Sleep Disturbance Among Nurses in Al-Dakhiliyah Governorate, Oman
Abdullah Al Nabhani, Mohammed Al Harrasi, AlSalt Al Tubi, Ali Z Al Busaidi, Khalil Al Kharusi, Taleb Al Busaidi, Iman Al Furqani

TL;DR
This study found that nearly a quarter of nurses in Oman experience clinically significant insomnia, with medical conditions and nationality as key predictors.
Contribution
The study identifies specific predictors of insomnia among nurses in Oman, including nationality and medical illness, which were not previously well-documented in this population.
Findings
24.0% of nurses had clinically significant insomnia, and 33.6% had subthreshold insomnia.
Non-Omani nationality and presence of medical illness were significant predictors of insomnia severity.
Night shifts were common but not independently linked to insomnia severity.
Abstract
Background: Nurses are at high risk of insomnia due to demanding schedules and psychosocial stressors. We investigated the prevalence, severity, and predictors of insomnia among nurses working in Al-Dakhiliyah Governorate, Oman. Methods: A cross-sectional survey of registered nurses (n=271) used a demographic/work-related questionnaire and the 7-item Insomnia Severity Index (ISI). Descriptive statistics, t-tests/ANOVA, and multiple linear regression were used (α=0.05). An online link was sent to the nurses, directing them to a Google Forms survey. The form included an informed consent section, a brief explanation of the study, and a statement emphasizing the anonymity of their responses. Results: Clinically significant insomnia (ISI≥15) affected 24.0% of nurses, while 33.6% had subthreshold insomnia. Mean ISI was 9.46±6.30 (subthreshold range). In adjusted models (R²=0.253; adjusted…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4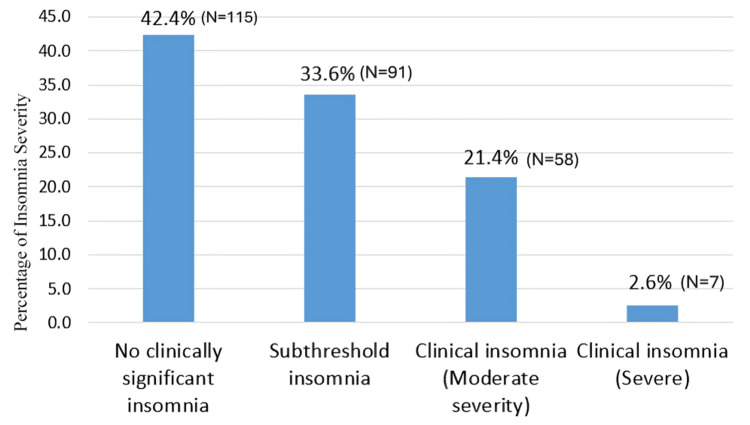 Figure 5
Figure 5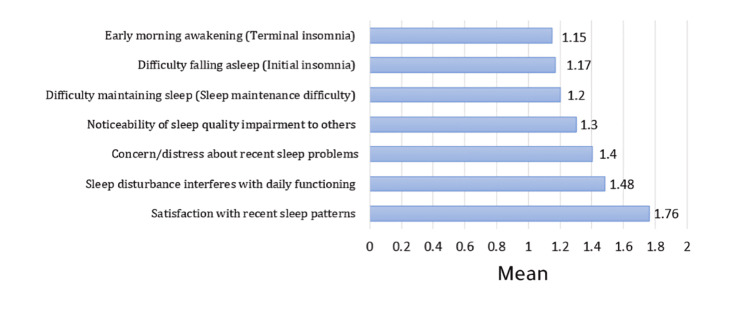 Figure 6
Figure 6| Nurses’ characteristics | Category | Frequency | Percentage |
| Nationality | Omani | 99 | 36.5% |
| Non-Omani | 172 | 63.5% | |
| Workplace | Local HC | 26 | 9.6% |
| Polyclinic | 11 | 4.1% | |
| Hospital | 234 | 86.3% | |
| Gender | Male | 36 | 13.3% |
| Female | 235 | 86.7% | |
| How many years worked as a nurse? | 1-4 | 28 | 10.3% |
| 5-9 | 52 | 19.2% | |
| 14-10 | 77 | 28.4% | |
| 15-20 | 86 | 31.7% | |
| 21-30 | 28 | 10.3% | |
| Age group | 20-29 | 27 | 10.0% |
| 30-39 | 163 | 60.1% | |
| 40-49 | 76 | 28.0% | |
| 50-59 | 5 | 1.8% | |
| Above 60 | 0 | 0.0% | |
| How many years worked as a nurse at the current department? | 1-5 | 155 | 57.2% |
| 6-10 | 43 | 15.9% | |
| 11-15 | 45 | 16.6% | |
| 16-20 | 16 | 5.9% | |
| 21-25 | 9 | 3.3% | |
| 26-30 | 3 | 1.1% | |
| Marital status | Married | 250 | 92.3% |
| Single | 19 | 7.0% | |
| Divorce | 2 | 0.7% | |
| Number of children | 0 | 36 | 13.8% |
| 1 | 64 | 24.6% | |
| 2 | 89 | 34.2% | |
| 3 | 41 | 15.8% | |
| 4 | 23 | 8.8% | |
| 5 | 7 | 2.7% | |
| >=6 | 11 | 4.1% | |
| Do you work night shifts? | Yes | 228 | 84.1% |
| No | 43 | 15.9% | |
| Do you have any medical illness that prevents you from falling asleep or continuing? | Yes | 56 | 20.7% |
| No | 215 | 79.3% | |
| If yes, choose one | HTN | 10 | 17.9% |
| DM | 3 | 5.4% | |
| Pain | 26 | 46.4% | |
| Other | 14 | 25.0% | |
| I don't have any medical illness | 3 | 5.4% | |
| Have you taken any sleeping pills for the last 3 months? | Yes | 18 | 6.6% |
| No | 253 | 93.4% | |
| If yes, how frequently per week? | Zero/week | 38 | 15.0% |
| Once/week | 0 | 0.0% | |
| 2 times/week | 1 | 0.4% | |
| 3 times/week | 0 | 0.0% | |
| Equal to or more than 4 times/week | 2 | 0.8% | |
| I haven't taken any sleeping pills for the last 3 months | 212 | 83.8% |
| ISI Category | Frequency | Percentage |
| No clinically significant insomnia (0-7) | 115 | 42.4 % |
| Subthreshold insomnia (8-14) | 91 | 33.6% |
| Moderate clinical insomnia (15-21) | 58 | 21.4% |
| Severe clinical insomnia (22-28) | 7 | 2.6% |
| Total | 271 | 100.0% |
| Item | Mean | SD |
| Difficulty falling asleep (initial insomnia) | 1.17 | 1.08 |
| Difficulty maintaining sleep (sleep maintenance difficulty) | 1.20 | 1.00 |
| Early morning awakening (terminal insomnia) | 1.15 | 1.05 |
| Satisfaction with recent sleep patterns | 1.76 | 1.19 |
| Sleep disturbance interferes with daily functioning | 1.48 | 1.09 |
| Noticeability of sleep quality impairment to others | 1.30 | 1.04 |
| Concern/distress about recent sleep problems | 1.40 | 1.17 |
| Total ISI | 9.46 | 6.30 |
| Variable | Category | N | (%) | Mean | SD | t/F-Test | p-value | Interpretation |
| Nationality | Omani | 99 | 36.5 | 11.8 | 5.4 | t=4.84 | <0.001 | Statistically significant |
| Non-Omani | 172 | 63.5 | 8.11 | 6.4 | ||||
| Workplace | Local H.C | 26 | 9.6 | 10.38 | 5.32 | F=1.59 | 0.227 | Not statistically significant |
| Polyclinic | 11 | 4.1 | 12.36 | 6.53 | ||||
| Hospital | 234 | 86.3 | 9.22 | 6.37 | ||||
| Gender | Male | 36 | 13.3 | 8.69 | 5.98 | t=-0.78 | 0.434 | Not statistically significant |
| Female | 235 | 86.7 | 9.58 | 6.35 | ||||
| How many years worked as a nurse? | 1-4 | 28 | 10.3 | 8.75 | 6.1 | F=0.531 | 0.713 | Not statistically significant |
| 5-9 | 52 | 19.2 | 9.94 | 6.38 | ||||
| 10-14 | 77 | 28.4 | 9.74 | 6.85 | ||||
| 15-20 | 86 | 31.7 | 8.87 | 5.82 | ||||
| 21-30 | 28 | 10.3 | 10.32 | 6.41 | ||||
| Age group | 20-29 | 27 | 10.0 | 10.59 | 5.57 | F=0.78 | 0.52 | Not statistically significant |
| 30-39 | 163 | 60.1 | 9.01 | 6.28 | ||||
| 40-49 | 76 | 28.0 | 10 | 6.64 | ||||
| 50-59 | 5 | 1.8 | 10 | 5.7 | ||||
| How many years worked as a nurse at the current department? | 1-5 | 155 | 57.2 | 8.97 | 6.26 | F=1.09 | 0.402 | Not statistically significant |
| 6-10 | 43 | 15.9 | 9.23 | 6.5 | ||||
| 11-15 | 45 | 16.6 | 10.62 | 5.96 | ||||
| 16-20 | 16 | 5.9 | 12.38 | 6.43 | ||||
| 21-25 | 9 | 3.3 | 8.11 | 7.36 | ||||
| 26-30 | 3 | 1.1 | 9.33 | 4.93 | ||||
| Marital status | Married | 250 | 92.3 | 9.52 | 6.29 | F=0.11 | 0.898 | Not statistically significant |
| Single | 19 | 7.0 | 8.74 | 6.23 | ||||
| Divorce | 2 | 0.7 | 9 | 12.73 | ||||
| Number of children | 0 | 36 | 13.3 | 9 | 6.12 | F=2.22 | 0.057 | Not statistically significant |
| 1 | 64 | 23.6 | 8.45 | 5.4 | ||||
| 2 | 89 | 32.8 | 8.98 | 6.82 | ||||
| 3 | 41 | 15.1 | 10.24 | 6.59 | ||||
| 4 | 23 | 8.5 | 11.09 | 6.22 | ||||
| 5 | 7 | 2.6 | 13.71 | 3.99 | ||||
| >=6 | 11 | 4.1 | 11.73 | 6.63 | ||||
| Work night shifts | No | 43 | 15.9 | 11 | 5.76 | t=1.7 | 0.091 | Not statistically significant |
| Yes | 228 | 84.1 | 9.18 | 6.37 | ||||
| Do you have any medical illnesses? | No | 215 | 79.3 | 8.31 | 6.02 | t=-6.32 | <0.001 | Statistically significant |
| Yes | 56 | 20.7 | 13.9 | 5.35 | ||||
| Have you taken any sleeping pills for the last 3 months? | No | 253 | 93.4 | 9.08 | 6.26 | t=-3.84 | <0.001 | Statistically significant |
| Yes | 18 | 6.6 | 14.8 | 4.18 |
| R | R² | Adjusted R² | Std. error estimate |
| 0.5030 | 0.2530 | 0.1521 | 5.8179 |
| Parameter | Non standard coef beta | Standard coef beta | Std. error | t | p-value | 95% CI | ||
| lower bound | upper bound | |||||||
| Constant | 6.89 | - | 5.35 | 1.29 | 0.2 | -3.7 | 17.4 | |
| Nationality (reference: Omani) | ||||||||
| Non-Omani | -2.7 | -0.2 | 1.23 | -2.2 | 0.03 | -5.2 | -0.3 | |
| Workplace (reference: polyclinic) | ||||||||
| Hospital | -0.9 | -0.1 | 2.11 | -0.4 | 0.66 | -5.1 | 3.22 | |
| Local HC | -1.6 | -0.1 | 2.29 | -0.7 | 0.48 | -6.1 | 2.89 | |
| Gender (reference: male) | ||||||||
| Gender female | 2.22 | 0.12 | 1.28 | 1.74 | 0.08 | -0.3 | 4.75 | |
| Years worked as a nurse (reference: 1-4) | ||||||||
| 5-9 years | 3.37 | 0.21 | 1.74 | 1.94 | 0.05 | -0.1 | 6.8 | |
| 10-14 years | 2.9 | 0.21 | 1.82 | 1.59 | 0.11 | -0.7 | 6.5 | |
| 15-20 years | -0.1 | 0 | 1.96 | -0.1 | 0.96 | -4 | 3.75 | |
| 21-30 years | 0.62 | 0.03 | 2.61 | 0.24 | 0.81 | -4.5 | 5.77 | |
| Age group (reference: 20-29) | ||||||||
| 30-39 years | -2.5 | -0.2 | 1.79 | -1.4 | 0.16 | -6.1 | 1 | |
| 40-49 years | -1.1 | -0.1 | 2.13 | -0.5 | 0.61 | -5.3 | 3.1 | |
| 50-59 years | 0.46 | 0.01 | 4.15 | 0.11 | 0.91 | -7.7 | 8.64 | |
| Years in at current department (reference: 1-5) | ||||||||
| 6-10 years | 0.42 | 0.02 | 1.1 | 0.38 | 0.7 | -1.7 | 2.59 | |
| 11-15 years | 1.35 | 0.08 | 1.16 | 1.16 | 0.25 | -0.9 | 3.64 | |
| 16-20 years | 1.32 | 0.05 | 1.91 | 0.69 | 0.49 | -2.4 | 5.08 | |
| 21-25 years | -1.8 | 0 | 2.57 | -0.7 | 0.49 | -6.9 | 3.27 | |
| 26-30 years | -4.8 | -0.1 | 4.69 | -1 | 0.31 | -14 | 4.47 | |
| Marital status (reference: divorced) | ||||||||
| Married | -0.5 | 0 | 4.38 | -0.1 | 0.91 | -9.1 | 8.15 | |
| Single | -1.7 | -0.1 | 4.9 | -0.4 | 0.72 | -11 | 7.93 | |
| Number of children (reference: 0) | ||||||||
| 1 | -1.2 | -0.1 | 1.63 | -0.7 | 0.48 | -4.4 | 2.04 | |
| 2 | 0.72 | 0.05 | 1.58 | 0.45 | 0.65 | -2.4 | 3.83 | |
| 3 | 0.47 | 0.03 | 1.82 | 0.26 | 0.8 | -3.1 | 4.07 | |
| 4 | 0.53 | 0.02 | 2.26 | 0.23 | 0.82 | -3.9 | 4.99 | |
| 5 | 3.25 | 0.08 | 3.03 | 1.07 | 0.29 | -2.7 | 9.22 | |
| >=6 | 1.96 | 0.06 | 3.07 | 0.64 | 0.52 | -4.1 | 8 | |
| Do you work night shifts (reference: no) | ||||||||
| Yes | 1.55 | 0.09 | 1.5 | 1.03 | 0.3 | -1.4 | 4.49 | |
| Medial illness (reference: no) | ||||||||
| Yes | 4.32 | 0.28 | 1.04 | 4.15 | < 0.001> | 2.27 | 6.37 | |
| Sleeping pills (reference: no) | ||||||||
| Yes | 2.9 | 0.11 | 1.69 | 1.72 | 0.09 | -0.4 | 6.22 | |
| How frequent per week (reference: 0) | ||||||||
| 2 times/week | 2.62 | 0.03 | 6.04 | 0.43 | 0.67 | -9.3 | 14.5 | |
| >=4 times/week | -0.5 | 0 | 4.59 | -0.1 | 0.91 | -9.6 | 8.52 | |
| I don't take | 1.68 | 0.1 | 1.1 | 1.53 | 0.13 | -0.5 | 3.85 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSleep and Work-Related Fatigue · Sleep and related disorders · Nursing education and management
Introduction
Insomnia-difficulty initiating, maintaining sleep or dissatisfaction with sleep despite adequate opportunity-impairs cognition, vigilance and well-being, and increases risk of errors and burnout in healthcare providers [1,2,3,4]. The Sultanate of Oman’s health system relies heavily on nurses across hospitals and primary care [1,2]. Nurses in Al-Dakhiliyah Governorate face unique occupational and sociocultural demands that may predispose them to sleep disturbance [3]. Recent evidence highlights that insomnia and fatigue among healthcare workers are driven not only by long working hours but also by systemic factors such as workload intensity and irregular shifts, which substantially impair alertness and well-being [5]. Effective fatigue-management strategies in healthcare settings, like meditation, have been shown to reduce sleep-related impairment, emphasizing the need for organizational policies that support adequate rest and recovery [1,5]. In parallel, behavioral interventions such as mindfulness meditation have demonstrated significant improvements in sleep quality, suggesting that non-pharmacological approaches can play a critical role in addressing insomnia among healthcare staff [6]. Randomized trial evidence shows that mindfulness-based practices reduce insomnia symptoms by lowering physiological arousal and enhancing stress regulation, offering a promising method for sleep enhancement in high-stress professions such as nursing [5,6]. This study, therefore, aims to determine the prevalence and severity of insomnia among nurses working in Al-Dakhiliyah Governorate, to examine the demographic and occupational factors associated with insomnia among nurses and to propose evidence-based strategies to reduce insomnia and improve sleep quality among nurses.
Materials and methods
Study design and time period
A descriptive, quantitative, cross-sectional study design was employed to determine the prevalence and associated factors of insomnia among registered nurses. The study was conducted in the Al Dakhiliyah Governorate of the Sultanate of Oman, encompassing government hospitals and primary health centres within the region. The study was conducted during October and November 2025.
Setting, sampling and participants
The study population consisted of all registered nurses currently employed in government hospitals and primary health centres across the Al-Dakhiliyah Governorate, Oman. The estimated total number of eligible nurses was approximately 1,800. A stratified random sampling technique was adopted to ensure proportional representation of nurses from different healthcare settings (hospitals and primary health centres). The sample size was calculated using Cochran’s formula with a finite population correction (FPC), based on an expected prevalence, a 95% confidence level, and a 6% margin of error. The minimum required sample size was 233. To account for a potential 10% non-response rate, the final target sample size was increased to 258 participants. Ultimately, 271 nurses participated. Nursing supervisors, students, interns, and administrative staff were excluded.
Data collection and measures
Data were collected between October and November 2025 using a structured self-administered Google Form (Appendix A). The survey consisted of sociodemographic and occupational variables (age, gender, nationality, marital status, number of children, years of experience, workplace level, night shift duties, medical illness, and use of sleep medication), and the validated seven-item Insomnia Severity Index (ISI) [7]. Each item is scored 0-4, yielding a total score range 0-28, with established cut-points (0-7 no insomnia, 8-14 subthreshold, 15-21 moderate, 22-28 severe).
Statistical analysis
Data analysis was conducted in SPSS Statistics (IBM Corp., 2019 IBM SPSS Statistics for Windows Version 26.0), and the results were displayed in the format of charts and tables. Descriptive statistics were used to summarize the data. To assess the normality of the ISI score, skewness and kurtosis values were examined, along with graphical methods such as histograms and Q-Q plots. Given the normal distribution of this variable, t-tests and ANOVA were utilized to explore the relationship between ISI score and background characteristics. Subsequently, variables were incorporated into a multiple linear regression analysis to identify predictors of ISI scores. A significance level of p<0.05 was established for all statistical tests.
Ethical considerations
Institutional approval for conducting the research was obtained from the Research and Ethical Review and Approval Committee, Al-Dakhliya Governorate, Ministry of Health, Sultanate of Oman, with approval number MоH/CSR/25/3099. Participation was voluntary, without incentives. Submission of the online survey constituted implied consent, and no identifying personal data was collected.
Results
Sociodemographic characteristics of participants
A total of 271 nurses from Al-Dakhaliah Governorate participated in the study. Table 1 summarizes their demographic profile. The table shows that the majority of participants were Non-Omani (N=172, 63.5%), while 36.5% (N=99) were Omani.
This can be seen as well in Figure 1.
Nurses nationality distribution.
Most participants worked in hospital settings (N=234, 86.3%), followed by local health centres (N=26, 9.6%) and polyclinics (N=11, 4.1%) (Figure 2).
Workplace distribution.Local H.C: local health centre.
A large proportion of respondents were female (N=235, 86.7%), while 13.3% (N=36) were male (Figure 3).
Gender distribution.
Regarding experience, most nurses had worked 15-20 years (N=86, 31.7%), and the largest age group was 30-39 years (N=163, 60.1%). Over half of the participants (N=155, 57.2%) had been working in their current department for 1-5 years, and a majority were married (N=250, 92.3%). About 61.1% (N=171) of nurses had more than one child. The vast majority (N=228, 84.1%) reported working night shifts (Figure 4), and 20.7% (N=57) had a medical illness affecting their sleep. Among those, pain (46.4%) was the most common condition. Only 6.6% (N=18) reported using sleeping pills during the last three months, and most of them used these less than once per week.
Night shifts duties distribution.
Prevalence and severity of insomnia among nurses in Al-Dakhaliah Governorate
Table 2 summarizes the prevalence and severity of insomnia. ISI total scores showed: 42.4% (N=115) had no clinically significant insomnia (ISI: 0-7), 33.6% (N=91) had subthreshold insomnia (ISI: 8-14), 21.4% (N=58) had moderate insomnia (ISI: 15-21), and 2.6% (N=7) had severe insomnia (ISI: 22-28).
Combined clinically significant insomnia (moderate + severe) was 24.0% (N=65) (Figure 5). This indicates that approximately one-quarter of the nurses had clinically significant insomnia and one-third had subthreshold insomnia, reflecting a substantial burden of sleep disturbance in this population.
Percentage of prevalence and severity of insomnia (Insomnia Severity Index).
Table 3 presents the means and standard deviations for each item of the ISI. Participants reported the highest severity on the item Satisfaction with recent sleep patterns (M=1.76, SD=1.19), suggesting lower satisfaction with their recent sleep quality.
The lowest severity was observed on early morning awakening (terminal insomnia) (M=1.15, SD=1.05), indicating fewer difficulties with waking up too early (Figure 6). The mean total ISI score was 9.46 (SD=6.30), which falls within the subthreshold insomnia range (8-14) according to standard ISI scoring guidelines. Overall, these findings suggest that participants experienced mild sleep difficulties, with dissatisfaction regarding sleep patterns being the most prominent concern.
Means of Insomnia Severity Index items (0-4).
The findings in Table 4 indicate that most demographic and work-related characteristics of nurses were not significantly associated with insomnia severity. Variables such as workplace setting, gender, age, years of nursing experience, years working in the current department, marital status, number of children, and night shift duties did not show any meaningful differences in ISI scores (p> 0.05 for all). In contrast, three variables demonstrated statistically significant relationships with insomnia severity. Omani nurses reported significantly higher insomnia scores than non-Omani nurses (p< 0.001), suggesting potential cultural, social, or work-related stress differences between groups. Nurses with a medical illness had markedly higher insomnia levels compared to those without medical conditions (p< 0.001), indicating that underlying health problems may intensify sleep disturbances. Additionally, those who reported using sleeping pills during the past three months had the highest ISI scores among all groups (p< 0.001), which may reflect more severe or persistent sleep problems that necessitate medication. Overall, while most background characteristics did not contribute to variations in insomnia severity, nationality, presence of medical illness, and sleeping pill usage emerged as key factors associated with significantly higher insomnia symptoms among nurses.
Table 5 presents the summary results of a multiple linear regression analysis conducted to determine the factors associated with insomnia severity among nurses, as measured by the ISI score. All variables were entered simultaneously to adjust for potential confounding effects. The overall model explained 25.3% of the variance in insomnia severity (R²=0.253), with an adjusted R² of 0.152, indicating a moderate level of explanatory power. After controlling for all other demographic and work-related variables, only two variables demonstrated statistically significant associations with insomnia severity: nationality and medical illness.
The findings in Table 6 indicate that after adjusting for all predictors, nationality and medical illness remained significant independent predictors of insomnia severity. Non-Omani nurses had lower insomnia scores than Omani nurses, while nurses with medical illnesses showed markedly higher levels of insomnia symptoms. No other demographic or work-related factors demonstrated significant associations in the final model. Non-Omani nurses had significantly lower ISI scores compared with Omani nurses (B=−2.7, p=0.028; 95% CI: −5.2 to −0.3). This suggests that being Omani is associated with greater insomnia symptoms. Nurses reporting a medical illness had significantly higher ISI scores than those without (B=4.32, p< 0.001; 95% CI: 2.27 to 6.37). This was the strongest predictor in the model (β=0.28).
Discussion
In the present study, medical illness and nationality emerged as the only significant predictors of insomnia severity among nurses after controlling for demographic and occupational variables. Nurses who reported having a medical illness experienced significantly higher insomnia scores [5]. This finding is consistent with previous studies indicating that chronic health conditions can impair sleep quality through physical discomfort, pain, stress, and psychological burden [6,8,9,10]. Nurses with existing health issues may also be more vulnerable to work-related strain, which can further exacerbate sleep disturbances [6,11]. Early identification and supportive workplace accommodations may therefore be critical to reduce sleep problems among this group [5,6,12,13].
Interestingly, non-Omani nurses demonstrated significantly lower insomnia severity compared with Omani nurses. This result contrasts with expectations, as expatriate nurses may commonly encounter stressors such as workload adaptation, homesickness, cultural challenges, and job insecurity [14,15]. One possible explanation is that non-Omani nurses may adopt more adaptive coping strategies or have stronger family or peer support systems. Alternatively, Omani nurses may be facing increased national responsibilities, societal expectations, or dual-role pressures within the home and workplace, leading to more sleep disruptions. Further qualitative research is recommended to explore these sociocultural factors [16,17].
Other demographic and work-related characteristics, such as age, gender, workplace setting, night shift status, and years of experience, were not significantly associated with insomnia in the final adjusted model. This suggests that insomnia among nurses may be more strongly driven by personal health conditions and psychosocial influences rather than routine workforce characteristics. It also indicates that common occupational assumptions, such as night shift work being the primary cause of poor sleep, may not fully capture the complexity of insomnia in this population [3,15]. The modest explanatory power of the model (adjusted R²=0.152) further suggests that additional relevant variables were not captured, such as occupational stress, burnout, staffing level, workload intensity, and mental health factors (e.g., anxiety and depression), which are known contributors to sleep disorders in nursing staff [6,12]. Future research should include a broader range of psychosocial predictors to better understand the multifactorial nature of insomnia among nurses.
Overall, the findings highlight the importance of addressing medical conditions and supporting Omani nurses who appear more susceptible to insomnia. Tailored sleep health interventions and workplace wellbeing programs may reduce the burden of sleep disturbances and enhance nursing performance and patient safety [1,2,4,18,19].
A comprehensive, multi-level strategy to guide insomnia treatment among nurses
Health Management
Routine screening and optimal management of chronic medical illnesses are essential to reduce physiological drivers of sleep disruption.
Stress Reduction
Evidence-based interventions such as Mindfulness-Based Stress Reduction (MBSR) and Cognitive Behavioral Therapy for Insomnia (CBT-I) should be implemented to address psychological stressors and maladaptive sleep behaviors.
Shift Scheduling
Forward-rotating shift systems, protected rest breaks, and access to designated rest areas can minimize circadian misalignment, a core mechanism in shift-work related insomnia.
Mental Health Support
Formal fatigue management and burnout prevention programs are critical for lowering insomnia severity and improving emotional resilience in high-demand work settings.
Medication Use
Pharmacotherapy should be considered adjunctive and time-limited. The gold-standard approach involves CBT-I combined with gradual tapering of hypnotics to reduce dependence and avoid rebound insomnia.
Cultural Sensitivity
Interventions should be culturally adapted, family-inclusive, and context-appropriate for Omani nurses to improve acceptability, engagement, and sustainability.
Recommendations
Comprehensive health screening and appropriate workplace accommodations should be provided for nurses living with chronic illnesses to support their well-being and job performance. Moreover, access to CBT-I and mindfulness-based programs may help reduce reliance on hypnotic medications while promoting healthier sleep patterns and implementing evidence-based rostering practices that ensure adequate recovery periods, along with education on sleep hygiene, can further optimize nurses’ sleep quality and overall functioning. Additionally, culturally tailored well-being initiatives, including family-inclusive supports, are particularly important for Omani nurses. Finally, future prospective studies should explore predictors such as burnout, workload, and mental health to better understand factors influencing sleep disturbances among nurses.
Strengths and limitations
This study is one of the very few investigations focusing specifically on sleep disturbance and insomnia among nurses working within the Al-Dakhiliyah Governorate. The use of a validated insomnia screening tool (Insomnia Severity Index) strengthens the reliability of the findings, and the inclusion of nurses from different levels of healthcare institutions (hospitals, polyclinics, and local health centres) increases the contextual relevance and representativeness of the results within the governorate. Additionally, the analysis applied both bivariate and multivariable regression techniques, allowing identification of independent predictors beyond basic demographic differences.
However, this study has limitations that should be acknowledged. First, data were collected using convenience sampling, which limits the generalizability of findings and may introduce response bias, particularly if nurses experiencing sleep disturbance were more motivated to participate. Second, the cross-sectional nature of the study prevents the determination of causality; thus, associations do not imply directionality. Third, data collection relied on self-reported measures, which may be affected by recall bias or social desirability bias. Finally, important psychosocial factors known to influence sleep, such as workload intensity, burnout, staffing adequacy, and mental health variables (anxiety, depression), were not measured in this study and may partially explain the unexplained variance in ISI scores. Future research should incorporate longitudinal designs, structured mental health screening, and objective sleep measures (e.g., actigraphy) to better understand the causal mechanisms underlying insomnia among nurses in Oman.
Conclusions
Insomnia was found to be a modest prevalent condition among nurses working in Al-Dakhiliyah Governorate, with many experiencing clinically significant insomnia and reporting subthreshold symptoms. Although most demographic and occupational variables were not associated with insomnia severity, both medical illness and nationality emerged as independent predictors. Nurses with chronic health conditions demonstrated markedly higher insomnia scores, underscoring the role of physical health in sleep disturbance. Furthermore, Omani nurses exhibited significantly higher insomnia severity than non-Omani nurses, suggesting that sociocultural and family-role pressures may contribute to sleep impairment within the local nursing workforce.
These findings highlight the need for targeted sleep health strategies within the Omani nursing system. Routine screening for chronic illness, incorporation of structured sleep-focused wellbeing initiatives, and access to evidence-based non-pharmacological interventions such as CBT-I may reduce insomnia burden and enhance occupational functioning. Future research should integrate longitudinal designs and include psychosocial, mental health, burnout, and workload factors to strengthen causal inference and guide intervention development. Improving sleep health in nurses is a strategic priority to protect workforce wellbeing and maintain the quality and safety of patient care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Epidemiology of insomnia: prevalence, self-help treatments, consultations, and determinants of help-seeking behaviors Sleep Med Morin CM Le Blanc M Daley M Gregoire JP Mérette C 123130720061645914010.1016/j.sleep.2005.08.008 · doi ↗ · pubmed ↗
- 2Individual vulnerability to insomnia, excessive sleepiness and shift work disorder amongst healthcare shift workers. A systematic review Sleep Med Rev Booker LA Magee M Rajaratnam SM Sletten TL Howard ME 2202334120182968017710.1016/j.smrv.2018.03.005 · doi ↗ · pubmed ↗
- 3Precarious work schedules and sleep: a study of unionized full-time workers Occup Health Sci Dugan AG Decker RE Zhang Y 247277620223537267110.1007/s 41542-022-00114-y PMC 8962924 · doi ↗ · pubmed ↗
- 4Sleep quality and its associated factors among nurses in Jimma Zone public hospitals, Southwest Ethiopia, 2018.Sleep Hyp Olana Olana D.DD.D Ayana A.M Abebe S.T 271280212019 https://sleepandhypnosis.org/research/ing/Pdf/c 4d 052b 8c 3b 0480 c 86187 f 995dcbda 7e.pdf
- 5Mindfulness meditation and improvement in sleep quality and daytime impairment among older adults with sleep disturbances: a randomized clinical trial JAMA Intern Med Black DS O'Reilly GA Olmstead R Breen EC Irwin MR 49450117520152568630410.1001/jamainternmed.2014.8081 PMC 4407465 · doi ↗ · pubmed ↗
- 6Fatigue risk management in healthcare: A scoping literature review Int J Nurs Stud Fox S Dall'Ora C Young M 10528217420254127389110.1016/j.ijnurstu.2025.105282 · doi ↗ · pubmed ↗
- 7The Insomnia Severity Index: psychometric indicators to detect insomnia cases and evaluate treatment response Sleep Morin CM Belleville G Bélanger L Ivers H 6016083420112153295310.1093/sleep/34.5.601PMC 3079939 · doi ↗ · pubmed ↗
- 8International classification of sleep disorders-third edition: highlights and modifications Chest Sateia MJ 1387139414620142536747510.1378/chest.14-0970 · doi ↗ · pubmed ↗