Long-Term Outcome of Myocardial Protection in Heart Transplantation: Comparison Among 3 Different Solutions
Fabrizio Settepani, Aldo Cannata, Igor Belluschi, Giulia Pinuccia Pisani, Michele Giovanni Mondino, Andrea Garascia, Claudio Francesco Russo

TL;DR
This study compares the long-term outcomes of three different cardioplegic solutions used in heart transplants and finds that one solution is linked to higher graft dysfunction but similar survival rates.
Contribution
The study provides new long-term comparative data on cardioplegic solutions in heart transplantation.
Findings
HTK-Custodiol was associated with higher primary graft dysfunction compared to Celsior.
In-hospital mortality and long-term survival were similar across all three groups.
Post-transplant rejection rates were comparable among the three cardioplegic solutions.
Abstract
We analysed our long-term experience with heart transplantation (Htx) utilizing 3 different cardioplegic solutions. During a 20-year period, 538 adult individuals underwent isolated Htx at our institution. Ten cases in which the Organ Care System TransMedics Inc was utilized were excluded, resulting in a final cohort of 528 individuals. Patients were stratified into 3 groups according to the donor heart cardioplegic solution: Celsior (n = 301; reference group), HTK-Custodiol (n = 88), and St Thomas (n = 139). Mean follow-up period was 6.2 ± 5.5 years (maximum 20 years). The rate of severe primary graft dysfunction (PGD) was 10.2% in the HTK-Custodiol group, significantly higher than the reference group (4.5%; P < .040). Overall, in-hospital mortality was 12.9%: 13.6% in the HTK-Custodiol group and 12.9% in the St Thomas group, comparable to the reference group (P = .803 and P = .924).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
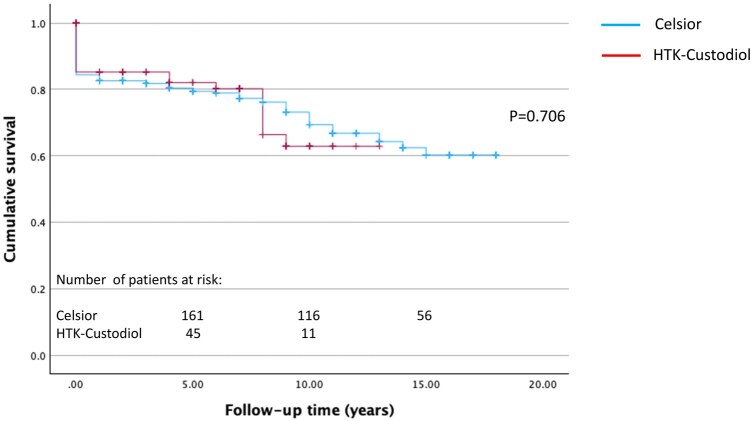 Figure 1
Figure 1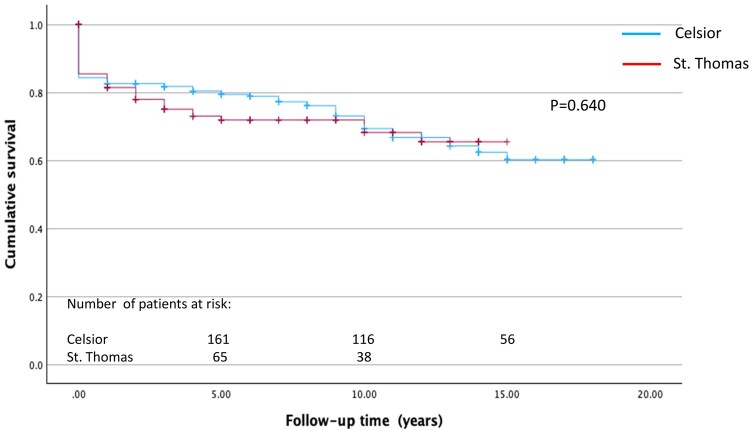 Figure 2
Figure 2| Variables | Celsior ( | HTK-Custodiol ( |
| St. Thomas ( |
|
|---|---|---|---|---|---|
| Age (years) | 49.4 (±11.2) | 49.3 (±11.3) | .921 | 48.6 (±11.4) | .476 |
| Gender, female | 88 (29.2%) | 32 (36.4%) | .203 | 45 (32.4%) | .505 |
| BMI (kg/m2) | 23.1 (±3,8) | 23.6 (±3,3) | .193 | 23.3 (±3,4) | .518 |
| PVRI (Woods units) | 4.2 (±2,6) | 4.5 (±2,4) | .323 | 4.1 (±2,4) | .847 |
| Aetiology of heart failure | |||||
| Dilated cardiomyopathy | 113 (37.5%) | 37 (42%) | .445 | 52 (37.4%) | .979 |
| Hypertrophic cardiomyopathy | 16 (5.3%) | 6 (6.8%) | .591 | 8 (5.8%) | .850 |
| Ischaemic aetiology | 93 (31%) | 19 (21.6%) | .087 | 38 (27.3%) | .435 |
| Valvular aetiology | 14 (4.7%) | 3 (3.4%) | .612 | 2 (1.4%) | .093 |
| Congenital heart disease | 9 (3%) | 3 (3.4%) | .841 | 4 (2.9%) | 1.0 |
| CAV | 7 (2.3%) | 1 (1.1%) | .489 | 5 (3.6%) | .531 |
| Restrictive cardiomyopathy | 5 (1.7%) | 3 (3.4%) | .309 | 3 (2.2%) | .712 |
| VAD complications | 9 (3%) | 2 (2.3%) | .721 | 6 (4.3%) | .537 |
| Emergency transplant | 58 (19.3%) | 19 (21.8%) | .597 | 33 (23.7 %) | .282 |
| L-VAD | 43 (14.5%) | 8 (9.1%) | .187 | 26 (18.7%) | .266 |
| ECMO | 19 (6.4%) | 9 (10.2%) | .228 | 17 (12.2%) |
|
| Impella | 4 (1.4%) | 0 | .578 | 1 (0.7%) | .564 |
| IABP | 35 (11.8%) | 13 (14.8%) | .463 | 16 (11.5 %) | .924 |
| Ventilator support | 25 (8.4%) | 15 (17%) |
| 12 (8.6%) | .948 |
| Prior cardiac surgery | 84 (27.9%) | 21 (23.9%) | .452 | 41 (29.5%) | .731 |
| Diabetes | 33 (11.3%) | 13 (14.8%) | .376 | 12 (8.7 %) | .416 |
| Chronic renal failure | 69 (23.5%) | 24 (27.6%) | .432 | 33 (24.1%) | .882 |
| Acute renal failure | 28 (9.5%) | 8 (9.2%) | .927 | 7 (5.1%) | .118 |
| Dialysis | 2 (0.7%) | 0 (0%) | .441 | 2 (1.5%) | .432 |
| CVVH | 45(1.7%) | 3 (3.4%) | .313 | 4 (2.9%) | .412 |
| Serology | |||||
| HCV | 14 (4.7%) | 3 (3.4%) | .752 | 3 (2.2%) | .203 |
| HIV | 0 | 0 | 1.0 | 1 (0.7 %) | 1.0 |
| Creatinine at transplant (mg/dL) | 1.21 (±0.54) | 1.19 (±0.4) | .737 | 1.22 (±1) | .956 |
| Bilirubin at transplant (mg/dL) | 1.15 (±1.12) | 1.96 (±7.33) | .322 | 1.83 (±6) | .209 |
| Variables | Celsior ( | HTK-Custodiol ( |
| St. Thomas ( |
|
|---|---|---|---|---|---|
| Age (years) | 41.5 (±13.8) | 44.2 (±12.7) | .086 | 43.3 (±13.1) | .190 |
| Gender female | 105 (35%) | 34 (39.1%) | .482 | 49 (35.5%) | .911 |
| BMI (kg/m2) | 25 (±3.9) | 25.4 (±2.1) | .446 | 25.4 (±3.5) | .488 |
| Cause of death | |||||
| Head trauma | 45 (15.1%) | 8 (9.2%) | .163 | 22 (16.6%) | .763 |
| SAH | 134 (44.8%) | 43 (49.4%) | .448 | 59 (43.4%) | .780 |
| Polytrauma | 64 (21.4%) | 25 (28.7%) | .153 | 27 (19.9%) | .712 |
| Comorbidities | |||||
| Hypertension | 61 (22.9%) | 21 (25%) | .696 | 23 (18.7%) | .345 |
| Diabetes | 2 (0.8%) | 2 (2.4%) | .244 | 1 (0.8%) | 1.0 |
| Obesity (BMI >30) | 5 (1.9%) | 3 (3.6%) | .404 | 2 (1.6) | 1.0 |
| Cocaine abuse | 7 (2.6%) | 5 (5.9%) | .171 | 9 (7%) | .055 |
| Smoke history | 53 (19.9%) | 27 (32.1%) |
| 34 (27.4%) | .098 |
| Inotropic support | |||||
| LD | 136 (47.9%) | 35 (42.2%) | .358 | 50 (39.1%) | .109 |
| MD | 80 (28.2%) | 18 (21.7%) | .240 | 34 (26.6%) | .736 |
| HD | 24 (8.5%) | 9 (10.8%) | .503 | 13 (10.2%) | .575 |
| Serology | |||||
| Toxoplasmosis | 7 (2.5%) | 7 (8.3%) |
| 8 (6.3%) | .084 |
| CMV | 17 (5.9%) | 13 (15.3%) |
| 17 (13.3%) |
|
| HCV | 3 (1%) | 2 (2.4%) | .320 | 1 (0.8%) | 1.0 |
| Severe hypotension/cardiac arrest | 74 (27%) | 29 (33.7%) | .229 | 37 (30.3%) | .497 |
| Cardiac arrest time (min) | 3.3 (±1.19) | 2.4 (±2.1) | .411 | 2.1 (1.6) | .216 |
| Positive blood culture | 4 (1.6%) | 4 (5.2%) | .089 | 3 (2.1) | .137 |
| Blood transfusion | 133 (59.1%) | 49 (64.5%) | .402 | 65 (58.6%) | .921 |
| ICU time (days) | 3.40 (±3.6) | 3 (±3.1) | .368 | 3.7 (±3.4) | .489 |
| CPK total (U/L) | 509 (±80) | 411 (±45) | .155 | 430 (±62) | .395 |
| CPK-MB (U/L) | 21 (±5) | 15 (±3) | .723 | 31 (±3) | .633 |
| Serum Na+ (mEq/L) | 147 (±12) | 149 (±9) | .335 | 148 (±9) | .439 |
| Serum K+(mEq/L) | 4 (±2.7) | 3.8 (±0.5) | .193 | 3.9 (±0.6) | .407 |
| Central venous pressure (mmHg) | 7 (±3) | 8 (±3) | .528 | 8 (±3) | .335 |
| Variables | Celsior ( | HTK-Custodiol ( |
| St. Thomas ( |
|
|---|---|---|---|---|---|
| Female donor/male recipient sex mismatch | 38 (12.6%) | 9 (10.2%) | .544 | 19 (13.7%) | .763 |
| Donor/recipient ratio BMI | 1.106 (±0.225) | 1.096 (±0.23) | .620 | 1.11 (±0.235) | .887 |
| Donor-recipient pHM undersize >15% | 28 (9.5%) | 5 (5.9%) | .303 | 9 (6.7%) | .344 |
| CPB time (min) | 208 (±78) | 224 (±80) | .114 | 212 (±63) | .623 |
| Total ischaemic time (min) | 185 (±53) | 180 (±50) | .459 | 186 (±51) | .822 |
| ICU LOS (days) | 12.3 (±3.8) | 11.7 (±1.4) | .849 | 10.8 (±1.2) | .556 |
| Transfusion requirements (units) | |||||
| RBC | 3.9 (±0.6) | 5.1 (±0.8) | .175 | 5 (±0.8) | .164 |
| Platelets | 0.6 (±0.1) | 0.6 (±0.3) | .899 | 0.5 (±0.2) | .498 |
| FFP | 2.1 (±0.4) | 3.1 (±0.8) | .322 | 2 (±0.3) | .787 |
| ECMO | 13 (4.5%) | 9 (10.2%) |
| 5 (3.6%) | .679 |
| IABP | 41 (13.4%) | 26 (29.5%) |
| 29 (21.2%) | .074 |
| Primary graft dysfunction (severe) | 13 (4.5%) | 9 (10.2%) |
| 5 (3.6%) | .696 |
| CVVH | 46 (15.7%) | 19 (21.6%) | .198 | 23 (18.6%) | .774 |
| Chronic renal failure (new onset, including dialysis) | 23 (7.8%) | 3 (3.8%) | .215 | 12 (9.4%) | .588 |
| Dialysis (excluding pre-operative) | 5 (1.7%) | 0 (0%) | .589 | 0 (0%) | .320 |
| TND | 22 (7.6%) | 6 (6.9%) | .817 | 11 (8.1%) | .872 |
| PND | 7 (2.4%) | 3 (3.4%) | .704 | 4 (2.9%) | .762 |
| Sternal wound infection | 9 (3.1%) | 1 (1.1%) | .464 | 2 (1.5%) | .308 |
| UTIs | 5 (1.7%) | 2 (2.3%) | .74 | 3 (2.2%) | .755 |
| Pneumonia | 48(16.6%) | 15 (17.2%) | .922 | 25 (18.4%) | .685 |
| Tracheostomy | 15 (5.2%) | 3 (3.4%) | .775 | 8 (5.9%) | .819 |
| In-hospital mortality | 38 (12.6%) | 12 (13.6%) | .803 | 18 (12.9%) | .924 |
| Variables | Celsior ( | HTK-Custodiol ( |
| St. Thomas ( |
|
|---|---|---|---|---|---|
| Cellular rejection | 142 (48.8%) | 48 (57.8%) | .139 | 67 (50.4%) | .572 |
| Humoral rejection | 15 (5.2%) | 3 (3.6%) | .533 | 9 (6.8%) | .493 |
| Univariate analysis | Multivariable analysis | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI |
| HR | 95% CI |
| |
| Recipient factors | ||||||
| Age (years) | 1.047 | 1.024-1.069 |
| 1.027 | 1.009-1.046 |
|
| Sex female | 1.558 | 1.117-2.175 |
| |||
| BMI (kg/m2) | 1.011 | 0.957-1.069 | .685 | |||
| Aetiology of heart failure | ||||||
| Dilated cardiomyopathy | 1.252 | 0.814-1.925 | .306 | |||
| Hypertrophic cardiomyopathy | 0.489 | 0.162-1.474 | .195 | |||
| Ischaemic aetiology | 1.594 | 1.018-2.496 |
| |||
| Valvular aetiology | 1.140 | 0.337-3.860 | .762 | |||
| Congenital heart disease | 1.140 | 0.337-3.860 | .762 | |||
| CAV | 1.140 | 0.337-3.860 | .762 | |||
| Restrictive cardiomyopathy | 0.374 | 0.045-3.137 | .681 | |||
| VAD complications | 0.168 | 0.022-1.299 | .073 | |||
| Emergency transplant | 0.455 | 0.256-0.810 |
| |||
| Pre-operative L-VAD | 1.136 | 0.649-1.989 | .655 | |||
| Pre-operative ECMO | 0.771 | 0.350-1.697 | .517 | |||
| Pre-operative Impella | 6.907 | 0.717-67.651 | .087 | |||
| Pre-operative IABP | 0.625 | 0.308-1.268 | .190 | |||
| Pre-operative ventilator support | 1.096 | 0.517-2.325 | .811 | |||
| Prior cardiac surgery | 1,243 | 0.787-1.963 | .351 | |||
| Diabetes | 1.048 | 0.510-2.152 | .899 | |||
| Chronic renal failure | 1.994 | 1.238-3.211 |
| 1.518 | 1.059-2.177 |
|
| Acute renal failure | 0.907 | 0.405-2.031 | .813 | |||
| Dialysis | 4.525 | 0.406-50.371 | .227 | |||
| CVVH | 1.116 | 0.274-4.538 | 1.0 | |||
| Donor factors | ||||||
| Age (years) | 1.019 | 1.003-1.035 |
| 1.015 | 1.001-1.030 |
|
| Gender female | 1.152 | 0.856-1.552 | .342 | |||
| BMI (kg/m2) | 1.025 | 0.970-1.083 | .381 | |||
| Cause of death | ||||||
| Head trauma | 1.206 | 0.706-2.242 | .433 | |||
| SAH | 0.858 | 0.559-1.315 | .481 | |||
| Polytrauma | 0.926 | 0.549-1.563 | .773 | |||
| Comorbidities | ||||||
| Hypertension | 1.008 | 0.594-1.711 | .977 | |||
| Diabetes | 1.084 | 0.097-12.079 | 1.0 | |||
| Obesity (BMI >30) | 0.428 | 0.049-3.709 | .699 | |||
| Cocaine abuse | 1.985 | 0.702-6.612 | .253 | |||
| Smoke history | 0.908 | 0.525-1.570 | .730 | |||
| Inotropic support HD | 1.169 | 0.561-2.435 | .676 | |||
| Severe hypotension/cardiac arrest | 1.090 | 0.673-1.765 | .725 | |||
| Cardiac arrest time (min) | 1.008 | 0.987-1.029 | .470 | |||
| Cardioplegic solution | ||||||
| Celsior | 1.102 | 0.704-1.727 | .671 | |||
| HTK-Custodiol | 1.008 | 0.992-1.024 | .306 | |||
| St. Thomas | 0.931 | 0.592-1.464 | .758 | |||
| Transplant data | ||||||
| Total ischaemic time | 1.005 | 1.001-1.009 |
| 1.004 | 1.001-1.007 |
|
| Severe PGD | 3.087 | 1.407-6.772 |
| 3.253 | 1.805-5.863 |
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTransplantation: Methods and Outcomes · Cardiac Ischemia and Reperfusion · Mechanical Circulatory Support Devices
INTRODUCTION
Heart transplantation (HTx) has become the preferred option for select end-stage heart failure patients.1 Effective graft preservation, typically achieved through diastolic arrest and static cold ischaemia with a 4-6 h limit, is crucial.2 Despite various preservation solutions, an optimal standard remains elusive.3 This article reports our single-center, 20-year experience with 3 different cardiac preservation solutions (Celsior, HTK-Custodiol and St Thomas) in HTx.
METHODS
Study design and patient population
This was an observational study, utilizing a prospectively maintained institutional database of all consecutive Htx at the Niguarda Hospital, Milan. The study was approved by the Institutional Ethic Board at Niguarda Hospital Milan (ERB approval number: 215-29042020; May 5, 2020) and individual consent was waived. The collection and use of identifiable data and biological materials prioritize individual rights, informed consent, privacy, and robust governance in accordance with the The WMA Declaration of Taipe. The ethics committee has approved the establishment and monitored ongoing use of such databases and biobanks.
From January 2002 to December 2022, 538 adult patients were consecutively submitted to isolated Htx at our institution. This period was selected because the operative technique and immunosuppressive treatment were comparable in the entire cohort. To minimize the effect of variables that could interfere with the results, 10 cases in which the Organ Care System TransMedics Inc was utilized were excluded from the study, resulting in a final cohort of 528 individuals. Patients were stratified into 3 groups according to the donor heart cardioplegic solution: Celsior (n = 301; reference group), HTK-Custodiol (n = 88), and St Thomas (n = 139). The perioperative variables and postoperative outcomes were retrospectively reviewed. The primary end-points were recipient severe PGD, survival, and post-transplant rejection.
Operative technique
Grafts were harvested from beating-heart brain-dead donors. Our clinical protocols for preservation solutions were previously reported in details.4 Briefly, for donor heart preservation, we adopted 3 types of solutions: extracellular Celsior (Genzyme Corp., Boston, MA, United States), intracellular HTK-Bretschneider (Custodiol, Dr Franz Cohler Chemie GMBT, Bensheim, Germany), and extracellular St Thomas No. 2 (Plegisol, Hospira, Inc, United States). The choice of the solution was left to the surgeon’s discretion. Upon implantation, antegrade cold (4°C) 4:1 blood cardioplegia was administered every 20 min to hearts preserved by means of Celsior and St Thomas solutions. In accordance with the Custodiol cardioplegia administration protocol, that enables up to 3 h of safe cardioplegic arrest, no further cardioplegia was administered during implantation to hearts preserved by means this solution, unless total ischaemic time exceeded 180 min: in that case, half dose of Custodiol was re-administered.3^,^5^,^6 Orthotopic transplantation was invariably performed with standard left atrial cuff technique. Our approach to the primary graft dysfunction (PGD) has been previously described.7 Briefly: a pulmonary artery catheter was inserted after the transplantation. If this was not possible, PGD was diagnosed using echocardiographic parameters as per Kobashigawa et al.8 Accordingly, severe PGD was diagnosed as dependence on left or biventricular mechanical support, after excluding a discernible cause such as hyper-acute rejection, pulmonary hypertension, or known surgical complications (eg, uncontrolled bleeding). With regards to haemodynamic parameters, severe haemodynamic compromise lasting >1 hour manifested as hypotension (systolic blood pressure <90 mmHg), low cardiac output (cardiac index <2.0 L/min/m^2^), high filling pressures (right atrial pressure (RAP) >15 mmHg and pulmonary capillary wedge pressure >20 mmH), requiring ≥2 intravenous inotropic/vasopressor drugs, including high-dose norepinephrine (>0.7 μg/kg/min) or high-dose epinephrine (>0.07 μg/kg/min), indicate PGD. To support the diagnosis, an echocardiographic assessment of the left and right ventricle must be performed: in details, a low left ventricle ejection fraction (40% or less), a reduction of the tricuspid annular plane systolic excursion (13 mm or less) and RV free wall strain (−14% or less), are key indicators of PGD.
Statistical analysis
Baseline clinical and procedural characteristics as well as clinical outcomes were compared between the groups. Continuous variables were expressed as the mean ± SD and were analysed by using the Welch t-test. Categorical variables were presented as percentage and were analysed with the X^2^ test or Fischer exact test when appropriate. Estimates for long-term survival were made by the Kaplan-Meier method. Differences between survival curves were evaluated with the log-rank statistic. Cox proportional hazard model was used to analyse the relationship between survival probability and treatment. Univariate and multivariable analysis of risk factors for late mortality was performed. For the univariate analysis several pre-operative and intraoperative variables were considered. Variables that achieved a P-value less than .2 in the univariate analysis were examined by using Cox proportional hazard regression. Statistical analysis was performed using SPSS version 29 (SPSS, Inc., Chicago, IL, United States).
RESULTS
Comparison among the groups
Pre-operative recipient and donor characteristics with statistical comparison of the 3 groups are displayed in Tables 1 and 2, respectively. The groups were similar for most of the variables considered. However, when compared to the reference group, patients in the St Thomas group had a significantly higher rate of pre-operative extra-corporeal membrane oxygenation (ECMO) (12.2% vs 6.4%, P = .040), whereas, patients in the HTK-Custodiol group had a higher rate of pre-operative ventilatory support (17% vs 8.4%, P = .020). With respect to the donor characteristics, no significant differences were observed among the groups for most of the variables, but smoke history, serology positive for toxoplasmosis, and cytomegalovirus were more common in the HTK-Custodiol group.
Intraoperative data as well as postoperative outcomes for each group are summarized in Table 3.
There were no significant differences among the groups regarding intraoperative variables including total ischaemic time.
With regards to postoperative outcomes, patients in the HTK-Custodiol group had a higher rate of ECMO (10.2% vs 4.5%, P = .046) and intra-aortic balloon pump (IABP) (29.5% vs 13.4%., P = .001).
Primary graft dysfunction
Patients in the HTK-Custodiol group had a higher rate of severe primary graft dysfunction (10.2% vs 4.5%, P = .040). Instead, the rate of severe PGD in the St Thomas group was found to be comparable to the reference group (3.6% vs 4.5%, P = .696). The mean values of the main haemodynamic and echocardiographic parameters at the time of severe PGD diagnosis were: systolic blood pressure = 74 (±6) mmHg, cardiac index = 1.3 (±0.3) L/min/m^2^, pulmonary capillary wedge pressure = 28 (±7) mmHg, left ventricle ejection fraction = 22 (±5)%, RV free wall strain = −11 (±3)%.
** Table 3 ** displays in details intraoperative and postoperative in-hospital outcomes.
Survival analysis
Overall, in-hospital mortality was 12.9%; 13.6% in the in HTK-Custodiol group and 12.9% in the St Thomas group, comparable to the reference group (P = .803 and P = .924). Mean follow-up period was 6.2 ± 5.5 years (maximum follow-up time 20 years; 98% complete). Survival at 1, 5, and 12 years in the Celsior and HTK-Custodiol groups was 82.6 ± 2.2% vs 85.2 ± 3.8%, 79.4 ± 2.4% vs 82.1 ± 4.3%, and 66.8 ± 3.3% vs 62.9 ± 7.3%, respectively (P = .706) (Figure 1). Survival at 1, 5, and 12 years in the St Tomas group was 81.5 ± 3.4%, 71.9 ± 4.1%, and 65.5 ± 5.2%, respectively, comparable to the reference group (P = .640) (Figure 2).
Kaplan-Meier Post-Transplant Survival Curves in Celsior and HTK-Custodiol Groups
Kaplan-Meier Post-Transplant Survival Curves in Celsior and St Thomas Groups
Using the Celsior solution as the comparator for survival probability, the hazard function analysis showed the HTK-Custodiol and the St Thomas not statistically distinct from the Celsior (HR 1.06, P = .795 and HR 1.03, P = .748, respectively).
Post-transplant rejection
Overall, the rate of post-transplant rejection was 51.5%. The rejection was cellular in the 49.7% of the cases and humoral in the 5.3%. No significant difference was detected in the HTK-Custodiol and St Thomas groups when compared to the reference group. Detailed data are shown in Table 4.
Univariate and multivariable analysis
Univariate and multivariable Cox regression model analyses were performed to identify risk factors for late mortality. In the univariate analysis, many factors have been found to be significant. Multivariate analysis identified increasing recipient and donor age, recipient chronic renal failure, total ischaemic time, and severe PGD as independent risk factors for late mortality. Details are provided in Table 5.
DISCUSSION
The variety of myocardial preservation solutions and strategies utilized by the heart transplant centres reflects the lack of consensus on the optimal methods.4^,^9 Preservation solutions can be grouped broadly into extracellular and intracellular. While extracellular solutions induce cardiac arrest via depolarization, the intracellular solutions reduce the membrane potential resting state, thus preventing the generation of action potentials. Celsior is an extracellular high sodium and low potassium solution, with glutamate as energy substrate and reduced glutathione and histidine as oxygen-free radical scavengers. HTK-Custodiol is classified as an intracellular, crystalloid cardioplegia due to its low sodium and calcium content. Sodium depletion of the extracellular space causes a hyperpolarization of the plasma membrane of myocytes, inducing cardiac arrest in diastole. The main characteristics of this solution is that it allows a safe cardioplegic arrest time up to 3 h.3^,^5^,^6^,^10 Hachida et al indicated that the promotion of anaerobic glycolysis during ischaemic by HTK-Custodiol cardioplegia results in prolonged preservation of the energetic and contractile function of the heart.11 Therefore, following the cardioplegia administration protocol uniformly recognized in the literature, we repeated a second half dose (half the initial dose) of HTK-Custodiol only if the total ischaemia time exceeded 180 min.12 St Thomas No. 2 is a crystalloid extracellular cardioplegia which provides a rapid diastolic cardiac arrest by high potassium and magnesium concentration as well as by the stabilizing effect of procaine hydrochloride on membrane.
HTK-Custodiol cardioplegia in donors significantly increased severe PGD incidence in our study, roughly doubling the rate compared to the reference group. Despite this, comparable in-hospital mortality rates between the groups (13.6% vs 12.6%; P = .803) were observed. While PGD is a clinical diagnosis of severe ventricular dysfunction within 24 h post-transplant with no identifiable secondary cause, microscopic examination can show ischaemia-reperfusion injury and early inflammatory responses. Common histological features observed in PGD include myocyte oedema, contraction band necrosis, interstitial haemorrhage, and varying degrees of inflammatory cell infiltration, predominantly neutrophils and macrophages. These findings reflect the acute cellular damage and innate immune activation that occur during the donor heart preservation and reperfusion.13 However, it is important to note that these histological changes are often non-specific and can overlap with other forms of graft injury, such as early rejection or donor-related myocardial abnormalities.
Regarding the recipient characteristics, although the pre-operative ECMO rate was significantly higher in the St Thomas group, this finding had no impact neither on mortality nor on PGD incidence. While the most of the literature has shown that pre-operative ECMO support is associated with higher morbidity and mortality,14 selected studies have demonstrated similar post-transplant survival.15 Although our data are not strong enough to demonstrate a protective effect of the St Thomas solution in this subgroup of patients, this finding invites reflection.
Our data did not show an improvement in mid- and long-term survival associated with 1 of the 3 solutions. In a recent comparison of HTK-Custodiol and St Thomas as cardiac preservation solution in HTx, Dulguerov et al16 found no difference in the rate of severe post-transplant PGD and a significantly improved mid-term survival associated with the use of HTK-Custodiol solution. However, they used the 2 solutions separately in different eras (2009-2015 St Thomas, 2016-2020 HTK-Custodiol) and this may have significantly influenced the results, considering that the mean follow-up of the HTK-Custodiol patients was considerably shorter than for St Thomas patients (3.1 vs 7.0 years). Seen from the meta-analysis of results from 147 hearts comparing HTK-Custodiol with Celsior solution, heart dysfunction and in-hospital mortality had no statistical difference in the 2 preservation solutions but the Celsior tended to have better outcomes.17 Karduz et al18 evaluated the effect of HTK-Custodiol, St Thomas, and Del Nido solutions functionally and biochemically in a rat model of donor heart. HTK-Custodiol administration led to reduced myocardial contraction, decreased ATP level, increased TNF-α, and increased troponin I levels. The authors conclude that HTK-Custodiol had the weakest protection in inflammation, oxidative stress, and myocardial contractile strength. In a similar transplantation model, an imbalance between antioxidants and oxidants following HTK-Custodiol administration has shown to be associated with oxidative stress.3 Although these studies provide solid data, the inherent limitations of the animal model do not allow us to transpose the results directly to humans.
With respect to post-transplant rejection, we found no significant difference among the groups. Accordingly, Carter et al,19 in a large recent study, failed to show significant difference in rejection when comparing Wisconsin, Celsior, and HTK-Custodiol solutions, whereas, in another comparative study among HTK-Custodiol, Celsior, and Viaspan solutions,20 Celsior allowed for better post-transplant heart recovery and accounted for less incidence for vasculopathy and chronic rejection in the mid-term follow-up.
In the multivariate analysis for late mortality, none of the 3 solutions used was found to be an independent risk factor. This finding suggests that, in the context of contemporary HTx practices and patient management, the choice of these specific cardioplegia solutions may not be a primary determinant of long-term survival outcomes.
CONCLUSION
The choice of myocardial preservation solution in HTx remains a subject of ongoing debate and research. While HTK-Custodiol offers the advantage of single-dose administration and may improve some early and mid-term outcomes like inotropic scores and rejection rates, concerns exist regarding its potential association with higher PGD rates. St Thomas and Celsior solutions demonstrate promise in reducing early post-transplant morbidity, such as the need for mechanical support, with comparable long-term survival. Overall, our data show comparable results of the 3 solutions except for severe PGD rate and temporary mechanical circulatory support. Although this data had no impact on mortality, we believe that HTK-Custodiol solution should be used with caution for preservation of donor hearts. Therefore, currently, we favour the other 2 solutions. Nevertheless, the overall impact on outcomes is multifaceted, with various studies presenting nuanced findings. Further large-scale, prospective, randomized trials are needed to definitively establish the optimal cardioplegic solution for HTx, taking into account different donor and recipient characteristics and ischaemic times.
Limitation
The major limitation of the current investigation is the retrospective approach of the analysis. Moreover, this is a single-center study with a limited number of patients when compared to the most qualified international and national registries, and this may reduce the statistical power of some well-known risk factors. However, the completeness of data collection represents a strong point of our work.
There was no prespecified plan to adjust for multiple comparisons; hence, findings should be interpreted as exploratory in nature.
The choice of the preservation solution was left to the surgeon and this could have introduced some hidden bias and confounders in the results. Nevertheless, each surgeon showed a strong and stable preference for 1 solution during the study period.
According to the HTK-Custodiol administration protocol, a single dose of this solution was administered into the hearts of the donors unless the total ischaemia time exceeded 3 h and this, in a particular context such as cold ischaemia of HTx, could have influenced the results.
Finally, the reference group (Celsior) includes a larger number of patients and has a longer follow-up time and this may affect the results.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hullin R , Meyer P, Yerly P, Kirsch M. Cardiac surgery in advanced heart failure. J Clin Med. 2022;11:773.35160225 10.3390/jcm 11030773 PMC 8836496 · doi ↗ · pubmed ↗
- 2Kukreja J , Campo-Canaveral de la Cruz JL, Van Raemdonck D, et al The 2024 American Association for Thoracic Surgery expert consensus document: current standards in donor lung procurement and preservation. J Thorac Cardiovasc Surg. 2025;169:484-504.39826938 10.1016/j.jtcvs.2024.08.052 · doi ↗ · pubmed ↗
- 3Renner A , Sagstetter MR, Götz ME, et al Heterotopic rat heart transplantation: severe loss of glutathione in 8-hour ischemic hearts. J Heart Lung Transplant. 2004;23:1093-1102.15454177 10.1016/j.healun.2003.08.012 · doi ↗ · pubmed ↗
- 4Cannata A , Botta L, Colombo T, et al Does the cardioplegic solution have an effect on early outcomes following heart transplantation. Eur J Cardiothorac Surg. 2012;41:e 48-e 52; discussion e 52.22423082 10.1093/ejcts/ezr 321 · doi ↗ · pubmed ↗
- 5Bretschneider HJ. Myocardial protection. Thorac Cardiovasc Surg. 1980;28:295-302.6161427 10.1055/s-2007-1022099 · doi ↗ · pubmed ↗
- 6Bretschneider HJ , Hübner G, Knoll D, Lohr B, Nordbeck H, Spieckermann PG. Myocardial resistance and tolerance to ischemia: physiological and biochemical basis. J Cardiovasc Surg (Torino). 1975;16:241-260.
- 7Settepani F , Pedrazzini GL, Olivieri GM, et al Long-term effects of primary graft dysfunction after heart transplantation. J Card Surg. 2022;37:1290-1298.35229361 10.1111/jocs.16364 · doi ↗ · pubmed ↗
- 8Kobashigawa J , Zuckermann A, Macdonald P, et al; Consensus Conference participants. Report from a consensus conference on primary graft dysfunction after cardiac transplantation. J Heart Lung Transplant. 2014;33:327-340.24661451 10.1016/j.healun.2014.02.027 · doi ↗ · pubmed ↗