIM has been established as a dynamic marker of intrinsic chemosensitivity derived from early CA-125 kinetics during platinum-based chemotherapy. Across multiple datasets, KELIM has shown consistent prognostic value for progression-free survival and overall survival, supporting its role as an early, treatment-informed biomarker beyond static baseline variables [6,7,10,13]. In addition to survival prognostication, KELIM has been investigated for clinically actionable applications in treatment planning. Several studies in advanced-stage disease treated with neoadjuvant chemotherapy have reported that favorable KELIM is associated with a higher probability of achieving complete interval debulking surgery [14], suggesting potential value as a triage tool to anticipate surgical outcomes. Moreover, exploratory trial-based analyses have evaluated KELIM as a complementary biomarker for treatment selection, including identifying subgroups more likely to benefit from PARP inhibitor strategies [15], highlighting its potential role in contemporary maintenance decision frameworks.
The median KELIM value observed in this investigation was 1.1, with a range spanning from 0.3 to 2.3. The incidence of unfavorable KELIM results was 34.5%, which was demonstrably lower than that reported in previous research, which varied between 47.2% and 67.4% [3,7,16]. Among advanced cancer in this study, the unfavorable KELIM rate was 41.8%. This figure aligns with the range of 19.0–58.1% found in alternative publications [17,18]. A lack of uniformity characterized the distribution of favorable and unfavorable KELIM rates across the reviewed literature. Nevertheless, a shared observation across several investigations, including this one, was the predominance of favorable KELIM outcomes. This indicates that the majority of the patients exhibited a positive response to chemotherapy. This finding corroborates with our study’s robust treatment response rate of 93.8%.
The high proportion of early-stage disease and optimal cytoreduction observed in our study reflects institutional referral patterns. At Tu Du Hospital, advanced-stage patients with high tumor burden or anticipated surgical complexity are commonly referred to tertiary oncology centers for specialized treatment. This referral model inherently selects for patients suitable for primary surgery, contributing to favorable baseline characteristics. Our findings are consistent with those reported by Nguyen et al. (2022) [19], who also documented a predominance of early-stage EOC in a cohort treated at the same institution. This alignment reinforces the internal validity of our stage distribution and highlights the systematic influence of our center’s treatment policy. Nevertheless, this selection bias may amplify the apparent prognostic strength of tumor biology markers such as KELIM. Therefore, caution should be exercised when extrapolating our results to broader or more advanced-stage EOC populations, where survival is more critically influenced by surgical feasibility and perioperative factors.
The relatively long median follow-up (77.1 months) strengthens the reliability of the reported 5-year overall survival estimates. The 1-year, 3-year, and 5-year survival rates in our study were 98.6, 89.6, and 83.5%, respectively. The survival rates in our study were higher than those reported in other countries. The US ovarian cancer statistics (2018) showed that the 5-year survival rate of EOC in Asian/Pacific Islanders is 57% [1]. A UK study (2022) showed that the 1-year and 5-year survival rates were 76% and 38%, respectively [20]. A Chinese study by Bai et al. (2023) showed that the 1-year, 3-year, and 5-year survival rates of 76%, 59%, and 45%, respectively [21]. In the early-stage cancer group, the 5-year survival rate was 90.4%. This rate is comparable to that of some studies, with 5-year survival rates ranging from 89.8% to 94.5% [22,23]. The survival rates in our study were generally higher than those reported in previous studies. This difference may be because our study included a large number of patients diagnosed at an early stage (75.4%) who achieved optimal debulking surgery (91.9%).
Multivariate regression analysis identified four independent predictors of survival duration: KELIM level, pretreatment CA-125 concentration, cancer stage, and the presence of residual tumor tissue following surgical intervention. These prognostic indicators are consistent with the findings of extensive large-scale and multicenter investigations. [7,16,24,25] Consequently, the results of the present investigation align with established trends concerning factors associated with survival outcomes of patients with epithelial ovarian cancer (EOC).
Pretreatment CA-125 is an easily accessible biomarker that supports risk assessment and prognosis at the time of diagnosis. In addition to our study, other studies have also noted the prognostic role of CA-125 in survival, such as the pooled analysis of Wang et al. (2022) that recorded HR = 1.62 [95% CI: 1.27–2.06] [25]. However, some studies have denied the prognostic role of pretreatment CA-125 levels [26,27].
The cancer stage and residual tumor tissue after debulking surgery have a strong impact on survival. Patients diagnosed with advanced-stage disease have a 1.78- to 10-fold increased risk of death compared to those diagnosed with early-stage disease [7,16,28]. The difference in the impact of cancer stage on survival between studies may be due to differences in study populations or the choice of covariates for the multivariate Cox models. Optimal debulking surgery is an important goal in EOC treatment. Residual tumor tissue after surgery is a strong prognostic factor for survival [16,17,21,24]. Achieving a tumor-free postoperative course reflects surgical skill. It is also related to the cancer stage, histology, and response to preoperative chemotherapy.
Although residual disease status was included in the multivariate model as a surrogate for surgical outcome, we acknowledge that it may not fully capture the nuances of surgical effort or intraoperative complexity. At our institution, surgical procedures are comprehensively documented through standardized operative protocols; however, validated surgical complexity scoring systems—such as the Surgical Complexity Score [29]—were not routinely adopted during the study period. Consequently, while data on the extent of resection were available, the lack of a quantitative surgical complexity index limited our ability to include this variable in prognostic modeling. Future studies should incorporate formal scoring systems to evaluate the prognostic interaction between surgical effort, tumor biology, and survival outcomes.
The generally short TTC and limited variability in our cohort may partly explain the lack of association between TTC and overall survival, in contrast to advanced-stage cohorts where greater surgical burden and postoperative morbidity more frequently lead to treatment delays [30].
Postoperative morbidity and 30-day perioperative mortality were reviewed in our cohort. Complications were rare (two intraoperative bladder injuries with good recovery), and no 30-day deaths due to surgical complications were observed. This likely reflects the predominance of early-stage, surgically favorable cases, in contrast to advanced-stage cohorts characterized by higher operative burden and greater complication variability [31]; therefore, postoperative morbidity was not included as a covariate due to insufficient event frequency.
KELIM is a dynamic marker with increasingly recognized prognostic value [7,16,17,24]. Patients with favorable KELIM have a 44% to 54% lower risk of death than those with unfavorable KELIM [7,16]. Our study found that the unfavorable KELIM group had a 1.78-fold increased risk of death, which is similar to the study by Lazar et al. [17]. The consistency of KELIM across studies confirms the value of KELIM in accurate risk stratification, supporting prognosis and patient follow-up strategies.
The results of the nomogram score analysis reflected the impact of the following factors on survival prognosis: unfavorable KELIM (2.7 points), favorable KELIM (0.0 points), pre-treatment CA-125 ≥ 35 U/mL (8.6 points), CA-125 < 35 U/mL (4.3 points), advanced-stage cancer (8.3 points), early-stage cancer (4.2 points), residual tumor tissue after surgery (10.0 points), and no residual tumor tissue (5.0 points). For example, if a patient is diagnosed with EOC with a pretreatment CA-125 level of 50 U/mL, FIGO stage II, KELIM score of 1.2, and no residual tumor tissue after debulking surgery. The patient’s total score is 8.7 + 4.2 + 0.0 + 5.0 = 17.9 points. Referring to the chart, the patient’s 1-year, 3-year, and 5-year survival rates are 98%, 94%, and 90%, respectively.
We used the scores calculated from the nomogram model to calculate the scores for all patients in the study. The total score had a median of 17.8 points (range: 13.5–29.6). The areas under the ROC curves at 1, 3, and 5 years were 0.8617, 0.810, and 0.8023, respectively, indicating that the nomogram model had good discrimination ability. This confirms the practical value of the model for personalized survival prediction.
In our cohort, KELIM remained independently associated with overall survival and added prognostic information when integrated with key clinicopathologic factors (pretreatment CA-125, FIGO stage, and residual tumor postsurgery). Accordingly, the developed nomogram enables individualized estimation of 1-, 3-, and 5-year OS, which may support patient counseling, risk stratification, and follow-up planning in settings where molecular profiling (e.g., BRCA/HRD) is not routinely available.
Limitations of study: Several constraints were present within the scope of this investigation. Initially, the retrospective nature of the study design introduced the potential for inaccuracies stemming from data recording. Furthermore, the analysis did not include a separate examination of the individual histological subtypes of epithelial ovarian cancer (EOC). Third, our cohort was enriched for early-stage, surgically favorable EOC due to our institutional referral model, which may limit generalizability to advanced-stage populations. External validation in tertiary cancer centers is warranted. Fourth, our analysis did not account for maintenance therapies. During the study period (2015–2019), PARP inhibitors were not yet approved for clinical use in Vietnam and were not available in routine practice at our institution. Although bevacizumab was permitted, retrospective data on its administration were not consistently documented. Consequently, the survival model presented in this study reflects outcomes in the pre-maintenance era and may not capture survival improvements attributable to contemporary maintenance strategies. Lastly, the dataset from Tu Du Hospital lacked information regarding biomarkers, including BRCA1/2 and Homologous Recombination Deficiency (HRD) status, owing to site-specific clinical practices and treatment protocols. These markers are becoming increasingly critical for personalized treatment strategies and prognostic assessments.
5. Conclusions
The present investigation documented one-year, three-year, and five-year survival rates for EOC patients in Southern Vietnam, yielding figures of 98.6%, 89.6%, and 83.5%, respectively. Determinants significantly associated with patient survival included the KELIM score, pretreatment CA-125 levels, cancer stage, and the presence of residual tumor following cytoreductive surgery. To broaden the scope of the analysis, future research concerning EOC patients in Southern Vietnam will incorporate assessments of BRCA1/2 status and homologous recombination deficiency (HRD).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Torre L.A. Trabert B. De Santis C.E. Miller K.D. Samimi G. Runowicz C.D. Gaudet M.M. Jemal A. Siegel R.L. Ovarian cancer statistics, 2018 CA Cancer J. Clin.20186828429610.3322/caac.2145629809280 PMC 6621554 · doi ↗ · pubmed ↗
- 2Ferlay J.E.M. Lam F. Laversanne M. Colombet M. Mery L. Piñeros M. Znaor A. Soerjomataram I. Bray F. Global Cancer Observatory: Cancer Today Available online: https://gco.iarc.who.int/today(accessed on 1 February 2024)
- 3Lauby A. Colomban O. Corbaux P. Peron J. Van Wagensveld L. Gertych W. Bakrin N. Descargues P. Lopez J. Kepenekian V. The Increasing Prognostic and Predictive Roles of the Tumor Primary Chemosensitivity Assessed by CA-125 Elimination Rate Constant K (KELIM) in Ovarian Cancer: A Narrative Review Cancers 2021149810.3390/cancers 1401009835008262 PMC 8750686 · doi ↗ · pubmed ↗
- 4Lu H.Y. Tai Y.J. Chen Y.L. Chiang Y.C. Hsu H.C. Cheng W.F. Ovarian cancer risk score predicts chemo-response and outcome in epithelial ovarian carcinoma patients J. Gynecol. Oncol.202132 e 1810.3802/jgo.2021.32.e 1833327048 PMC 7930441 · doi ↗ · pubmed ↗
- 5Hu J. Jiao X. Zhu L. Guo H. Wu Y. Establishment and verification of the nomogram that predicts the 3-year recurrence risk of epithelial ovarian carcinoma BMC Cancer 20202093810.1186/s 12885-020-07402-232993522 PMC 7526363 · doi ↗ · pubmed ↗
- 6You B. Colomban O. Heywood M. Lee C. Davy M. Reed N. Pignata S. Varsellona N. Emons G. Rehman K. The strong prognostic value of KELIM, a model-based parameter from CA 125 kinetics in ovarian cancer: Data from CALYPSO trial (a GINECO-GCIG study)Gynecol. Oncol.201313028929410.1016/j.ygyno.2013.05.01323694718 · doi ↗ · pubmed ↗
- 7Corbaux P. You B. Glasspool R.M. Yanaihara N. Tinker A.V. Lindemann K. Ray-Coquard I.L. Mirza M.R. Subtil F. Colomban O. Survival and modelled cancer antigen-125 ELI Mination rate constant K score in ovarian cancer patients in first line before poly(ADP-ribose) polymerase inhibitor era: A Gynaecologic Cancer Intergroup meta-analysis Eur. J. Cancer 202319111296610.1016/j.ejca.2023.11296637542936 · doi ↗ · pubmed ↗
- 8Berek J.S. Renz M. Kehoe S. Kumar L. Friedlander M. Cancer of the ovary, fallopian tube, and peritoneum: 2021 update Int. J. Gynecol. Obstet.2021155618510.1002/ijgo.13878 PMC 929832534669199 · doi ↗ · pubmed ↗