A Rare Case of Gastric Glomangioma Mimicking a Gastrointestinal Stromal Tumor (GIST)
Ahmet Yugruk, Altan Aydın, Orhan Semerci

TL;DR
A rare case of gastric glomangioma was mistaken for a gastrointestinal stromal tumor, highlighting the need for accurate diagnosis in similar cases.
Contribution
This paper reports a rare clinical case of gastric glomangioma misdiagnosed as a gastrointestinal stromal tumor.
Findings
A gastric glomangioma was surgically excised and confirmed histopathologically in a 61-year-old woman.
The lesion was initially misdiagnosed as a gastrointestinal stromal tumor due to overlapping imaging features.
Complete surgical removal resulted in an uneventful recovery with no complications during follow-up.
Abstract
Glomus tumors are rare mesenchymal neoplasms originating from modified smooth muscle cells involved in thermoregulation. Although typically located in peripheral soft tissues, their presence in the stomach is uncommon and may lead to diagnostic difficulties. This report presents a rare case of gastric glomangioma that clinically and radiologically mimicked a gastrointestinal stromal tumor. A 61-year-old woman presented in July 2024 with a three-month history of epigastric pain, nausea, and abdominal bloating. Upper gastrointestinal endoscopy revealed a submucosal lesion at the incisura angularis resembling a stromal tumor. Endoscopic ultrasonography demonstrated a well-circumscribed, submucosal, iso-hypoechoic mass measuring 19.5×11.3 mm. Due to persistent symptoms, surgical excision was performed, and the mass was completely removed with negative margins. Histopathological evaluation…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1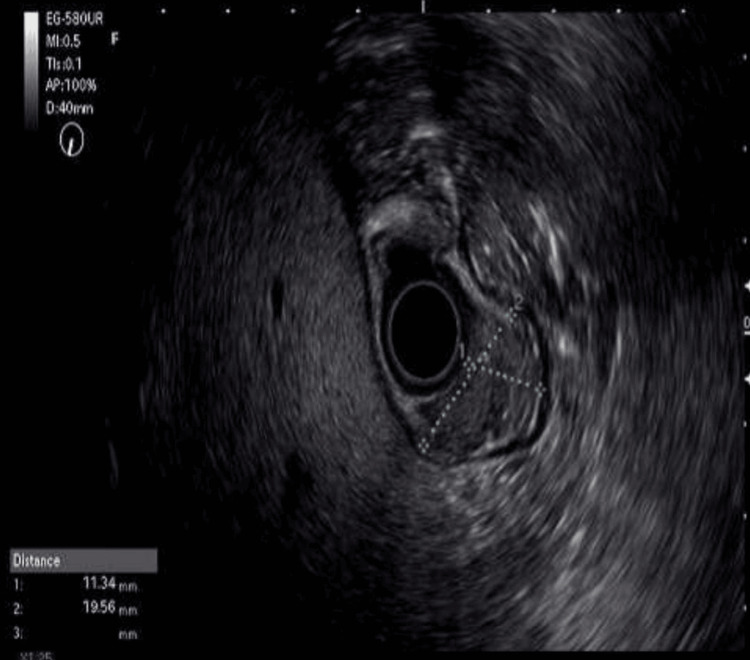 Figure 2
Figure 2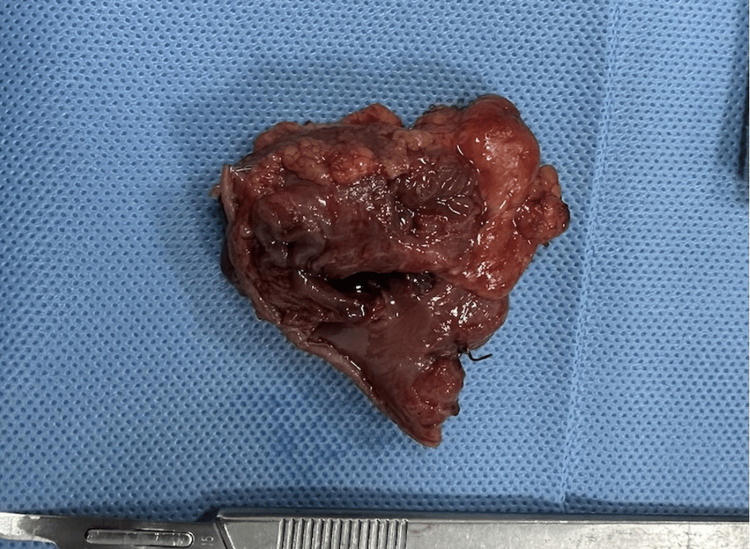 Figure 3
Figure 3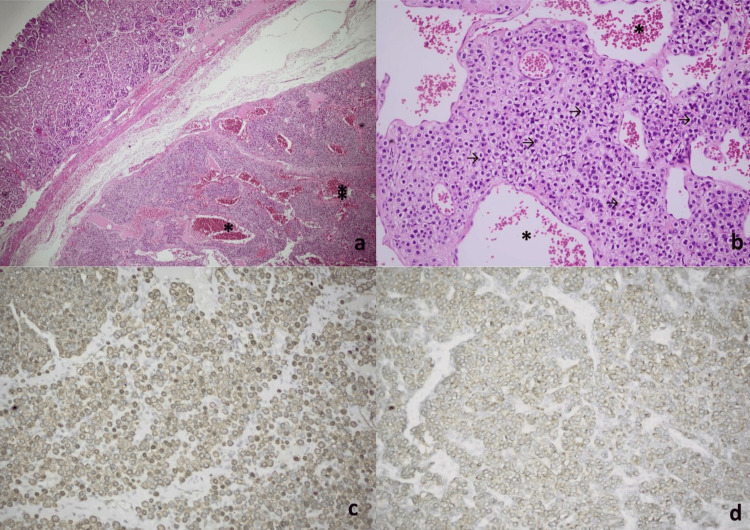 Figure 4
Figure 4| Parameters | Values | Normal range |
| Hemoglobin (g/dL) | 12.7 | 11-17 |
| White blood cells (x103/µL) | 10.2 | 3.9-10.9 |
| Platelets (x103/µL) | 216 | 100-380 |
| eGFR (mL/min) | 59 | >90 |
| Glucose (mg/dL) | 184 | 74-100 |
| Aspartate aminotransferase (IU/L) | 16 | <35 |
| Alanine aminotransferase (IU/L) | 22 | <35 |
| LDH (IU/L) | 162 | <248 |
| Amylase (IU/L) | 61 | 28-100 |
| Serum gastrin (pg/mL) | 520 | 13-115 |
| CA 19-9 (U/mL) | 85 | 0-37 |
| Markers | Results |
| CD117 | Very focal weak positive |
| DOG1 | Negative |
| CD34 | Focal positive |
| Ki-67 | 1% |
| S100 | Negative |
| SMA | Positive |
| Calponin | Positive |
| Caldesmon | Positive |
| Collagen type IV | Positive |
| Synaptophysin | Positive |
| Chromogranin | Negative |
| Desmin | Negative |
| PanCK | Negative |
| CD45 | Negative |
| CD31 | Negative |
| INSM1 | Negative |
| CD56 | Focal positive |
| CAM 5.2 | Negative |
| SSTR2 | Positive |
| GATA3 | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSoft tissue tumors and treatment · Soft tissue tumor case studies · Teratomas and Epidermoid Cysts
Introduction
Glomus tumors are rare mesenchymal neoplasms arising from glomus bodies, which are specialized arteriovenous anastomoses involved in thermoregulation [1]. Although they are typically found in peripheral soft tissues, including the subungual regions, their occurrence in visceral organs, particularly within the gastrointestinal tract, is extremely rare. To date, fewer than 200 cases of gastric glomus tumors have been reported in the literature, underscoring their exceptional rarity. They account for approximately 1% of all glomus tumors and are most commonly located in the antrum [2,3]. Clinically, these tumors may present with nonspecific symptoms, such as epigastric pain, dyspepsia, nausea, vomiting, and upper gastrointestinal bleeding. Due to their submucosal localization and overlapping imaging characteristics, these tumors are frequently misdiagnosed as the more common gastrointestinal stromal tumors (GISTs) [4]. Distinguishing between these entities is crucial, as their management and prognosis differ significantly. Immunohistochemical profiling plays a pivotal role in diagnosis, as glomus tumors typically show positivity for smooth muscle actin (SMA) and negativity for cluster of differentiation 117 (CD117) and discovered on GIST-1 (DOG1) [5]. Complete surgical resection with negative margins remains the mainstay of treatment and serves both diagnostic and curative purposes. This study contributes to the limited literature on gastric glomangiomas and highlights the importance of considering these rare tumors in the differential diagnosis of subepithelial gastric lesions.
Case presentation
A 61-year-old woman with class III obesity (body mass index: 43 kg/m², WHO classification) presented in July 2024 with a three-month history of persistent epigastric pain, nausea, and bloating. Her past medical history included type 2 diabetes mellitus, hypertension, hypercholesterolemia, and stage 2 chronic kidney disease secondary to diabetic nephropathy. On physical examination, no pathological findings were observed other than obesity. Initial laboratory evaluation revealed elevated serum gastrin and increased cancer antigen 19-9 (CA 19-9) levels, while renal function was decreased, consistent with her chronic kidney disease (Table 1).
Upper gastrointestinal endoscopy demonstrated a 2 cm subepithelial lesion at the incisura angularis with intact overlying mucosa (Figure 1). Endoscopic ultrasonography revealed a well-circumscribed, iso-hypoechoic mass (19.5×11.3 mm) confined to the submucosa without invasion of the muscularis propria, with minimal cystic changes and poor vascularity (Figure 2). Abdominal computed tomography showed no evidence of metastatic disease.
Endoscopic view of gastric glomangioma.
Endoscopic ultrasonography view of gastric glomangioma.
Given the persistence of symptoms and diagnostic uncertainty, exploratory laparotomy with wedge resection of the gastric lesion was performed. The resected specimen measured 3×3 cm and contained a well-defined 1.5×0.6 cm nodule, located 1 cm from the stapled margin, 0.2 cm from the mucosal margin, and 0.1 cm from the serosal surface (Figure 3).
Surgical specimen material.
Histopathological examination revealed a well-circumscribed submucosal lesion composed of round glomus cells arranged around dilated, erythrocyte-filled vascular channels, resembling cavernous hemangioma-like structures. The tumor showed monotonous architecture with amphophilic to lightly eosinophilic cytoplasm and vesicular chromatin (Figures 4a-4d). Immunohistochemistry demonstrated positivity for smooth muscle actin (SMA), vimentin, and calponin, with negativity for cluster of differentiation 117 (CD117), Discovered on GIST-1 (DOG1), desmin, and S-100 (Table 2, Figures 4a-4d).
Histopathological and immunohistochemical features of gastric glomangioma.(a) Hematoxylin and eosin (H&E, ×40): a submucosal proliferative tumor lesion composed of small clusters of glomus cells surrounding dilated, erythrocyte-filled vessels (), resembling cavernous hemangioma-like structures. (b) H&E (×100): the tumor consists of uniform, small, round glomus cells with monotonous round nuclei, vesicular chromatin, and amphophilic to lightly eosinophilic cytoplasm. These cells exhibited sharply defined borders (→) and were arranged in clusters surrounding dilated vascular structures (). (c) Smooth muscle actin {SMA} immunohistochemistry {IHC} (×100): diffuse SMA positivity, consistent with glomus tumor phenotype. (d) Synaptophysin IHC (×100): strong synaptophysin expression, a potential diagnostic pitfall mimicking neuroendocrine tumors.
The final diagnosis of gastric glomangioma was established based on the combined histomorphology and immunohistochemical findings. The postoperative course was uneventful, and the patient was discharged on postoperative day five with regular follow-up. Clinical examinations were performed at one, three, six, nine, and 12 months, while abdominal CT imaging was obtained at six and 12 months of follow-up. At both six and 12 months, the patient remained symptom-free with no clinical or radiological evidence of recurrence.
Discussion
Intramural mesenchymal tumors of the stomach include GISTs, various sarcomas, lipomas, leiomyomas, schwannomas, glomus tumors, hemangiomas, inflammatory fibroid polyps, inflammatory myofibroblastic tumors, and plexiform fibromyxomas. Among these, glomus tumors of the gastrointestinal tract (GIT) are rare, accounting for approximately 1% of GIT soft tissue tumors [2]. GISTs are the most common soft tissue tumors of the stomach [4]. Gastric glomus tumors are approximately 100 times less common than GISTs [6]. Gastric glomus tumors predominantly affect women between the ages of 50 and 60 years and typically present as solitary submucosal lesions localized in the antrum [5]. Symptoms are generally nonspecific and may include epigastric pain, bleeding, nausea, and vomiting.
Preoperative differentiation between glomus tumors and GIST remains challenging due to overlapping endoscopic and imaging findings, their deep submucosal location, and the lack of distinctive findings on CT scans [7,8]. Consequently, many gastric glomus tumors are identified incidentally during surgical intervention for presumed GISTs [2]. Immunohistochemical staining is essential for accurate diagnosis. Glomus tumors typically show strong SMA positivity and are negative for CD117 and DOG1, although rare cases may demonstrate focal or weak, non-specific CD117 staining that is not indicative of GIST. In our case, CD117 showed very focal weak positivity, consistent with this known but uncommon finding. DOG1 staining is increasingly recognized as a specific marker for diagnosing GIST [5]. Yoshida et al. reported that synaptophysin expression in gastric glomus tumors poses a significant diagnostic challenge, as evidenced by their report of a glomus tumor initially misdiagnosed as a neuroendocrine neoplasm due to strong synaptophysin immunoreactivity [3]. This paradoxical positivity, observed in 30-40% of cases according to Wang et al, requires careful interpretation alongside negative chromogranin and insulinoma-associated protein 1 results, to prevent misclassification [5]. The synaptophysin/chromogranin profile observed in this case is consistent with the findings of Vassiliou et al., highlighting that glomus tumors should be included in the differential diagnosis of synaptophysin-positive gastric submucosal lesions despite their non-neuroendocrine origin [7].
Although most gastric glomus tumors are benign, lesions exceeding 5 cm may raise concern for malignant potential [9]. The preferred treatment is complete surgical resection with negative margins, followed by long-term postoperative surveillance to monitor for recurrence [2].
Conclusions
Gastric glomangioma, a vascular variant of glomus tumor, is a rare but clinically important neoplasm that can closely mimic more common subepithelial gastric tumors, particularly GIST. Accurate diagnosis depends primarily on histopathological and immunohistochemical examinations, as imaging findings are often nonspecific. This case highlights the importance of considering glomus tumors in the differential diagnosis of gastric lesions, especially when typical GIST immunomarkers are absent. Complete surgical resection with negative margins remains the treatment of choice, and long-term follow-up is recommended due to a low but possible risk of recurrence. Increasing awareness and reporting of such cases can enhance diagnostic accuracy and optimize patient management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gastric glomus tumor J Surg Case Rep Jain SA Agarwal L Goyal A Kumar R Nadkarni S Ameta A Rao YS 2014201410.1093/jscr/rju 049PMC 407134124968870 · doi ↗ · pubmed ↗
- 2Laparoscopic antral resection with Billroth I reconstruction for a gastric glomus tumor Int J Surg Case Rep Halawani HM Khalife M Safadi B Rida K Boulos F Khalifeh F 11281131520142543765510.1016/j.ijscr.2014.10.009PMC 4276278 · doi ↗ · pubmed ↗
- 3Gastrointestinal: glomus tumor: a rare submucosal tumor of the stomach J Gastroenterol Hepatol Yoshida H Asada M Marusawa H 34201910.1111/jgh.1459430665269 · doi ↗ · pubmed ↗
- 4Gastrointestinal stromal tumors: the incidence, prevalence, clinical course, and prognostication in the preimatinib mesylate era - a population-based study in western Sweden Cancer Nilsson B Bümming P Meis-Kindblom JM 82182910320051564808310.1002/cncr.20862 · doi ↗ · pubmed ↗
- 5Features of gastric glomus tumor: a clinicopathologic, immunohistochemical and molecular retrospective study Int J Clin Exp Pathol Wang ZB Yuan J Shi HY 1438144872014 https://pubmed.ncbi.nlm.nih.gov/24817939/24817939 PMC 4014223 · pubmed ↗
- 6Small submucosal tumors of the stomach: differentiation of gastric schwannoma from gastrointestinal stromal tumor with CT Korean J Radiol Choi JW Choi D Kim KM Sohn TS Lee JH Kim HJ Lee SJ 4254331320122277856410.3348/kjr.2012.13.4.425PMC 3384824 · doi ↗ · pubmed ↗
- 7Gastric glomus tumor: a case report World J Surg Oncol Vassiliou I Tympa A Theodosopoulos T Dafnios N Fragulidis G Koureas A Kairi E 8201010.1186/1477-7819-8-19PMC 285658220307271 · doi ↗ · pubmed ↗
- 8Glomus tumor of the stomach: a rare cause of upper gastrointestinal bleeding Case Rep Surg Nascimento EF Fonte FP Mendonça RL Nonose R de Souza CA Martinez CA 2011201110.1155/2011/371082 PMC 335005522606576 · doi ↗ · pubmed ↗