Branch Retinal Vein Occlusion Revealing Previously Undiagnosed Systemic Disease
Daria Valipur Kolti, Jakub Juszczyk, Sara Omidi, Julia Kierner, Dariusz Valipur Kolti

TL;DR
A case of sudden vision loss from a retinal vein block revealed hidden high blood pressure, highlighting the need for better coordination between eye doctors and general physicians.
Contribution
Highlights BRVO as a potential first sign of undiagnosed hypertension and identifies gaps in current systemic screening protocols.
Findings
BRVO can be the first clinical manifestation of undetected systemic hypertension.
Current referral protocols for RVO lack standardization, delaying essential systemic evaluations.
Multidisciplinary care combining ocular and systemic management is crucial to prevent complications.
Abstract
Branch retinal vein occlusion (BRVO) is a common cause of vision loss and frequently reflects an underlying systemic vascular disorder. Early systemic assessment is fundamental for preventing ocular and cardiovascular complications. This report describes the clinical case of a 61-year-old woman who presented with sudden, painless visual field loss in the left eye. Fundoscopic and angiographic findings confirmed superotemporal BRVO with macular edema. Intravitreal anti-vascular endothelial growth factor (VEGF) therapy was initiated, and referral to a primary care physician for systemic evaluation was requested. However, due to the absence of a standardized referral protocol, the patient did not undergo prompt assessment. One week after the initial ophthalmologic visit, she presented to the emergency department with a severe headache and was found to have a hypertensive crisis. This case…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
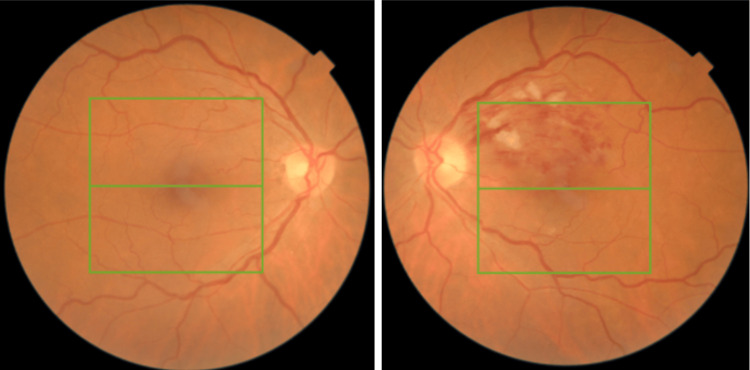 Figure 1
Figure 1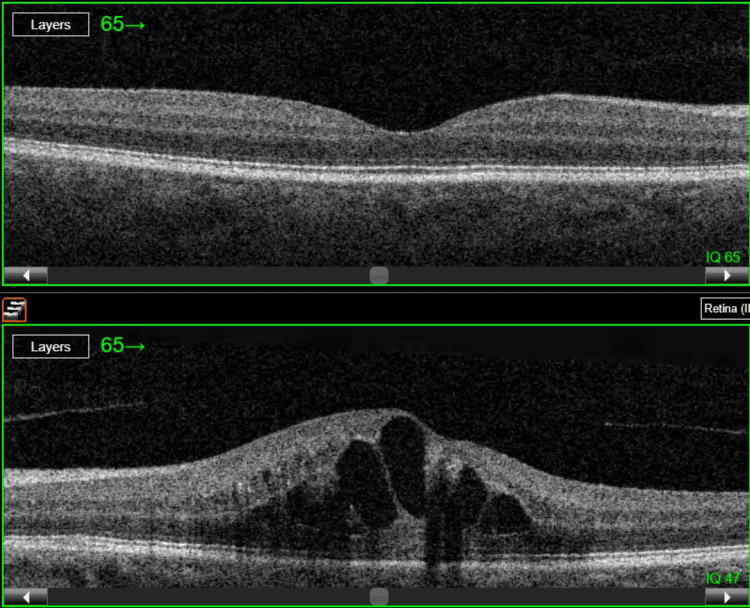 Figure 2
Figure 2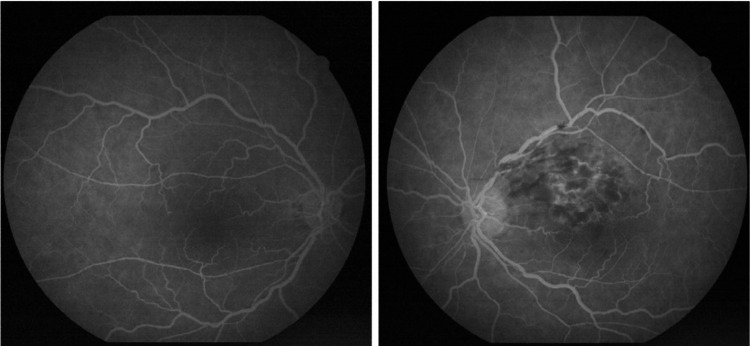 Figure 3
Figure 3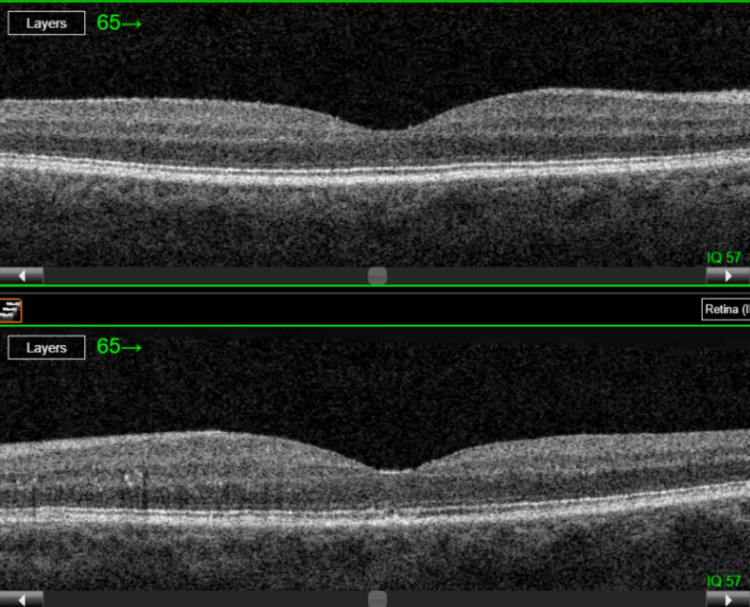 Figure 4
Figure 4| Parameter | Result |
| Blood pressure | 270/130 mmHg |
| Fasting blood glucose | Normal |
| HbA1c | Normal |
| Lipid profile | Normal |
| Complete blood count | Normal |
| Renal function/Electrolytes | Normal |
| Inflammatory markers | Normal |
| Timepoint | Treatment | BCVA (Snellen) | Central retinal thickness (µm) | Notes |
| Baseline | — | 20/40 | 638 | Cystoid macular edema |
| After 1st Injection | Anti-VEGF | 20/30 | 300 | Improvement in macular edema |
| After 2nd Injection | Anti-VEGF | 20/25 | 194 | Complete resolution of macular edema |
| Ongoing follow-up | Anti-VEGF | 20/25 | 194 | Monitoring continued |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRetinal and Optic Conditions · Retinal Diseases and Treatments · Retinal Imaging and Analysis
Introduction
Retinal vein occlusion (RVO) is one of the principal retinal vascular disorders, representing a significant cause of visual impairment [1]. It is estimated to affect approximately 16 million people worldwide. Among its subtypes, branch retinal vein occlusion (BRVO) occurs predominantly among all ethnic groups [2]. The arterio-venous crossing anatomy is a key element of BRVO pathogenesis. An anteriorly running arteriole compresses the underlying vein, contributing to occlusion. As a consequence, patients often notice a subtle blurring in a part of their visual field. BRVO typically presents with characteristic fundoscopic image, such as intraretinal hemorrhages, dilated and tortuous veins, cotton-wool spots, and macular edema [3]. The multifactorial nature of RVO has been reflected in a case-control study by Rath et al. (1992), which identified systemic hypertension, open-angle glaucoma, and male sex as major independent risk factors [4]. Arterial hypertension remains the strongest risk factor in both subtypes [5]. Notably, hypertension and diabetes-related end-organ damage promote vascular remodeling, atherosclerotic changes, and impaired endothelial function, all of which markedly predispose individuals to BRVO [6]. Given the multifactorial pathogenesis of this condition and its implications beyond the eye, it is crucial to emphasize the role of ophthalmologists in early diagnosis and timely referral for systemic evaluation. The present case report highlights the importance of comprehensive care in BRVO in unmasking a previously undiagnosed systemic disease.
Case presentation
Patient information
A 61-year-old woman presented to the ophthalmology outpatient department with a sudden, painless narrowing of the visual field in the left eye, which had developed the day before. She denied any other accompanying symptoms, including pain, flashes, or floaters, and reported no systemic symptoms suggestive of underlying disease. The patient had no significant past medical history and was not taking any regular medications. Family history was notable for myocardial infarction and ischemic stroke.
Ophthalmologic examination
On examination, her best-corrected visual acuity (BCVA) was 20/40 in the left eye, 20/30 in the right eye, and intraocular pressure was 15 mmHg bilaterally. The slit-lamp examination of the anterior segment was unremarkable in both eyes. Fundoscopic examination of the left eye revealed dilated, tortuous retinal veins, scattered retinal flame-shaped hemorrhages, retinal edema, and cotton wool spots, predominantly in the superior temporal quadrant. No abnormalities were observed in the right eye (Figure 1).
Fundus imaging of the right eye (left image) and the left eye (right image)The left eye demonstrates changes consistent with branch retinal vein occlusion.
Imaging findings
Optical coherence tomography (OCT) of the macula showed retinal elevation with cystoid macular edema with a central retinal thickness (CRT) of 638 µm in the left eye, while OCT of the right eye visualized well-preserved retinal architecture, with a CRT of 173 µm (Figure 2).
Optical coherence tomography (OCT) images of the right (top) and left (bottom) eyeThe scan of the left eye reveals cystoid macular edema associated with branch retinal vein occlusion.
Fluorescein angiography (FFA) confirmed non-ischemic BRVO in the superotemporal region, demonstrating delayed venous filling, venous leakage, and formation of collateral vessels. The retinal periphery showed no evidence of capillary non-perfusion or disturbed flow. The optic disc appeared normal (Figure 3).
Fluorescein angiography of the right eye (left image) and the left eye (right image), demonstrating findings consistent with a superior temporal branch retinal vein occlusion in the left eyeThe affected venous branch appears dilated and tortuous, with venous anastomoses temporal to the macula. In the area of occlusion, dot-blot and flame-shaped hemorrhages, cotton wool spots, and retinal edema extending towards the macula are observed. The peripheral retina shows no evidence of ischemic areas.
Treatment and systemic evaluation
Based on these findings, the patient was referred to a primary care physician for an evaluation of possible systemic causes of BRVO, and treatment with intraocular anti-VEGF injections was proposed. Anti-VEGF therapy was chosen to reduce macular edema and improve visual acuity, as recommended by current clinical guidelines [7,8]. Additionally, prior to the anti-VEGF injections, the patient was prescribed sulodexide to improve retinal microcirculation and reduce the risk of further vascular events. Although its direct effect on visual outcomes in BRVO is not clearly proven, and its use varies between clinicians, sulodexide was administered as an adjunct due to its vascular-protective properties [9].
One week after the initial ophthalmologic evaluation, the patient woke up with a severe headache and presented to the emergency department, where her blood pressure was found to be 270/130 mmHg (normal value: 120/80 mmHg). Laboratory tests, including complete blood count, lipid profile, metabolic panel and blood glucose were performed. All results were within normal limits, ruling out alternative systemic causes, such as uncontrolled diabetes, hypercoagulable states, and inflammatory conditions (Table 1).
The patient was diagnosed with primary arterial hypertension and, after blood pressure stabilization, was started on an antihypertensive therapy including a calcium channel blocker (amlodipine) and a thiazide diuretic (hydrochlorothiazide) under cardiology supervision.
Follow up
Subsequent ophthalmology follow-up, 20 days after the first presentation, showed improvement in visual acuity after the first anti-VEGF injection and stabilization after the second. Currently further treatment is ongoing, with the following results in the left eye: BCVA 20/25 and CRT of 194 µm (Figure 4 and Table 2).
Follow-up optical coherence tomography (OCT) scans of the right eye (top) and left eye (bottom), 20 days after two intravitreal anti-VEGF injections into the left eye, showing complete resolution of macular edema in the left eye
Discussion
In addition to being a retinal vascular disorder, BRVO often indicates an underlying systemic vascular malfunction, making it a major clinical issue in ophthalmology. Maintaining awareness of the close clinical correlation between BRVO and systemic vascular conditions is crucial for accurate evaluation and prevention of further complications.
Hyperlipidemia, arterial hypertension, diabetes mellitus, and hormonal variables are commonly associated with BRVO. The pathophysiological connection between BRVO and systemic hypertension extends beyond compression of the retinal vein by a sclerotic artery at the arteriovenous crossing. Subclinical processes, such as turbulent blood flow, decreased venous outflow, and endothelial damage, create conditions that favor the formation of a parietal thrombus, often making visual symptoms the first indication of systemic disease [10].
A recent systematic review of clinical practice guidelines for the diagnosis and management of retinal vein occlusion revealed inconsistencies regarding recommendations for systemic screening. The majority of the reviewed guidelines, scored low in methodological rigor, particularly when it came to protocols for cardiovascular screening and hypertension management. These results suggest that current guidelines may not provide sufficiently detailed approaches to systemic risk evaluation, emphasizing the need for a more multidisciplinary model of care for patients with BRVO [7].
In the present case, despite prompt referral for systemic assessment, the lack of standardized screening guidance and delayed follow-up led to a late recognition of the underlying hypertension. This marks the clinical importance of implementing standardized systemic assessment protocols in patients with retinal vascular occlusions. Establishing clear and time-bound pathways for cardiovascular assessment could facilitate earlier detection of hidden hypertension and reduce the risk of preventable ocular and systemic complications.
Other studies published in the literature have outlined retinal vascular occlusions as the first manifestation of systemic vascular disease. For example, Zhang et al. (2025) described a patient presenting with both BRVO and contralateral branch retinal artery occlusion (BRAO), who was found to have significant carotid atherosclerosis, suggesting a shared systemic pathology [11]. Considering the systemic vascular connections of BRVO, the local retinal pathology reflects the consequences of vascular compromise within the eye. A series of events, including disruption of the blood-retinal barrier, increased vascular permeability, and the development of macular edema are initiated. Moreover, sustained hypoxia promotes VEGF production, leading to neovascularization that may progress to vitreous hemorrhage or neovascular glaucoma if left untreated [12].
In this study, intravitreal anti-VEGF therapy significantly reduced macular edema and stabilized visual acuity, confirming the efficacy of this targeted treatment. Ocular complications, including macular edema, vitreous hemorrhage, and tractional retinal detachment, should be addressed promptly, with particular attention to resolving macular edema before irreversible damage occurs to the foveal photoreceptors, which are critical for central vision [13].
Given the association between retinal vein occlusions and potentially fatal events, a multidisciplinary approach is essential. Therefore, management should be integral not only for recognizing underlying systemic conditions such as hypertension, diabetes, dyslipidemia, or thrombophilic disorders but also for directing further ocular management. This shows that BRVO care should also be tailored to its underlying cause, since effective treatment requires addressing both ocular pathology and the systemic conditions that contribute to venous occlusion.
This case underscores the importance of standardized systemic screening after retinal vascular occlusions and shows how delayed diagnosis of hypertension might accelerate disease progression. It acts as an educational reminder of the need for organized cooperation between ophthalmologists and internal medicine caregivers.
Conclusions
BRVO represents a condition at the nexus of ophthalmology and internal medicine, where ocular findings may reveal hidden systemic disease. Prompt ocular care and systemic assessment may not only improve visual outcomes but also avert future cardiovascular complications. This case report illustrates how systemic hypertension may remain clinically silent until ocular vascular occlusion occurs, reinforcing the diagnostic relevance of retinal findings in the detection of systemic illness. The need for standardized systemic screening protocols and greater collaboration between ophthalmologists and internists to prevent irreversible vision loss and improve overall patient outcomes is strongly emphasized.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Retinal vein occlusion: beyond the acute event Surv Ophthalmol Ehlers JP Fekrat S 2812995620112160190310.1016/j.survophthal.2010.11.006 · doi ↗ · pubmed ↗
- 2The prevalence of retinal vein occlusion: pooled data from population studies from the United States, Europe, Asia, and Australia Ophthalmology Rogers S Mc Intosh RL Cheung N 31331911720102002211710.1016/j.ophtha.2009.07.017PMC 2945292 · doi ↗ · pubmed ↗
- 3Retinal vein occlusion Indian J Ophthal Hayreh SS 109132421994 https://journals.lww.com/ijo/fulltext/1994/42030/retinal_vein_occlusion.2.aspx 7829175 · pubmed ↗
- 4Risk factors for retinal vein occlusions. A case-control study Ophthalmology Rath EZ Frank RN Shin DH Kim C 509514991992158456710.1016/s 0161-6420(92)31940-2 · doi ↗ · pubmed ↗
- 5Global epidemiology of retinal vein occlusion: a systematic review and meta-analysis of prevalence, incidence, and risk factors J Glob Health Song P Xu Y Zha M Zhang Y Rudan I 104279201910.7189/jogh.09.010427 PMC 651350831131101 · doi ↗ · pubmed ↗
- 6Risk factors associated with developing branch retinal vein occlusion among enrollees in a United States managed care plan Ophthalmology Newman-Casey PA Stem M Talwar N Musch DC Besirli CG Stein JD 1939194812120142495379310.1016/j.ophtha.2014.04.045PMC 4177949 · doi ↗ · pubmed ↗
- 7Systematic review of clinical practice guidelines for the diagnosis and management of retinal vein occlusion Eye (Lond) Galvez-Olortegui J Bouchikh-El Jarroudi R Silva-Ocas I 172217333820243846786310.1038/s 41433-024-03008-1PMC 11156943 · doi ↗ · pubmed ↗
- 8Effectiveness and safety of anti-vascular endothelial growth factor therapies for macular edema in retinal vein occlusion: a systematic review and network meta-analysis of randomized controlled trials Surv Ophthalmol Chen KY Chan HC Chan CM 106710897020254041916610.1016/j.survophthal.2025.05.008 · doi ↗ · pubmed ↗