A Rare Presentation of Babesia‐Associated Splenic Infarction in an Immunocompetent Young Male With Mild Parasitemia
Jamal A. Anthony, Dejan Nikolic, Rosalie Pepe, Henry Fraimow

TL;DR
A young, healthy man with mild babesiosis experienced a rare complication of splenic infarction, highlighting the disease's potential severity even with low parasite levels.
Contribution
Reports a rare case of splenic infarction in a young, immunocompetent individual with mild babesiosis parasitemia.
Findings
A young, immunocompetent male developed severe babesiosis with splenic infarction.
The patient had low parasitemia levels, challenging the assumption that high levels are required for severe disease.
The case highlights the need for awareness of rare complications in mild babesiosis cases.
Abstract
Babesiosis is a vector‐borne protozoal disease primarily transmitted by the Ixodes scapularis tick, though it can also be transmitted through blood transfusions from infected donors. The illness can be asymptomatic or present with mild flu‐like symptoms. Still, in severe cases, it can lead to disseminated intravascular coagulation and severe hemolytic anemia, sometimes necessitating management in the intensive care unit. Traditionally, severe babesiosis has been linked to individuals over 50 years old, asplenia, and those who are immunocompromised. Notably, parasitemia levels greater than 10% are also associated with severe disease. However, we report a case of a young, immunocompetent male with severe babesiosis exhibiting severe hemolytic anemia and a rare complication of splenic infarction despite a low level of parasitemia. This case emphasizes that significant clinical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
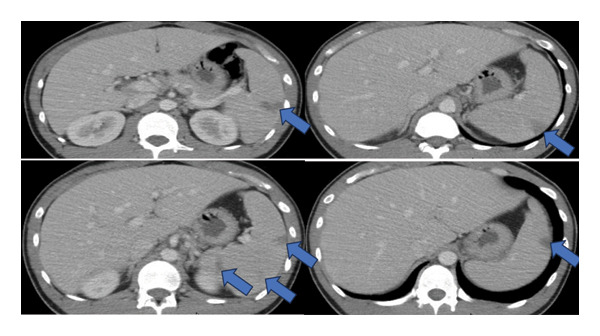 Figure 1
Figure 1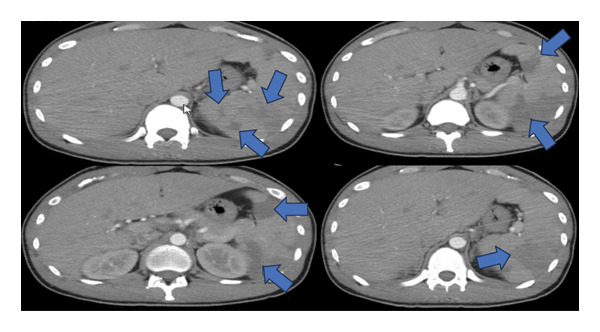 Figure 2
Figure 2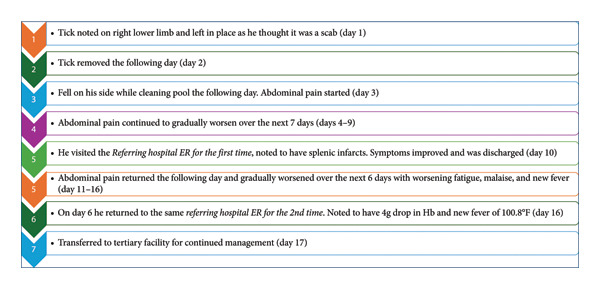 Figure 3
Figure 3| Location/institution | Referring hospital visit 1 | Referring hospital visit 2 (6 days later) |
Tertiary institution
| |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hospital day | 1 | 1a | 1b | 1 | 2a | 2b | 2c | 3 | 4 | 5 | 6 | 7 |
| CBC results | ||||||||||||
| WBC (NR: 4.50–11.00 103/μL) | 5.18 | 8.37 | 8.12 | 7.52 | 7.00 | 7.30 | 7.71 | 7.55 | 7.59 | 7.86 | 6.74 | 7.01 |
| Hemoglobin (NR: 14.0–18.0 g/dL) | 12.4 | 8.4 | 7.9 | 7.2 | 7.0 | 6.9 | 7.1 | 6.6 | 6.5 | 7.9 | 8.0 | 8.9 |
| Hematocrit (NR: 42.0%–52.0%) | 36.2 | 27.1 | 24.7 | 22.8 | 22.4 | 22.4 | 22.2 | 20.7 | 20.7 | 24.9 | 25.9 | 29.4 |
| MCV (NR: 80.0–94.0 fL) | 84.6 | 84.7 | 87.3 | 87.4 | 87.5 | 88.2 | 87.7 | 88.5 | 90.4 | 89.9 | 93.2 | 95.8 |
| MCH (NR: 27.0–31.0 pg) | 29.0 | 27.8 | 27.9 | 27.6 | 27.3 | 27.2 | 28.1 | 28.2 | 28.4 | 28.5 | 28.8 | 29.0 |
| MCHC (NR: 33.0–36.0 g/dL) | 34.3 | 32.8 | 32.0 | 31.6 | 31.3 | 30.8 | 32.0 | 31.9 | 31.4 | 31.7 | 30.9 | 30.3 |
| Platelet count (NR: 150–400 103/μL) | 156 | 169 | 181 | 179 | 204 | 213 | 196 | 216 | 213 | 230 | 275 | 338 |
| Hemolysis, anemia, and coagulation studies | ||||||||||||
| Fibrinogen level (NR: 173–430 mg/dL) | 633 | |||||||||||
| Ferritin (NR: 15–400 ng/mL) | > 1800 | 2366 | ||||||||||
| INR (0.8–1.2) | 1.3 | 1.4 | 1.3 | |||||||||
| Prothrombin time (NR: 9.9–13.5 s) | 14.9 | 16.1 | 15.3 | |||||||||
| Activated PTT (NR: 29.1–35.7 s) | 30.1 | 23.2 | 29.7 | |||||||||
| Haptoglobin (NR: 30–200 mg/dL) | < 15 | < 10 | < 10 | < 10 | < 10 | < 10 | < 10 | < 10 | ||||
| LDH (NR: 110–230 U/L) | 701 | 749 | 720 | 906 | 789 | 744 | ||||||
| Reticulocyte count (NR: 0.5%–2.0%) | 7.20 | 8.2 | ||||||||||
| Reticulocyte absolute count (NR: 0.0235–0.1220 106/μl) | 0.1886 | 0.2080 | ||||||||||
| Blood parasite smear % parasitemia | 1.4% | 1.3% | 1.0% | |||||||||
| Location/institution | Referring hospital visit 1 | Referring hospital visit 2 (6 days later) |
Tertiary institution
| |||||
|---|---|---|---|---|---|---|---|---|
| Hospital day | 1 | 1 | 1 | 2 | 3 | 4 | 5 | 6 |
| Glucose (NR: 70–110 mg/dL) | 87 | 112 | 96 | 111 | 140 | 117 | 114 | 141 |
| BUN (NR: 9–23 mg/dL) | 11 | 8 | 10 | 10 | 8 | 10 | 10 | 11 |
| Creatinine (NR: 0.60–1.20 mg/dL) | 0.93 | 0.87 | 0.92 | 0.77 | 0.73 | 0.76 | 0.76 | 0.84 |
| Sodium (NR: 135–145 mmol/L) | 138 | 133 | 139 | 135 | 132 | 136 | 134 | 138 |
| Potassium (NR: 3.5–5.0 mmol/L) | 3.9 | 4.3 | 4.5 | 4.6 | 4.4 | 4.5 | 4.0 | 4.2 |
| Chloride, serum (NR: 96–108 mmol/L) | 102 | 96 | 100 | 98 | 97 | 100 | 98 | 98 |
| CO2 (NR: 22–28 mmol/L) | 25 | 27 | 26 | 26 | 24 | 25 | 26 | 23 |
| Albumin (NR: 3.8–5.3 g/dL) | 4 | 3.9 | 3.3 | 3.3 | 2.9 | 3.1 | 3.6 | 3.8 |
| eGFR | ||||||||
| > 59 mL/min/[1.73_m2] | > 60 | > 60 | 116 | 125 | 127 | 126 | 126 | 122 |
| Anion Gap (NR: 7–16 mmol/L) | 11 | 10 | 13 | 11 | 11 | 11 | 10 | 17 |
| AST (NR: 10–35 U/L) | 36 | 58 | 52 | 48 | 64 | 109 | 65 | 50 |
| ALT (NR: 6–45 U/L) | 23 | 80 | 65 | 64 | 72 | 125 | 120 | 109 |
| Alkaline phosphatase (NR: 39–117 u/L) | 81 | 107 | 107 | 104 | 114 | 118 | 124 | 142 |
| Bilirubin total (NR: 0.0–1.2 mg/dL) | 2.6 | 1.6 | 1.9 | 2.1 | 1.3 | 1.2 | 0.9 | 0.8 |
| Bilirubin direct (NR: 0.0–0.3 mg/dL) | 0.5 | 0.5 | 0.8 | 0.9 | 0.4 | 0.4 | 0.4 | 0.2 |
| Protein (NR: 6.0–8.5 g/dL) | 7.8 | 8.4 | 7.5 | 7.4 | 6.9 | 7.2 | 7.5 | 8.3 |
| Case no. | Author | Year | Age | Comorbidities | Presenting symptoms | Immune status | Splenic pathology | Babesia species | Parasitemia level | Coinfection | Missed on initial presentation | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. | Javed et al. [ | 2001 | 85 (M) | Hypertension | Fever, chills, malaise | Immunocompetent | Infarction | Microti | 8% | Ehrlichiosis |
| Patient expired despite medical therapy |
| 2. | Froberg et al. [ | 2008 | 56 (M) | Hypertension, cigarette smoking, and bilateral inguinal hernia repair status post laparoscopic surgery | Two week history of fever up to 103°F, chills, myalgia, and 10‐pound weight loss | Immunocompetent | Rupture | Microti | Not reported | Lyme disease | No | Splenectomy + medical management |
| 3. | Kuwayama and Briones. [ | 2008 | 61 (M) | None | Fever, chills, headache, and malaise | Immunocompetent | Rupture | Microti | 5% | Not reported | No | Splenectomy + medical management |
| 4. | Florescu et al. [ | 2008 | 58 (M) | malaria in childhood | Fever, chills, myalgias, and left upper quadrant pain | Immunocompetent | Infarction | Microti | 0.5% | Anaplasmosis | No | Medical management |
| 5. | Florescu et al. [ | 2008 | 75 (F) | Colon cancer status postcompletion of chemotherapy 5 years prior and hypertension | Fever, night sweats, and fatigue | Immunocompetent but a history of being immunocompromised | Infarction | unknown | < 1% | No |
| Patient demised despite medical management |
| 6. | El Khoury et al. [ | 2011 | 36 (M) | None | Left upper quadrant pain and 2 weeks of fever and chills | Immunocompetent | Infarction | Microti | 3%–4% | No | No | Medical management |
| 7. | El Khoury et al. [ | 2011 | 70 (M) | Lyme disease 10 years prior | A 4 day history of malaise, fatigue, fevers, chills, and diffuse abdominal pain | Immunocompetent | Rupture | Microti | 2% | No | No | Splenectomy + medical management |
| 8. | Reis et al. [ | 2011 | 70 (M) | Not reported | Three day history of fever, nausea, and vomiting, and sudden onset of abdominal pain | Not reported | Rupture | Microti | Not reported | No | Selective splenic artery embolization | |
| 9. | Abbas et al. [ | 2011 | 23 (M) | None | Fever, chills, weight loss, malaise | Immunocompetent | Rupture | Microti | 30% | No |
| Splenectomy + medical management |
| 10. | Tobler et al. [ | 2011 | 54 (M) | Lyme disease | Left upper quadrant abdominal pain, fever of 102.3 °F, nausea, chills, night sweats, and dark urine | Immunocompetent | Rupture | Microti | 3% | No | No | Splenectomy + medical Management |
| 11. | Usatii et al. [ | 2014 | 54 (M) | None | Left upper quadrant abdominal pain for 1 week along with abdominal distention and subjective fevers and headache | Immunocompetent | Rupture | Microti | Not reported | No |
| Splenectomy + medical management |
| 12. | Farber et al. [ | 2015 | 59 (F) | CAD, hyperlipidemia, and depression | A syncopal episode after 2 weeks of headaches, fatigue, chills, abdominal pain, nausea, and diarrhea | Immunocompetent | Rupture | Microti | 0.9% | No | No | Splenectomy + medical management |
| 13. | Al Zoubi et al. [ | 2016 | 72 (M) | Hypertension | Fever, chills, weight loss, and abdominal pain | Immunocompetent | Infarction | Microti | 0.5% | No |
| Medical management |
| 14. | Dumic et al. [ | 2018 | 79 (F) | Hypertension, coronary artery disease, and atrial fibrillation on warfarin | Left‐sided chest pain, extreme fatigue, and dizziness without any fever but she represented on postop day 10 with fevers and abdominal pain. | Immunocompetent | Rupture | Microti | 1.6% | Lyme |
| Splenectomy + medical management |
| 15. | Blackwood et al. [ | 2018 | 51 (M) | Hypertension and atrial fibrillations | Syncope after a 5 day history of fever, chills, rigors, sweats, and general malaise with worsening abdominal pain | Immunocompetent | Rupture | Microti | 0.9% | No | No | Splenectomy + medical management |
| 16. | Blackwood and Binder [ | 2018 | 61 (M) | Hypertension and hyperlipidemia | Abdominal pain and 3 days of fever, chills, myalgias, weakness, and decreased appetite. | Immunocompetent | Infarction | Microti | 0.44% | No | No | Medical management |
| 17. | Gupta et al. [ | 2019 | 53 (M) | Tobacco use and cholecystitis status postcholecystectomy | Fatigue, fever, and abdominal pain | Immunocompetent | Infarction | Microti | 1.5% | No | No | Medical management |
| 18. | Sung et al. [ | 2021 | 46 (M) | None | Abdominal pain | Immunocompetent | Rupture | Microti | 0.1% | Lyme disease | No | Splenectomy + medical management |
| 19. | Sung et al. [ | 2021 | 51 (M) | Obesity status postgastric bypass surgery | Fever and left‐sided abdominal pain | Immunocompetent | Infarction | Microti | 0.6% | Lyme disease |
| Medical management |
| 20. | Mateja et al. [ | 2024 | 70 (M) | Hypertension, hyperlipidemia, BPH, asthma, gastroesophageal reflux disease, depression, anxiety, and schizoaffective disorder | Bilateral flank pain, sweating, nausea, and chills for 3 days. He reported having three syncopal episodes on the day of the presentation. | Immunocompetent | Rupture | Microti | 13% | Not reported |
| Splenectomy + medical management |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVector-borne infectious diseases · Parasites and Host Interactions · Entomological Studies and Ecology
Learning Points
- •Babesia‐associated splenic injury is a serious manifestation of babesiosis that does not always correlate with higher parasitemia levels; most cases are associated with low levels (< 5%).
- •Coinfection with other vector‐borne diseases may amplify clinical severity.
- •The patient’s clinical course should be the primary consideration in treating babesiosis, rather than the degree of parasitemia alone (except when the percent parasitemia is greater than 10%, in which case red cell exchange is recommended regardless of clinical presentation).
- •For patients presenting with atraumatic splenic injuries or splenic injuries that are out of proportion to the trauma, it is essential to rule out babesiosis, as it is an emerging cause of atraumatic splenic injury. This helps to prevent treatment delays.
- •Atraumatic splenic injury may be the only presenting sign, occurring without fever or systemic symptoms. Babesia‐associated splenic injury is a serious complication of the disease that does not require traditional risk factors for severe babesiosis, such as age over 50, immunocompromised state, or asplenia.
1. Introduction
Babesiosis is a vector‐borne illness caused by an intraerythrocytic protozoal parasite. It is most commonly transmitted by the Ixodes scapularis tick and, less commonly, by blood transfusion or organ transplantation [1–7]. There are many Babesia species. Most infect domestic and wild animals, with a few species causing human babesiosis [1–3]. Babesia microti, Babesia duncani, and Babesia divergens are known to cause human babesiosis [1–3]. It was first discovered in 1969 in an immunocompetent male from Nantucket Island, Massachusetts, who was found to have Babesia microti, giving it the name “Nantucket fever” [1, 2]. In the United States of America (USA), most cases are caused by Babesia microti [1–5].
Babesiosis is endemic in many states of the USA, particularly in the northeastern and midwestern regions, with a seasonal peak between the late spring and early fall (May–September) [1, 2]. The incubation period usually ranges from 1 to 4 weeks after the initial tick bite [1]. However, transfusion‐related cases tend to have a longer latency period, ranging from 1 to 9 weeks [1]. It can be asymptomatic in about 20% of patients [3]. Mild to moderate disease with symptoms often present with fever, chills, diaphoresis, headaches, myalgia, arthralgia, nausea, anorexia, and cough [1, 2]. Vannier et al. [1] also report that some patients may experience emotional lability, depression, hyperesthesia, sore throat, abdominal pain, vomiting, conjunctival injection, photophobia, and weight loss.
Spontaneous splenic injury (infarction or rupture) is a rare but severe complication of babesiosis that can result in an increased risk of morbidity and mortality if missed on initial presentation [2]. Here, we highlight that this complication of babesiosis can occur at any age, regardless of comorbidities or level of parasitemia.
2. Case Presentation
2.1. Case Description
A young, healthy male in his late 20s presented to a referring hospital in the early summertime with a worsening left upper quadrant pain, nausea, and vomiting, raising concerns about internal injury from a low‐level fall that had occurred 1 week before. He was hemodynamically stable and afebrile at that time. A computed tomography (CT) scan of the abdomen and pelvis suggested a splenic infarct or laceration (Figure 1). His symptoms improved after intravenous fluids and pain medication, and given that he was also hemodynamically stable, he was discharged with plans for outpatient follow‐up and repeat imaging.
Still images from CT abdomen and pelvis from the patient’s first presentation to the referring hospital demonstrating splenic lesions, thought to be splenic infarcts.
Six days later, he returned to the same hospital with increased fatigue, malaise, worsening left upper quadrant pain, decreased appetite, fever, and chills. A repeat complete blood count (CBC) showed that the hemoglobin level dropped from 12.4 g/dL to 8.4 g/dL (Table 1). Another CT indicated enlarged splenic infarcts with possible hematoma (Figure 2). He was admitted for further evaluation.
Table 1: Showing the trend of the patient’s CBC, hemolysis, coagulation, and anemia studies throughout his admissions.
<table><col/><col/><col/><col/><col/><col/><col/><col/><col/><col/><col/><col/><col/><thead><tr><th align="left" rowspan="1" colspan="1">Location/institution</th><th align="center" rowspan="1" colspan="1">Referring hospital visit 1</th><th colspan="2" align="center" rowspan="1">Referring hospital visit 2 (6 days later)</th><th colspan="9" align="center" rowspan="1"> <p>Tertiary institution</p> <p> <inline-graphic xmlns:xlink="http://www.w3.org/1999/xlink"/> </p> </th></tr></thead><tbody><tr><td align="left" rowspan="1" colspan="1">Hospital day</td><td align="center" rowspan="1" colspan="1">1</td><td align="center" rowspan="1" colspan="1">1a</td><td align="center" rowspan="1" colspan="1">1b</td><td align="center" rowspan="1" colspan="1">1</td><td align="center" rowspan="1" colspan="1">2a</td><td align="center" rowspan="1" colspan="1">2b</td><td align="center" rowspan="1" colspan="1">2c</td><td align="center" rowspan="1" colspan="1">3</td><td align="center" rowspan="1" colspan="1">4</td><td align="center" rowspan="1" colspan="1">5</td><td align="center" rowspan="1" colspan="1">6</td><td align="center" rowspan="1" colspan="1">7</td></tr><tr><td align="left" rowspan="1" colspan="1">CBC results</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td></tr><tr><td align="left" rowspan="1" colspan="1"> WBC (NR: 4.50–11.00 10<sup>3</sup>/μL)</td><td align="center" rowspan="1" colspan="1">5.18</td><td align="center" rowspan="1" colspan="1">8.37</td><td align="center" rowspan="1" colspan="1">8.12</td><td align="center" rowspan="1" colspan="1">7.52</td><td align="center" rowspan="1" colspan="1">7.00</td><td align="center" rowspan="1" colspan="1">7.30</td><td align="center" rowspan="1" colspan="1">7.71</td><td align="center" rowspan="1" colspan="1">7.55</td><td align="center" rowspan="1" colspan="1">7.59</td><td align="center" rowspan="1" colspan="1">7.86</td><td align="center" rowspan="1" colspan="1">6.74</td><td align="center" rowspan="1" colspan="1">7.01</td></tr><tr><td align="left" rowspan="1" colspan="1"> Hemoglobin (NR: 14.0–18.0 g/dL)</td><td align="center" rowspan="1" colspan="1">12.4</td><td align="center" rowspan="1" colspan="1">8.4</td><td align="center" rowspan="1" colspan="1">7.9</td><td align="center" rowspan="1" colspan="1">7.2</td><td align="center" rowspan="1" colspan="1">7.0</td><td align="center" rowspan="1" colspan="1">6.9</td><td align="center" rowspan="1" colspan="1">7.1</td><td align="center" rowspan="1" colspan="1">6.6</td><td align="center" rowspan="1" colspan="1">6.5</td><td align="center" rowspan="1" colspan="1">7.9</td><td align="center" rowspan="1" colspan="1">8.0</td><td align="center" rowspan="1" colspan="1">8.9</td></tr><tr><td align="left" rowspan="1" colspan="1"> Hematocrit (NR: 42.0%–52.0%)</td><td align="center" rowspan="1" colspan="1">36.2</td><td align="center" rowspan="1" colspan="1">27.1</td><td align="center" rowspan="1" colspan="1">24.7</td><td align="center" rowspan="1" colspan="1">22.8</td><td align="center" rowspan="1" colspan="1">22.4</td><td align="center" rowspan="1" colspan="1">22.4</td><td align="center" rowspan="1" colspan="1">22.2</td><td align="center" rowspan="1" colspan="1">20.7</td><td align="center" rowspan="1" colspan="1">20.7</td><td align="center" rowspan="1" colspan="1">24.9</td><td align="center" rowspan="1" colspan="1">25.9</td><td align="center" rowspan="1" colspan="1">29.4</td></tr><tr><td align="left" rowspan="1" colspan="1"> MCV (NR: 80.0–94.0 fL)</td><td align="center" rowspan="1" colspan="1">84.6</td><td align="center" rowspan="1" colspan="1">84.7</td><td align="center" rowspan="1" colspan="1">87.3</td><td align="center" rowspan="1" colspan="1">87.4</td><td align="center" rowspan="1" colspan="1">87.5</td><td align="center" rowspan="1" colspan="1">88.2</td><td align="center" rowspan="1" colspan="1">87.7</td><td align="center" rowspan="1" colspan="1">88.5</td><td align="center" rowspan="1" colspan="1">90.4</td><td align="center" rowspan="1" colspan="1">89.9</td><td align="center" rowspan="1" colspan="1">93.2</td><td align="center" rowspan="1" colspan="1">95.8</td></tr><tr><td align="left" rowspan="1" colspan="1"> MCH (NR: 27.0–31.0 pg)</td><td align="center" rowspan="1" colspan="1">29.0</td><td align="center" rowspan="1" colspan="1">27.8</td><td align="center" rowspan="1" colspan="1">27.9</td><td align="center" rowspan="1" colspan="1">27.6</td><td align="center" rowspan="1" colspan="1">27.3</td><td align="center" rowspan="1" colspan="1">27.2</td><td align="center" rowspan="1" colspan="1">28.1</td><td align="center" rowspan="1" colspan="1">28.2</td><td align="center" rowspan="1" colspan="1">28.4</td><td align="center" rowspan="1" colspan="1">28.5</td><td align="center" rowspan="1" colspan="1">28.8</td><td align="center" rowspan="1" colspan="1">29.0</td></tr><tr><td align="left" rowspan="1" colspan="1"> MCHC (NR: 33.0–36.0 g/dL)</td><td align="center" rowspan="1" colspan="1">34.3</td><td align="center" rowspan="1" colspan="1">32.8</td><td align="center" rowspan="1" colspan="1">32.0</td><td align="center" rowspan="1" colspan="1">31.6</td><td align="center" rowspan="1" colspan="1">31.3</td><td align="center" rowspan="1" colspan="1">30.8</td><td align="center" rowspan="1" colspan="1">32.0</td><td align="center" rowspan="1" colspan="1">31.9</td><td align="center" rowspan="1" colspan="1">31.4</td><td align="center" rowspan="1" colspan="1">31.7</td><td align="center" rowspan="1" colspan="1">30.9</td><td align="center" rowspan="1" colspan="1">30.3</td></tr><tr><td align="left" rowspan="1" colspan="1"> Platelet count (NR: 150–400 10<sup>3</sup>/μL)</td><td align="center" rowspan="1" colspan="1">156</td><td align="center" rowspan="1" colspan="1">169</td><td align="center" rowspan="1" colspan="1">181</td><td align="center" rowspan="1" colspan="1">179</td><td align="center" rowspan="1" colspan="1">204</td><td align="center" rowspan="1" colspan="1">213</td><td align="center" rowspan="1" colspan="1">196</td><td align="center" rowspan="1" colspan="1">216</td><td align="center" rowspan="1" colspan="1">213</td><td align="center" rowspan="1" colspan="1">230</td><td align="center" rowspan="1" colspan="1">275</td><td align="center" rowspan="1" colspan="1">338</td></tr><tr><td align="left" rowspan="1" colspan="1">Hemolysis, anemia, and coagulation studies</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td></tr><tr><td align="left" rowspan="1" colspan="1"> Fibrinogen level (NR: 173–430 mg/dL)</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1">633</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td></tr><tr><td align="left" rowspan="1" colspan="1"> Ferritin (NR: 15–400 ng/mL)</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1">> 1800</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1">2366</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td></tr><tr><td align="left" rowspan="1" colspan="1"> INR (0.8–1.2)</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1">1.3</td><td align="center" rowspan="1" colspan="1">1.4</td><td align="center" rowspan="1" colspan="1">1.3</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td></tr><tr><td align="left" rowspan="1" colspan="1"> Prothrombin time (NR: 9.9–13.5 s)</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1">14.9</td><td align="center" rowspan="1" colspan="1">16.1</td><td align="center" rowspan="1" colspan="1">15.3</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td></tr><tr><td align="left" rowspan="1" colspan="1"> Activated PTT (NR: 29.1–35.7 s)</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1">30.1</td><td align="center" rowspan="1" colspan="1">23.2</td><td align="center" rowspan="1" colspan="1">29.7</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td></tr><tr><td align="left" rowspan="1" colspan="1"> Haptoglobin (NR: 30–200 mg/dL)</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1">< 15</td><td align="center" rowspan="1" colspan="1">< 10</td><td align="center" rowspan="1" colspan="1">< 10</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1">< 10</td><td align="center" rowspan="1" colspan="1">< 10</td><td align="center" rowspan="1" colspan="1">< 10</td><td align="center" rowspan="1" colspan="1">< 10</td><td align="center" rowspan="1" colspan="1">< 10</td><td align="center" rowspan="1" colspan="1"> </td></tr><tr><td align="left" rowspan="1" colspan="1"> LDH (NR: 110–230 U/L)</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1">701</td><td align="center" rowspan="1" colspan="1">749</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1">720</td><td align="center" rowspan="1" colspan="1">906</td><td align="center" rowspan="1" colspan="1">789</td><td align="center" rowspan="1" colspan="1">744</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td></tr><tr><td align="left" rowspan="1" colspan="1"> Reticulocyte count (NR: 0.5%–2.0%)</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1">7.20</td><td align="center" rowspan="1" colspan="1">8.2</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td></tr><tr><td align="left" rowspan="1" colspan="1"> Reticulocyte absolute count (NR: 0.0235–0.1220 10<sup>6</sup>/μl)</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1">0.1886</td><td align="center" rowspan="1" colspan="1">0.2080</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td></tr><tr><td align="left" rowspan="1" colspan="1"> Blood parasite smear % parasitemia</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1">1.4%</td><td align="center" rowspan="1" colspan="1">1.3%</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1">1.0%</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td></tr></tbody></table>Still images from CT abdomen and pelvis from the patient’s 2nd presentation to the referring hospital, 6 days after being discharged after his first presentation. These images demonstrate significantly enlarged splenic infarcts (blue arrows), splenomegaly, and hepatomegaly.
During hospitalization, he experienced fevers of up to 100.8 ^o^F, and his hemoglobin decreased from 8.9 to 7.9 g/dL, labs confirmed hemolysis (Table 1). His complete metabolic panel demonstrated normal renal function, mild transaminitis, and indirect hyperbilirubinemia (Table 2).
Table 2: Complete metabolic panel.
<table><col/><col/><col/><col/><col/><col/><col/><col/><col/><thead><tr><th align="left" rowspan="1" colspan="1">Location/institution</th><th align="center" rowspan="1" colspan="1">Referring hospital visit 1</th><th align="center" rowspan="1" colspan="1">Referring hospital visit 2 (6 days later)</th><th colspan="6" align="center" rowspan="1"> <p>Tertiary institution</p> <p> <inline-graphic xmlns:xlink="http://www.w3.org/1999/xlink"/> </p> </th></tr></thead><tbody><tr><td align="left" rowspan="1" colspan="1">Hospital day</td><td align="center" rowspan="1" colspan="1">1</td><td align="center" rowspan="1" colspan="1">1</td><td align="center" rowspan="1" colspan="1">1</td><td align="center" rowspan="1" colspan="1">2</td><td align="center" rowspan="1" colspan="1">3</td><td align="center" rowspan="1" colspan="1">4</td><td align="center" rowspan="1" colspan="1">5</td><td align="center" rowspan="1" colspan="1">6</td></tr><tr><td align="left" rowspan="1" colspan="1">Glucose (NR: 70–110 mg/dL)</td><td align="center" rowspan="1" colspan="1">87</td><td align="center" rowspan="1" colspan="1">112</td><td align="center" rowspan="1" colspan="1">96</td><td align="center" rowspan="1" colspan="1">111</td><td align="center" rowspan="1" colspan="1">140</td><td align="center" rowspan="1" colspan="1">117</td><td align="center" rowspan="1" colspan="1">114</td><td align="center" rowspan="1" colspan="1">141</td></tr><tr><td align="left" rowspan="1" colspan="1">BUN (NR: 9–23 mg/dL)</td><td align="center" rowspan="1" colspan="1">11</td><td align="center" rowspan="1" colspan="1">8</td><td align="center" rowspan="1" colspan="1">10</td><td align="center" rowspan="1" colspan="1">10</td><td align="center" rowspan="1" colspan="1">8</td><td align="center" rowspan="1" colspan="1">10</td><td align="center" rowspan="1" colspan="1">10</td><td align="center" rowspan="1" colspan="1">11</td></tr><tr><td align="left" rowspan="1" colspan="1">Creatinine (NR: 0.60–1.20 mg/dL)</td><td align="center" rowspan="1" colspan="1">0.93</td><td align="center" rowspan="1" colspan="1">0.87</td><td align="center" rowspan="1" colspan="1">0.92</td><td align="center" rowspan="1" colspan="1">0.77</td><td align="center" rowspan="1" colspan="1">0.73</td><td align="center" rowspan="1" colspan="1">0.76</td><td align="center" rowspan="1" colspan="1">0.76</td><td align="center" rowspan="1" colspan="1">0.84</td></tr><tr><td align="left" rowspan="1" colspan="1">Sodium (NR: 135–145 mmol/L)</td><td align="center" rowspan="1" colspan="1">138</td><td align="center" rowspan="1" colspan="1">133</td><td align="center" rowspan="1" colspan="1">139</td><td align="center" rowspan="1" colspan="1">135</td><td align="center" rowspan="1" colspan="1">132</td><td align="center" rowspan="1" colspan="1">136</td><td align="center" rowspan="1" colspan="1">134</td><td align="center" rowspan="1" colspan="1">138</td></tr><tr><td align="left" rowspan="1" colspan="1">Potassium (NR: 3.5–5.0 mmol/L)</td><td align="center" rowspan="1" colspan="1">3.9</td><td align="center" rowspan="1" colspan="1">4.3</td><td align="center" rowspan="1" colspan="1">4.5</td><td align="center" rowspan="1" colspan="1">4.6</td><td align="center" rowspan="1" colspan="1">4.4</td><td align="center" rowspan="1" colspan="1">4.5</td><td align="center" rowspan="1" colspan="1">4.0</td><td align="center" rowspan="1" colspan="1">4.2</td></tr><tr><td align="left" rowspan="1" colspan="1">Chloride, serum (NR: 96–108 mmol/L)</td><td align="center" rowspan="1" colspan="1">102</td><td align="center" rowspan="1" colspan="1">96</td><td align="center" rowspan="1" colspan="1">100</td><td align="center" rowspan="1" colspan="1">98</td><td align="center" rowspan="1" colspan="1">97</td><td align="center" rowspan="1" colspan="1">100</td><td align="center" rowspan="1" colspan="1">98</td><td align="center" rowspan="1" colspan="1">98</td></tr><tr><td align="left" rowspan="1" colspan="1">CO2 (NR: 22–28 mmol/L)</td><td align="center" rowspan="1" colspan="1">25</td><td align="center" rowspan="1" colspan="1">27</td><td align="center" rowspan="1" colspan="1">26</td><td align="center" rowspan="1" colspan="1">26</td><td align="center" rowspan="1" colspan="1">24</td><td align="center" rowspan="1" colspan="1">25</td><td align="center" rowspan="1" colspan="1">26</td><td align="center" rowspan="1" colspan="1">23</td></tr><tr><td align="left" rowspan="1" colspan="1">Albumin (NR: 3.8–5.3 g/dL)</td><td align="center" rowspan="1" colspan="1">4</td><td align="center" rowspan="1" colspan="1">3.9</td><td align="center" rowspan="1" colspan="1">3.3</td><td align="center" rowspan="1" colspan="1">3.3</td><td align="center" rowspan="1" colspan="1">2.9</td><td align="center" rowspan="1" colspan="1">3.1</td><td align="center" rowspan="1" colspan="1">3.6</td><td align="center" rowspan="1" colspan="1">3.8</td></tr><tr><td align="left" rowspan="1" colspan="1">eGFR</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1"> </td></tr><tr><td align="left" rowspan="1" colspan="1">> 59 mL/min/[1.73_m2]</td><td align="center" rowspan="1" colspan="1">> 60</td><td align="center" rowspan="1" colspan="1">> 60</td><td align="center" rowspan="1" colspan="1">116</td><td align="center" rowspan="1" colspan="1">125</td><td align="center" rowspan="1" colspan="1">127</td><td align="center" rowspan="1" colspan="1">126</td><td align="center" rowspan="1" colspan="1">126</td><td align="center" rowspan="1" colspan="1">122</td></tr><tr><td align="left" rowspan="1" colspan="1">Anion Gap (NR: 7–16 mmol/L)</td><td align="center" rowspan="1" colspan="1">11</td><td align="center" rowspan="1" colspan="1">10</td><td align="center" rowspan="1" colspan="1">13</td><td align="center" rowspan="1" colspan="1">11</td><td align="center" rowspan="1" colspan="1">11</td><td align="center" rowspan="1" colspan="1">11</td><td align="center" rowspan="1" colspan="1">10</td><td align="center" rowspan="1" colspan="1">17</td></tr><tr><td align="left" rowspan="1" colspan="1">AST (NR: 10–35 U/L)</td><td align="center" rowspan="1" colspan="1">36</td><td align="center" rowspan="1" colspan="1">58</td><td align="center" rowspan="1" colspan="1">52</td><td align="center" rowspan="1" colspan="1">48</td><td align="center" rowspan="1" colspan="1">64</td><td align="center" rowspan="1" colspan="1">109</td><td align="center" rowspan="1" colspan="1">65</td><td align="center" rowspan="1" colspan="1">50</td></tr><tr><td align="left" rowspan="1" colspan="1">ALT (NR: 6–45 U/L)</td><td align="center" rowspan="1" colspan="1">23</td><td align="center" rowspan="1" colspan="1">80</td><td align="center" rowspan="1" colspan="1">65</td><td align="center" rowspan="1" colspan="1">64</td><td align="center" rowspan="1" colspan="1">72</td><td align="center" rowspan="1" colspan="1">125</td><td align="center" rowspan="1" colspan="1">120</td><td align="center" rowspan="1" colspan="1">109</td></tr><tr><td align="left" rowspan="1" colspan="1">Alkaline phosphatase (NR: 39–117 u/L)</td><td align="center" rowspan="1" colspan="1">81</td><td align="center" rowspan="1" colspan="1">107</td><td align="center" rowspan="1" colspan="1">107</td><td align="center" rowspan="1" colspan="1">104</td><td align="center" rowspan="1" colspan="1">114</td><td align="center" rowspan="1" colspan="1">118</td><td align="center" rowspan="1" colspan="1">124</td><td align="center" rowspan="1" colspan="1">142</td></tr><tr><td align="left" rowspan="1" colspan="1">Bilirubin total (NR: 0.0–1.2 mg/dL)</td><td align="center" rowspan="1" colspan="1">2.6</td><td align="center" rowspan="1" colspan="1">1.6</td><td align="center" rowspan="1" colspan="1">1.9</td><td align="center" rowspan="1" colspan="1">2.1</td><td align="center" rowspan="1" colspan="1">1.3</td><td align="center" rowspan="1" colspan="1">1.2</td><td align="center" rowspan="1" colspan="1">0.9</td><td align="center" rowspan="1" colspan="1">0.8</td></tr><tr><td align="left" rowspan="1" colspan="1">Bilirubin direct (NR: 0.0–0.3 mg/dL)</td><td align="center" rowspan="1" colspan="1">0.5</td><td align="center" rowspan="1" colspan="1">0.5</td><td align="center" rowspan="1" colspan="1">0.8</td><td align="center" rowspan="1" colspan="1">0.9</td><td align="center" rowspan="1" colspan="1">0.4</td><td align="center" rowspan="1" colspan="1">0.4</td><td align="center" rowspan="1" colspan="1">0.4</td><td align="center" rowspan="1" colspan="1">0.2</td></tr><tr><td align="left" rowspan="1" colspan="1">Protein (NR: 6.0–8.5 g/dL)</td><td align="center" rowspan="1" colspan="1">7.8</td><td align="center" rowspan="1" colspan="1">8.4</td><td align="center" rowspan="1" colspan="1">7.5</td><td align="center" rowspan="1" colspan="1">7.4</td><td align="center" rowspan="1" colspan="1">6.9</td><td align="center" rowspan="1" colspan="1">7.2</td><td align="center" rowspan="1" colspan="1">7.5</td><td align="center" rowspan="1" colspan="1">8.3</td></tr></tbody></table>He was later transferred to our tertiary‐level facility for further management after spending one day admitted to the referring hospital (see Figure 3 for the timeline of events). He then revealed that he lived in a wooded area and had multiple recent tick bites, including one a week before his first visit (see Figure 3). He reported no rash or recent travel. Physical examination was notable for left upper quadrant tenderness with hepatosplenomegaly; there were no rashes, tick bites, or attached ticks.
Timeline of events leading up to the transfer of the patient to our tertiary institution.
2.2. Differential Diagnoses Considered and Management
The patient initially presented to a referring hospital with signs concerning for a traumatic splenic laceration following a fall. However, his stable vital signs and normal hemoglobin 1 week later made such an injury unlikely. Initially, the absence of fever and a normal white blood cell count made an infectious cause less likely, leading to his discharge.
Six days later, he returned with worsening abdominal pain, hemolytic anemia, and fever, expanding the differential diagnosis. Negative Coombs tests made autoimmune hemolytic anemia less probable. To rule out acute retroviral syndrome, 5^th^‐generation HIV testing was performed and was nonreactive. His physical examination and imaging showed no lymphadenopathy or signs of malignancy, such as longstanding unexplained weight loss, fevers, or night sweats. Given his fever, hemolytic anemia, elevated transaminases, and tick exposure, there was concern for tick‐borne illness.
Parasitic forms were observed during microscopic examination of a Giemsa‐stained thin peripheral blood film prepared for CBC with differential assessment. Considering his recent tick bite, residence in a forested area, and living in an endemic region, babesiosis became the leading diagnosis, especially in the absence of travel to a location where he could have been exposed to malaria.
Several distinguishing morphologic features of Babesia were identified: the intracellular ring stages forming tetrads (“maltese crosses”) in infected red blood cells (RBCs) (Figures 4(a), 4(b)) and extracellular forms of the parasite (Figures 5(a), 5(b)). Morphologically, on microscopy, possible infection with Plasmodium (Malaria) species was excluded. Based on these findings, the final diagnosis of Babesiosis was made with a 1.4% parasitemia level.
Figure 4(a) Parasite smear (Giemsa stain 1000×) showing Maltese Crosses (black arrows). (b) Intracellular Babesia microti (Giemsa stain 1000×).(a)(b)
Figure 5(a) Giemsa‐stained thin blood film (1000×) showing extracellular forms of Babesia microti parasites (black arrows). Red arrows showing platelets. (b) Black arrow indicating extracellular Babesia microti (Giemsa stain 1000×). Red arrow showing platelet.(a)(b)
Considering coinfections with other vector‐borne infections transmitted by similar or identical vectors in endemic areas are not uncommon [8], they were also considered. The screening for coinfections revealed acute Lyme disease (IgM western blot positive; IgG immunoblot negative), while the testing was negative for Anaplasma phagocytophilum (no morulae visualized in peripheral blood neutrophils, and PCR using species‐specific primers was negative).
2.3. Treatment
At the beginning of his admission to our tertiary center, the patient had worsening hemolytic anemia even with the initiation of treatment on day one of admission (Table 1). He required a transfusion (days 3 and 4) of 2 units of packed RBCs to maintain his hemoglobin level above 7. As he continued treatment for his babesiosis, his hemolytic anemia stabilized by day 5, and his hemoglobin remained above 7 without the need for further transfusions. Our patient was classified as having mild parasitemia (percentage parasites being < 4%) but with severe clinical disease (severe hemolytic anemia < 10 g/dL, required hospitalization, and his splenic injury). He was treated with atovaquone (750 mg PO BID) + azithromycin (250 mg PO daily) regimen for 10 days. Lyme disease testing was positive, indicating coinfection. Doxycycline 100 mg PO BID was also prescribed (10 days) for coinfection with Borrelia, which was his only identifiable risk factor for severe disease.
2.4. Outcome and Follow‐Up
He remained stable. His abdominal pain and fever resolved by day 5, his splenomegaly improved, and his appetite returned. His hemoglobin also remained stable. As such, he was discharged to finish his course of antibiotics. The patient did well, with complete resolution of his symptoms and no further transfusions.
3. Discussion
3.1. Clinical Relevance
Our patient presented with fever, chills, severe abdominal pain, nausea, anorexia, fatigue, and malaise due to babesiosis, resulting in hospitalization. While most cases do not require hospitalization, babesiosis can lead to up to 21% mortality in hospitalized patients [1–3]. Historically, severe cases are typically observed in patients who are immunocompromised, aged > 50 years, and who have asplenia [1–18]. Additionally, Babesia divergens infection, compared to Babesia microti, babesiosis of any type with severe parasitemia (> 10%), as well as transfusion‐related babesiosis, have been linked to more severe disease [1, 2]. However, a growing body of evidence suggests that severe clinical manifestations of babesiosis, such as spontaneous splenic injury, can occur in immunocompetent young individuals with low levels of parasitemia. Therefore, it is crucial for clinicians to understand how to identify and provide appropriate treatment.
3.2. What This Case Contributes to the Literature
Table 3 shows a list of 20 cases of babesia‐associated splenic injury obtained from our literature review. Additionally, we found a systematic review by Dumic et al. [2] of 34 cases of babesia‐related splenic injury (which already included 17 of the 20 cases reported in Table 3). Our search identified three additional cases (cases 18–20), bringing the total to 37. Therefore, our case is the 38th documented instance. Of the 37 cases, most had low‐grade parasitemia < 5%, were all immunocompetent, and only 3 of 37 (8%) cases found were < 40 years old. Only one case reported by Abbas et al. [14] involved a patient < 30 years old. However, the 23‐year‐old patient described by Abbas et al. had severe parasitemia (30%), which likely contributed to his severe clinical disease and splenic injury.
Table 3: A list of reported babesiosis cases that have been associated with splenic complications and how each one compares to the patient described in this case report.
<table><col/><col/><col/><col/><col/><col/><col/><col/><col/><col/><col/><col/><col/><thead><tr><th align="left" rowspan="1" colspan="1">Case no.</th><th align="center" rowspan="1" colspan="1">Author</th><th align="center" rowspan="1" colspan="1">Year</th><th align="center" rowspan="1" colspan="1">Age</th><th align="center" rowspan="1" colspan="1">Comorbidities</th><th align="center" rowspan="1" colspan="1">Presenting symptoms</th><th align="center" rowspan="1" colspan="1">Immune status</th><th align="center" rowspan="1" colspan="1">Splenic pathology</th><th align="center" rowspan="1" colspan="1">Babesia species</th><th align="center" rowspan="1" colspan="1">Parasitemia level</th><th align="center" rowspan="1" colspan="1">Coinfection</th><th align="center" rowspan="1" colspan="1">Missed on initial presentation</th><th align="center" rowspan="1" colspan="1">Outcome</th></tr></thead><tbody><tr><td align="left" rowspan="1" colspan="1">1.</td><td align="center" rowspan="1" colspan="1">Javed et al. [<xref>19</xref>]</td><td align="center" rowspan="1" colspan="1">2001</td><td align="center" rowspan="1" colspan="1">85 (M)</td><td align="center" rowspan="1" colspan="1">Hypertension</td><td align="center" rowspan="1" colspan="1">Fever, chills, malaise</td><td align="center" rowspan="1" colspan="1">Immunocompetent</td><td align="center" rowspan="1" colspan="1">Infarction</td><td align="center" rowspan="1" colspan="1">Microti</td><td align="center" rowspan="1" colspan="1">8%</td><td align="center" rowspan="1" colspan="1">Ehrlichiosis</td><td align="center" rowspan="1" colspan="1"> <bold>Yes</bold> </td><td align="center" rowspan="1" colspan="1">Patient expired despite medical therapy</td></tr><tr><td align="left" rowspan="1" colspan="1">2.</td><td align="center" rowspan="1" colspan="1">Froberg et al. [<xref>15</xref>]</td><td align="center" rowspan="1" colspan="1">2008</td><td align="center" rowspan="1" colspan="1">56 (M)</td><td align="center" rowspan="1" colspan="1">Hypertension, cigarette smoking, and bilateral inguinal hernia repair status post laparoscopic surgery</td><td align="center" rowspan="1" colspan="1">Two week history of fever up to 103°F, chills, myalgia, and 10‐pound weight loss</td><td align="center" rowspan="1" colspan="1">Immunocompetent</td><td align="center" rowspan="1" colspan="1">Rupture</td><td align="center" rowspan="1" colspan="1">Microti</td><td align="center" rowspan="1" colspan="1">Not reported</td><td align="center" rowspan="1" colspan="1">Lyme disease</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1">Splenectomy + medical management</td></tr><tr><td align="left" rowspan="1" colspan="1">3.</td><td align="center" rowspan="1" colspan="1">Kuwayama and Briones. [<xref>16</xref>]</td><td align="center" rowspan="1" colspan="1">2008</td><td align="center" rowspan="1" colspan="1">61 (M)</td><td align="center" rowspan="1" colspan="1">None</td><td align="center" rowspan="1" colspan="1">Fever, chills, headache, and malaise</td><td align="center" rowspan="1" colspan="1">Immunocompetent</td><td align="center" rowspan="1" colspan="1">Rupture</td><td align="center" rowspan="1" colspan="1">Microti</td><td align="center" rowspan="1" colspan="1">5%</td><td align="center" rowspan="1" colspan="1">Not reported</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1">Splenectomy + medical management</td></tr><tr><td align="left" rowspan="1" colspan="1">4.</td><td align="center" rowspan="1" colspan="1">Florescu et al. [<xref>5</xref>]</td><td align="center" rowspan="1" colspan="1">2008</td><td align="center" rowspan="1" colspan="1">58 (M)</td><td align="center" rowspan="1" colspan="1">malaria in childhood</td><td align="center" rowspan="1" colspan="1">Fever, chills, myalgias, and left upper quadrant pain</td><td align="center" rowspan="1" colspan="1">Immunocompetent</td><td align="center" rowspan="1" colspan="1">Infarction</td><td align="center" rowspan="1" colspan="1">Microti</td><td align="center" rowspan="1" colspan="1">0.5%</td><td align="center" rowspan="1" colspan="1">Anaplasmosis</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1">Medical management</td></tr><tr><td align="left" rowspan="1" colspan="1">5.</td><td align="center" rowspan="1" colspan="1">Florescu et al. [<xref>5</xref>]</td><td align="center" rowspan="1" colspan="1">2008</td><td align="center" rowspan="1" colspan="1">75 (F)</td><td align="center" rowspan="1" colspan="1">Colon cancer status postcompletion of chemotherapy 5 years prior and hypertension</td><td align="center" rowspan="1" colspan="1">Fever, night sweats, and fatigue</td><td align="center" rowspan="1" colspan="1">Immunocompetent but a history of being immunocompromised</td><td align="center" rowspan="1" colspan="1">Infarction</td><td align="center" rowspan="1" colspan="1">unknown</td><td align="center" rowspan="1" colspan="1">< 1%</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1"> <bold>Yes, the patient was initially being worked up for malignancy as initial smears were negative. Treatment started 25 days after presentation. Course was complicated by aspiration pneumonia, sepsis multiorgan failure, and death.</bold> </td><td align="center" rowspan="1" colspan="1">Patient demised despite medical management</td></tr><tr><td align="left" rowspan="1" colspan="1">6.</td><td align="center" rowspan="1" colspan="1">El Khoury et al. [<xref>10</xref>]</td><td align="center" rowspan="1" colspan="1">2011</td><td align="center" rowspan="1" colspan="1">36 (M)</td><td align="center" rowspan="1" colspan="1">None</td><td align="center" rowspan="1" colspan="1">Left upper quadrant pain and 2 weeks of fever and chills</td><td align="center" rowspan="1" colspan="1">Immunocompetent</td><td align="center" rowspan="1" colspan="1">Infarction</td><td align="center" rowspan="1" colspan="1">Microti</td><td align="center" rowspan="1" colspan="1">3%–4%</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1">Medical management</td></tr><tr><td align="left" rowspan="1" colspan="1">7.</td><td align="center" rowspan="1" colspan="1">El Khoury et al. [<xref>10</xref>]</td><td align="center" rowspan="1" colspan="1">2011</td><td align="center" rowspan="1" colspan="1">70 (M)</td><td align="center" rowspan="1" colspan="1">Lyme disease 10 years prior</td><td align="center" rowspan="1" colspan="1">A 4 day history of malaise, fatigue, fevers, chills, and diffuse abdominal pain</td><td align="center" rowspan="1" colspan="1">Immunocompetent</td><td align="center" rowspan="1" colspan="1">Rupture</td><td align="center" rowspan="1" colspan="1">Microti</td><td align="center" rowspan="1" colspan="1">2%</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1">Splenectomy + medical management</td></tr><tr><td align="left" rowspan="1" colspan="1">8.</td><td align="center" rowspan="1" colspan="1">Reis et al. [<xref>11</xref>]</td><td align="center" rowspan="1" colspan="1">2011</td><td align="center" rowspan="1" colspan="1">70 (M)</td><td align="center" rowspan="1" colspan="1">Not reported</td><td align="center" rowspan="1" colspan="1">Three day history of fever, nausea, and vomiting, and sudden onset of abdominal pain</td><td align="center" rowspan="1" colspan="1">Not reported</td><td align="center" rowspan="1" colspan="1">Rupture</td><td align="center" rowspan="1" colspan="1">Microti</td><td align="center" rowspan="1" colspan="1">Not reported</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1"> </td><td align="center" rowspan="1" colspan="1">Selective splenic artery embolization</td></tr><tr><td align="left" rowspan="1" colspan="1">9.</td><td align="center" rowspan="1" colspan="1">Abbas et al. [<xref>14</xref>]</td><td align="center" rowspan="1" colspan="1">2011</td><td align="center" rowspan="1" colspan="1">23 (M)</td><td align="center" rowspan="1" colspan="1">None</td><td align="center" rowspan="1" colspan="1">Fever, chills, weight loss, malaise</td><td align="center" rowspan="1" colspan="1">Immunocompetent</td><td align="center" rowspan="1" colspan="1">Rupture</td><td align="center" rowspan="1" colspan="1">Microti</td><td align="center" rowspan="1" colspan="1">30%</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1"> <bold>Yes</bold> </td><td align="center" rowspan="1" colspan="1">Splenectomy + medical management</td></tr><tr><td align="left" rowspan="1" colspan="1">10.</td><td align="center" rowspan="1" colspan="1">Tobler et al. [<xref>17</xref>]</td><td align="center" rowspan="1" colspan="1">2011</td><td align="center" rowspan="1" colspan="1">54 (M)</td><td align="center" rowspan="1" colspan="1">Lyme disease</td><td align="center" rowspan="1" colspan="1">Left upper quadrant abdominal pain, fever of 102.3 °F, nausea, chills, night sweats, and dark urine</td><td align="center" rowspan="1" colspan="1">Immunocompetent</td><td align="center" rowspan="1" colspan="1">Rupture</td><td align="center" rowspan="1" colspan="1">Microti</td><td align="center" rowspan="1" colspan="1">3%</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1">Splenectomy + medical Management</td></tr><tr><td align="left" rowspan="1" colspan="1">11.</td><td align="center" rowspan="1" colspan="1">Usatii et al. [<xref>12</xref>]</td><td align="center" rowspan="1" colspan="1">2014</td><td align="center" rowspan="1" colspan="1">54 (M)</td><td align="center" rowspan="1" colspan="1">None</td><td align="center" rowspan="1" colspan="1">Left upper quadrant abdominal pain for 1 week along with abdominal distention and subjective fevers and headache</td><td align="center" rowspan="1" colspan="1">Immunocompetent</td><td align="center" rowspan="1" colspan="1">Rupture</td><td align="center" rowspan="1" colspan="1">Microti</td><td align="center" rowspan="1" colspan="1">Not reported</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1"> <bold>Yes</bold> </td><td align="center" rowspan="1" colspan="1">Splenectomy + medical management</td></tr><tr><td align="left" rowspan="1" colspan="1">12.</td><td align="center" rowspan="1" colspan="1">Farber et al. [<xref>9</xref>]</td><td align="center" rowspan="1" colspan="1">2015</td><td align="center" rowspan="1" colspan="1">59 (F)</td><td align="center" rowspan="1" colspan="1">CAD, hyperlipidemia, and depression</td><td align="center" rowspan="1" colspan="1">A syncopal episode after 2 weeks of headaches, fatigue, chills, abdominal pain, nausea, and diarrhea</td><td align="center" rowspan="1" colspan="1">Immunocompetent</td><td align="center" rowspan="1" colspan="1">Rupture</td><td align="center" rowspan="1" colspan="1">Microti</td><td align="center" rowspan="1" colspan="1">0.9%</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1">Splenectomy + medical management</td></tr><tr><td align="left" rowspan="1" colspan="1">13.</td><td align="center" rowspan="1" colspan="1">Al Zoubi et al. [<xref>18</xref>]</td><td align="center" rowspan="1" colspan="1">2016</td><td align="center" rowspan="1" colspan="1">72 (M)</td><td align="center" rowspan="1" colspan="1">Hypertension</td><td align="center" rowspan="1" colspan="1">Fever, chills, weight loss, and abdominal pain</td><td align="center" rowspan="1" colspan="1">Immunocompetent</td><td align="center" rowspan="1" colspan="1">Infarction</td><td align="center" rowspan="1" colspan="1">Microti</td><td align="center" rowspan="1" colspan="1">0.5%</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1"> <bold>Yes</bold> </td><td align="center" rowspan="1" colspan="1">Medical management</td></tr><tr><td align="left" rowspan="1" colspan="1">14.</td><td align="center" rowspan="1" colspan="1">Dumic et al. [<xref>6</xref>]</td><td align="center" rowspan="1" colspan="1">2018</td><td align="center" rowspan="1" colspan="1">79 (F)</td><td align="center" rowspan="1" colspan="1">Hypertension, coronary artery disease, and atrial fibrillation on warfarin</td><td align="center" rowspan="1" colspan="1">Left‐sided chest pain, extreme fatigue, and dizziness without any fever but she represented on postop day 10 with fevers and abdominal pain.</td><td align="center" rowspan="1" colspan="1">Immunocompetent</td><td align="center" rowspan="1" colspan="1">Rupture</td><td align="center" rowspan="1" colspan="1">Microti</td><td align="center" rowspan="1" colspan="1">1.6%</td><td align="center" rowspan="1" colspan="1">Lyme</td><td align="center" rowspan="1" colspan="1"> <bold>Yes: she presented without fever with splenic pathology, discharged, and represented with fever and then found to have babesiosis as the cause of her splenic injury.</bold> </td><td align="center" rowspan="1" colspan="1">Splenectomy + medical management</td></tr><tr><td align="left" rowspan="1" colspan="1">15.</td><td align="center" rowspan="1" colspan="1">Blackwood et al. [<xref>7</xref>]</td><td align="center" rowspan="1" colspan="1">2018</td><td align="center" rowspan="1" colspan="1">51 (M)</td><td align="center" rowspan="1" colspan="1">Hypertension and atrial fibrillations</td><td align="center" rowspan="1" colspan="1">Syncope after a 5 day history of fever, chills, rigors, sweats, and general malaise with worsening abdominal pain</td><td align="center" rowspan="1" colspan="1">Immunocompetent</td><td align="center" rowspan="1" colspan="1">Rupture</td><td align="center" rowspan="1" colspan="1">Microti</td><td align="center" rowspan="1" colspan="1">0.9%</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1">Splenectomy + medical management</td></tr><tr><td align="left" rowspan="1" colspan="1">16.</td><td align="center" rowspan="1" colspan="1">Blackwood and Binder [<xref>7</xref>]</td><td align="center" rowspan="1" colspan="1">2018</td><td align="center" rowspan="1" colspan="1">61 (M)</td><td align="center" rowspan="1" colspan="1">Hypertension and hyperlipidemia</td><td align="center" rowspan="1" colspan="1">Abdominal pain and 3 days of fever, chills, myalgias, weakness, and decreased appetite.</td><td align="center" rowspan="1" colspan="1">Immunocompetent</td><td align="center" rowspan="1" colspan="1">Infarction</td><td align="center" rowspan="1" colspan="1">Microti</td><td align="center" rowspan="1" colspan="1">0.44%</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1">Medical management</td></tr><tr><td align="left" rowspan="1" colspan="1">17.</td><td align="center" rowspan="1" colspan="1">Gupta et al. [<xref>4</xref>]</td><td align="center" rowspan="1" colspan="1">2019</td><td align="center" rowspan="1" colspan="1">53 (M)</td><td align="center" rowspan="1" colspan="1">Tobacco use and cholecystitis status postcholecystectomy</td><td align="center" rowspan="1" colspan="1">Fatigue, fever, and abdominal pain</td><td align="center" rowspan="1" colspan="1">Immunocompetent</td><td align="center" rowspan="1" colspan="1">Infarction</td><td align="center" rowspan="1" colspan="1">Microti</td><td align="center" rowspan="1" colspan="1">1.5%</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1">Medical management</td></tr><tr><td align="left" rowspan="1" colspan="1">18.</td><td align="center" rowspan="1" colspan="1">Sung et al. [<xref>3</xref>]</td><td align="center" rowspan="1" colspan="1">2021</td><td align="center" rowspan="1" colspan="1">46 (M)</td><td align="center" rowspan="1" colspan="1">None</td><td align="center" rowspan="1" colspan="1">Abdominal pain</td><td align="center" rowspan="1" colspan="1">Immunocompetent</td><td align="center" rowspan="1" colspan="1">Rupture</td><td align="center" rowspan="1" colspan="1">Microti</td><td align="center" rowspan="1" colspan="1">0.1%</td><td align="center" rowspan="1" colspan="1">Lyme disease</td><td align="center" rowspan="1" colspan="1">No</td><td align="center" rowspan="1" colspan="1">Splenectomy + medical management</td></tr><tr><td align="left" rowspan="1" colspan="1">19.</td><td align="center" rowspan="1" colspan="1">Sung et al. [<xref>3</xref>]</td><td align="center" rowspan="1" colspan="1">2021</td><td align="center" rowspan="1" colspan="1">51 (M)</td><td align="center" rowspan="1" colspan="1">Obesity status postgastric bypass surgery</td><td align="center" rowspan="1" colspan="1">Fever and left‐sided abdominal pain</td><td align="center" rowspan="1" colspan="1">Immunocompetent</td><td align="center" rowspan="1" colspan="1">Infarction</td><td align="center" rowspan="1" colspan="1">Microti</td><td align="center" rowspan="1" colspan="1">0.6%</td><td align="center" rowspan="1" colspan="1">Lyme disease</td><td align="center" rowspan="1" colspan="1"> <bold>Yes: Initial CT scan was unrevealing, and patient was discharged. He then returned with new hepatosplenomegaly, hemolytic anemia, acute splenic infarction.</bold> </td><td align="center" rowspan="1" colspan="1">Medical management</td></tr><tr><td align="left" rowspan="1" colspan="1">20.</td><td align="center" rowspan="1" colspan="1">Mateja et al. [<xref>13</xref>]</td><td align="center" rowspan="1" colspan="1">2024</td><td align="center" rowspan="1" colspan="1">70 (M)</td><td align="center" rowspan="1" colspan="1">Hypertension, hyperlipidemia, BPH, asthma, gastroesophageal reflux disease, depression, anxiety, and schizoaffective disorder</td><td align="center" rowspan="1" colspan="1">Bilateral flank pain, sweating, nausea, and chills for 3 days. He reported having three syncopal episodes on the day of the presentation.</td><td align="center" rowspan="1" colspan="1">Immunocompetent</td><td align="center" rowspan="1" colspan="1">Rupture</td><td align="center" rowspan="1" colspan="1">Microti</td><td align="center" rowspan="1" colspan="1">13%</td><td align="center" rowspan="1" colspan="1">Not reported</td><td align="center" rowspan="1" colspan="1"> <bold>Yes, he had splenectomy, then was discharged. Returned after developing fever on POD 17. Pathology notified primary team of babesia seen on examination of spleen. He required plasmapheresis</bold> </td><td align="center" rowspan="1" colspan="1">Splenectomy + medical management</td></tr></tbody></table>In contrast, our patient was an immunocompetent male in his late 20s with low‐level parasitemia (1.4%) with associated splenic infarction and severe hemolytic anemia, both known serious complications of babesiosis. Hence, we present a notable case of the youngest immunocompetent patient with babesia‐associated splenic injury in the setting of low parasitemia levels (< 4%). Our findings challenge the prevailing belief that severe presentations of babesiosis typically occur in patients over 50, those with severe parasitemia (> 10%), or in immunocompromised individuals, thus adding a unique perspective to the existing literature.
Our patient had no hemoglobinopathies, which could have accounted for his profound hemolysis despite a low parasitemia. He also did not have any history or findings of atrial fibrillation, nor was he taking any prothrombotic medications, which could have otherwise explained his splenic infarctions. A common risk factor in other cases is coinfection with Borrelia burgdorferi. Coinfection with Borrelia burgdorferi or Anaplasma phagocytophilum can increase disease severity and duration [1–4]. Table 3 shows that 5 of 20 cases were associated with other tick‐borne illnesses: 3 with Lyme disease, 1 with Anaplasmosis, and 1 with Ehrlichiosis. Although coinfection may lead to increased severity, many reported cases without coinfection have low parasitemia in immunocompetent patients, suggesting that babesiosis alone can cause spontaneous splenic injury. Thus, babesiosis should not be ruled out as a potential cause of splenic injury, even in the absence of other tick‐borne illnesses.
3.3. Pathophysiology of Babesia‐Associated Splenic Injury
The exact mechanism of splenic infarction remains an intriguing enigma. However, a study by Akel et al. [20] demonstrated that inoculating hamsters with Babesia led to microthrombi formation in the spleen’s small vessels, resulting in coagulative necrosis. Infected erythrocytes triggered an acute proinflammatory cytokine release, activating the coagulation system and increasing erythrocyte adhesion. This sequence of events obstructed flow and caused congestion in the splenic sinusoids [20]. As seen in malaria, infected RBCs cannot deform and thus further obstruct splenic sinusoids [2, 20]. Obstruction can lead to infarction in the affected area. Splenic macrophages also attempt to phagocytose infected RBCs trapped in splenic venules, leading to additional congestion and platelet sequestration, which can result in splenomegaly and potentially, splenic infarction or rupture [2, 21]. Dumic et al. [2] support this theory by describing findings of red pulp hyperplasia, diffuse hypercellularity, massive proliferation of plasma cells, and remarkable intrasinusoidal histiocytes in the ruptured spleens of patients infected by Plasmodium vivax.
Table 3 indicates that babesia‐associated splenic injury can occur independent of age, sex, immune status, comorbidities, or degree of parasitemia. However, splenic injuries are more likely in cases where there was a delay in presentation/treatment after the onset of symptoms. The finding that 53% of those cases (see Table 3 and Dumic et al. [2]) where babesiosis was initially missed resulted in worse outcomes further supports this theory. This likely stems from prolonged exposure to a heightened proinflammatory state as described by Akel et al. [20].
In the case of our patient, another factor that may have contributed to his condition was the fall he experienced before presentation. He found the tick before the fall, but it is unclear how long it had been attached before it was first noticed. One may argue that, in the same way that infectious mononucleosis makes the spleen more susceptible to damage upon impact, the same may be true in babesiosis. Hence, the fall and impact on an already compromised spleen from subclinical babesiosis at that point could have been another factor that contributed to the development of his splenic infarcts.
3.4. Importance of Early Diagnosis and How Delays can Affect Clinical Outcomes
Timely diagnosis is pivotal in decreasing disease‐related morbidity and mortality. Of the 38 known cases (including our case) of babesia‐associated splenic injury, 19 (50%) were initially missed. 10 out of the 19 cases (53%) had poor outcomes (death or required splenectomy/splenic artery embolization). 2 out of those 10 cases resulted in death, while 8 required splenectomy or splenic artery embolization. The remaining 9 cases were successfully treated with medical management, like our patient. Of those 9 cases, the patients either had no comorbidities or only hypertension. Dumic et al. [6] and Mateja et al. [13] described patients with splenic rupture who required emergency surgery and were discharged, only to return later with postoperative fever, eventually diagnosed with babesiosis as the cause of their splenic rupture.
Our patient initially presented with abdominal pain and splenic infarcts at an outside hospital, where he was discharged afebrile and stable. He later represented with fever, anemia, and more extensive splenic infarcts. This case underscores the necessity of maintaining a high suspicion for babesiosis in patients with atraumatic splenic injury or splenic injury out of proportion to the level of trauma, living in or who have recently traveled to endemic regions. Taking a detailed history of tick exposure and insect bites in endemic areas is crucial to prevent delays in diagnosis and treatment, which can lead to worse outcomes.
3.5. Treatment Pearls
Atovaquone and azithromycin treatment is as effective as clindamycin and quinine, with fewer adverse reactions [23]. In a randomized trial by Krause et al. [23], adverse reactions occurred in 15% of patients treated with atovaquone and azithromycin, compared to 72% for those given quinine and clindamycin.
Resistance to atovaquone–azithromycin has been observed in severely immunocompromised patients, limiting its use [24]. Additionally, due to insufficient data on atovaquone–azithromycin efficacy in immunocompromised hosts with severe babesiosis, quinine, and clindamycin are recommended in such cases [23]. For patients with high‐grade parasitemia > 10% (regardless of the clinical presentation), severe anemia (< 10 g/dL), or significant complications (with any level of parasitemia), RBC exchange is used alongside drug therapy [1, 2, 23].
Consent
No written consent has been obtained from the patient, as there are no patient‐identifiable data included in this case report.
Conflicts of Interest
The authors declare no conflicts of interest.
Funding
No funding was received for this manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vannier E. G. , Diuk-Wasser M. A. , Ben Mamoun C. , and Krause P. J. , Babesiosis, Infectious Disease Clinics of North America. (June 2015) 29, no. 2, 357–370, 10.1016/j.idc.2015.02.008, 2-s 2.0-84929617132.25999229 PMC 4458703 · doi ↗ · pubmed ↗
- 2Dumic I. , Madrid C. , Rueda Prada L. , Nordstrom C. W. , Taweesedt P. T. , and Ramanan P. , Splenic Complications of Babesia Microti Infection in Humans: A Systematic Review, The Canadian Journal of Infectious Diseases & Medical Microbiology. (May 2020) 27, 6934149–8, 10.1155/2020/6934149.PMC 727521732566058 · doi ↗ · pubmed ↗
- 3Sung L. H. , Sundaram A. H. , Glick A. L. , Chen D. F. , and Shipton L. , Babesiosis as a Cause of Atraumatic Splenic Injury: Two Case Reports and a Review of Literature, Journal of General Internal Medicine. (December 2021) 36, no. 12, 3869–3874, 10.1007/s 11606-021-07117-5.34549355 PMC 8455114 · doi ↗ · pubmed ↗
- 4Gupta A. , Patel P. , Manvar K. , Kellner T. , and Guevara E. , Splenic Infarction in Babesiosis: A Rare Presentation, Clinical Case Reports. (July 2019) 7, no. 8, 1591–1595, 10.1002/ccr 3.2301, 2-s 2.0-85070608275.31428398 PMC 6692990 · doi ↗ · pubmed ↗
- 5Florescu D. , Sordillo P. P. , Glyptis A. et al., Splenic Infarction in Human Babesiosis: Two Cases and Discussion, Clinical Infectious Diseases. (January 2008) 46, no. 1, e 8–e 11, 10.1086/524081, 2-s 2.0-39349110575.18171204 · doi ↗ · pubmed ↗
- 6Dumic I. , Patel J. , Hart M. , Niendorf E. R. , Martin S. , and Ramanan P. , Splenic Rupture as the First Manifestation of Babesia Microti Infection: Report of a Case and Review of Literature, American Journal of Case Reports. (March 2018) 19, 335–341, 10.12659/ajcr.908453, 2-s 2.0-85044728406.29567936 PMC 5878539 · doi ↗ · pubmed ↗
- 7Blackwood B. and Binder W. , Unusual Complications From Babesia Infection: Splenic Infarction and Splenic Rupture in Two Separate Patients, Journal of Emergency Medicine. (November 2018) 55, no. 5, e 113–e 117, 10.1016/j.jemermed.2018.08.004, 2-s 2.0-85053839063.30253953 · doi ↗ · pubmed ↗
- 8Nikolic D. , Mc Pherson R. A. , Pincus M. R. et al., Spirochete Infections: Treponemal Diseases, Leptospira, Borrelia and Agents of Intestinal Spirochetosis, Henry’s Clinical Diagnosis and Management by Laboratory Methods, 2022, 24th edition, Elsevier, 1229–1245.