The clinical impact of herpesvirus testing on multiplex PCR panels in a pediatric population
Caitlin Naureckas Li, Cecilia Thompson, Brittany Hunter, Elizabeth Dobler, Natalie Jachym, Emaan Mohsin, Marcelo Malakooti, Lisa Akhtar

TL;DR
This study examines how testing for herpesviruses in a pediatric PCR panel for meningitis/encephalitis affects clinical outcomes.
Contribution
The study provides insights into the clinical utility of including herpesvirus targets in a meningitis/encephalitis PCR panel for children.
Findings
Herpesvirus detection led to changes in clinical management in a subset of pediatric patients.
The inclusion of herpesvirus targets in the PCR panel had diagnostic and therapeutic implications.
Abstract
The use of multiplex polymerase chain reaction (PCR) panels for diagnosis of clinical syndromes is rapidly growing despite limited data on optimal use cases. We retrospectively reviewed the clinical impact and consequences of the inclusion of herpesvirus targets on the meningitis/encephalitis PCR panel.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
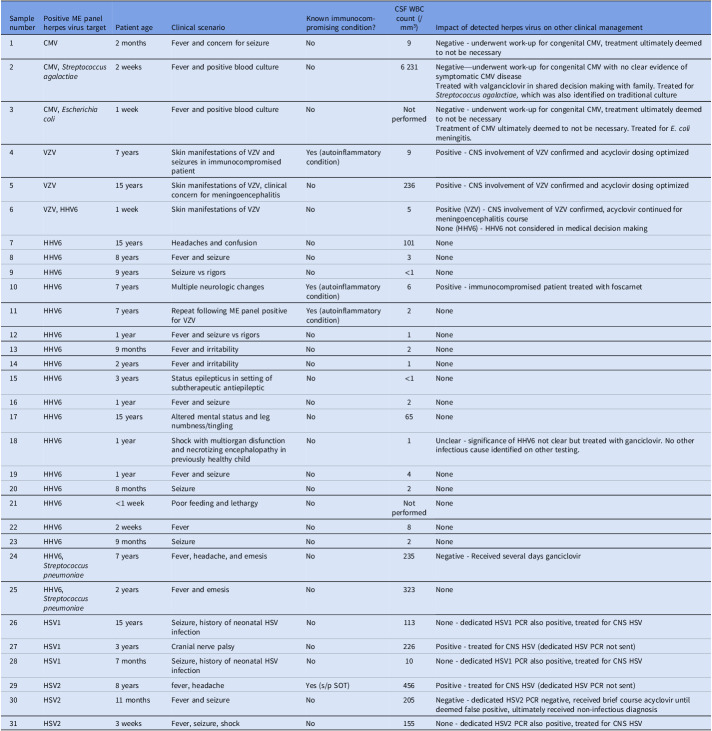 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHerpesvirus Infections and Treatments · Cytomegalovirus and herpesvirus research · Bacterial Infections and Vaccines
Introduction
A variety of multiplex molecular panels are now commercially available to detect a defined set of organisms associated with a clinical syndrome such as meningitis/encephalitis (ME), gastroenteritis, or pneumonia.^ 1 ^ However, these panels often include targets that may not be clinically significant in every patient. Detected organisms may represent normal flora, colonizing organisms, or reactivation of latent viruses in the setting of another underlying illness, particularly in immunocompetent patients.^ 2 ^ Positive result interpretation can be challenging, and clinicians may be hesitant to dismiss a positive result.
The multiplex polymerase chain reaction (PCR) ME panel from BioFire (BioMérieux, Salt Lake City, UT) received U.S. Food and Drug Administration clearance in 2015 and contains 14 bacterial, viral, and fungal targets.^ 3 ^ Reported positive predictive values (PPVs) vary widely but have been reported to be as low as 37%.^ 4,5 ^ Concerns around PPVs are particularly significant in children, where the epidemiology of meningitis differs from adult counterparts; for example, pediatric cryptococcosis is significantly more rare than the same disease in adults.^ 6,7 ^ Additionally, the clinical spectrum of meningitis and encephalitis is broad, with limited overlap in presentation between pathogens included on the panel. Given this, we sought to understand the clinical impact and describe potential benefits and harms associated with detection of herpesviruses on the ME panel at our institution.
Methods
This work took place at our freestanding Midwestern children’s hospital. At our site, an ME panel is typically ordered upfront, without restrictions, any time a sample is collected by lumbar puncture for infectious indications regardless of clinical presentation. Clinicians are encouraged to send a dedicated herpes simplex virus (HSV) PCR as the first line test when this diagnosis is suspected given concerns regarding lower ME panel sensitivity compared to targeted PCR.^ 8 ^
We retrospectively reviewed ME panel results from January 2019-January 2025 positive for any virus in the Herpesviridae family (cytomegalovirus [CMV], HSV1, HSV2, human herpesvirus 6 [HHV6], and varicella zoster virus [VZV]). Two infectious diseases attendings (CNL, LA) evaluated clinical significance of results based on documentation by the primary team. We applied descriptive statistics as appropriate. This work was deemed exempt from full review by our local institutional review board.
Results
1,598 ME panels were performed during the study period from 1,449 individual patients. Thirty-one panels were positive for a total of 32 herpesviruses: 20 HHV6, and 3 each CMV, HSV1, HSV2, and VZV. Five panels were positive for more than one organism: one with two herpesviruses and the remainder with a herpesvirus and a bacterium. Of the 32 positive herpesvirus ME panel results, six (19%) results were determined to have a positive impact on management, five (16%) a negative impact, one (3%) an unclear impact, and 20 (63%) no impact (Table 1). Half of panels with a positive impact on patients (3/6) served as confirmation of central nervous system (CNS) involvement, specifically in patients with known varicella. Two of the remaining three panels with a positive impact were in immunocompromised patients. All positive VZV results resulted in a positive change of management, and all positive CMV results resulted in unnecessary interventions.
Table 1.Clinical details of positive testsSample numberPositive ME panel herpes virus targetPatient ageClinical scenarioKnown immunocompromising condition?CSF WBC count (/mm^3^)Impact of detected herpes virus on other clinical management1CMV2 monthsFever and concern for seizureNo9Negative - underwent work-up for congenital CMV, treatment ultimately deemed to not be necessary2CMV, Streptococcus agalactiae 2 weeksFever and positive blood cultureNo6 231Negative—underwent work-up for congenital CMV with no clear evidence of symptomatic CMV diseaseTreated with valganciclovir in shared decision making with family. Treated for Streptococcus agalactiae, which was also identified on traditional culture3CMV, Escherichia coli 1 weekFever and positive blood cultureNoNot performedNegative - underwent work-up for congenital CMV, treatment ultimately deemed to not be necessaryTreatment of CMV ultimately deemed to not be necessary. Treated for E. coli meningitis.4VZV7 yearsSkin manifestations of VZV and seizures in immunocompromised patientYes (autoinflammatory condition)9Positive - CNS involvement of VZV confirmed and acyclovir dosing optimized5VZV15 yearsSkin manifestations of VZV, clinicalconcern for meningoencephalitisNo236Positive - CNS involvement of VZV confirmed and acyclovir dosing optimized6VZV, HHV61 weekSkin manifestations of VZVNo5Positive (VZV) - CNS involvement of VZV confirmed, acyclovir continued for meningoencephalitis courseNone (HHV6) - HHV6 not considered in medical decision making7HHV615 yearsHeadaches and confusionNo101None8HHV68 yearsFever and seizureNo3None9HHV69 yearsSeizure vs rigorsNo<1None10HHV67 yearsMultiple neurologic changesYes (autoinflammatory condition)6Positive - immunocompromised patient treated with foscarnet11HHV67 yearsRepeat following ME panel positivefor VZVYes (autoinflammatory condition)2None12HHV61 yearFever and seizure vs rigorsNo1None13HHV69 monthsFever and irritabilityNo2None14HHV62 yearsFever and irritabilityNo1None15HHV63 yearsStatus epilepticus in setting ofsubtherapeutic antiepilepticNo<1None16HHV61 yearFever and seizureNo2None17HHV615 yearsAltered mental status and legnumbness/tinglingNo65None18HHV61 yearShock with multiorgan disfunctionand necrotizing encephalopathy inpreviously healthy childNo1Unclear - significance of HHV6 not clear but treated with ganciclovir. No other infectious cause identified on other testing.19HHV61 yearFever and seizureNo4None20HHV68 monthsSeizureNo2None21HHV6<1 weekPoor feeding and lethargyNoNot performedNone22HHV62 weeksFeverNo8None23HHV69 monthsSeizureNo2None24HHV6, Streptococcus pneumoniae 7 yearsFever, headache, and emesisNo235Negative - Received several days ganciclovir25HHV6, Streptococcus pneumoniae 2 yearsFever and emesisNo323None26HSV115 yearsSeizure, history of neonatal HSV infectionNo113None - dedicated HSV1 PCR also positive, treated for CNS HSV27HSV13 yearsCranial nerve palsyNo226Positive - treated for CNS HSV (dedicated HSV PCR not sent)28HSV17 monthsSeizure, history of neonatal HSV infectionNo10None - dedicated HSV1 PCR also positive, treated for CNS HSV29HSV28 yearsfever, headacheYes (s/p SOT)456Positive - treated for CNS HSV (dedicated HSV PCR not sent)30HSV211 monthsFever and seizureNo205Negative - dedicated HSV2 PCR negative, received brief course acyclovir until deemed false positive, ultimately received non-infectious diagnosis31HSV23 weeksFever, seizure, shockNo155None - dedicated HSV2 PCR also positive, treated for CNS HSVA positive herpes virus result was determined to have had a positive impact if there was consensus among the providers involved in the patient’s care that it represented a true infection and allowed for addition of targeted therapy, determination of the need to continue therapy that had been started empirically, or discontinuation of a therapy that had been started empirically. It was determined to have a negative impact if there was ultimately consensus from providers involved in the patient’s care that it did not explain the symptoms for which a lumbar puncture was performed but additional medications were given or tests performed because of the positive test. It was characterized as unclear impact if there was not ultimately consensus about the significance of the result among the providers who saw the patient. There was considered to be no impact if the test result did not change clinical management or the diagnosis had been made by another test sent at the same time.N.B. Samples 4/10/11 and 8/9 were from the same patients at different time pointsCMV,cytomegalovirus; E. coli,Escherichia coli; HHV6,human herpes virus 6; CNS,central nervous system; HSV,herpes simplex virus; PCR,polymerase chain reaction; SOT,solid organ transplant; VZV,varicella zoster virus.
Discussion
We found that at our institution, management of immunocompetent children rarely changed when herpesviruses were detected on the ME panel. The widespread commercial availability of molecular tests has led to significant variation in utilization when optimal use case scenarios are not well defined.^ 9–11 ^ Our ME panel findings highlight the potential consequences of test overuse outlined by the Society for Healthcare Epidemiology of America: overdiagnosis of organisms not causing true disease, possible misdiagnosis if providers anchor on a positive result from this test, and excess cost burdens on the healthcare system.^ 12 ^
This work does have multiple limitations. Significantly, we did not evaluate the impact of negative tests or the psychological impact of positive tests that did not change clinical management. Given the retrospective nature of this study, we were unable to reach definitive conclusions about the impact of positive herpesvirus results on antimicrobial management. This study was not designed to evaluate the test performance characteristics of the ME panel, and our use of impact on clinical management as our main outcome does introduce the possibility of bias into the interpretation of the test impact. However, this measure still has value as it reflects the real-world impact of the test. Our findings are also likely less generalizable to other sites with strong stewardship strategies in place for this test, however the impact of a false positive result remains.
At our site, de-implementation of ME panels represent a significant opportunity for diagnostic stewardship,^ 13 ^ and we are actively pursuing quality improvement work to do so. We urge other sites with unrestricted use of multiplex panels to similarly consider potential downsides of this broad testing approach and seek out opportunities to optimize use of multiplex panel testing.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lewinski MA , Alby K , Babady NE , et al. Exploring the utility of multiplex infectious disease panel testing for diagnosis of infection in different body sites: a joint report of the association for molecular pathology, American society for microbiology, infectious diseases society of America, And Pan American Society For Clinical Virology. J Mol Diagn JMD 2023;25:857–875. doi:10.1016/j.jmoldx.2023.08.005.37757952 PMC 11702286 · doi ↗ · pubmed ↗
- 2Green DA , Pereira M , Miko B , Radmard S , Whittier S , Thakur K. Clinical significance of human Herpesvirus 6 Positivity on the Film Array Meningitis/Encephalitis panel. Clin Infect Dis 2018;67:1125– 1128. doi:10.1093/cid/ciy 288.29635334 PMC 7108106 · doi ↗ · pubmed ↗
- 3Bio Fire Diagnostics receives a de novo clearance by the FDA for the Film Array® Meningitis/Encephalitis panel continuing its extremely favorable business momentum. bio Mérieux Website. https://www.biomerieux.com/corp/en/journalists/press-releases/biofire-diagnostics-receives-de-novo-clearance-fda-filmarrayr-meningitisencephalitis-panel.html. Accessed October 29, 2025.
- 4Fleischer E , Aronson PL. Rapid diagnostic tests for Meningitis and Encephalitis - Biofire®. Pediatr Emerg Care 2020;36:397– 401. doi:10.1097/PEC.0000000000002180.32740268 PMC 7703746 · doi ↗ · pubmed ↗
- 5Myint T , Soria J , Gao Y , Conejo Castillo MR , Arora V , Ribes JA. Comparison of positive Bio Fire Film Array meningitis/encephalitis (ME) panels, CSF cultures, CSF parameters, clinical presentation and in-patient mortality among patients with bacterial and fungal meningitis. Microbiol Spectr 2024;13:e 00014– e 00024. doi: 10.1128/spectrum.00014-24.39714177 PMC 11792450 · doi ↗ · pubmed ↗
- 6Sáez-Llorens, X , Mc Cracken, GH. Bacterial meningitis in children. The Lancet 2003;361:2139– 2148. doi:10.1016/S 0140-6736(03)13693-8.12826449 · doi ↗ · pubmed ↗
- 7Meiring ST , Quan VC , Cohen C , et al. A comparison of cases of paediatric-onset and adult-onset cryptococcosis detected through population-based surveillance, 2005-2007. AIDS Lond Engl 2012;26:2307– 2314. doi:10.1097/QAD.0b 013e 3283570567.22739390 · doi ↗ · pubmed ↗
- 8Gaensbauer J , Fernholz E , Hiskey L , Binnicker M , Corsini Campioli C. Comparison of two assays to diagnose herpes simplex virus in patients with central nervous system infections. J Clin Virol 2023;166:105528. doi:10.1016/j.jcv.2023.105528.37390620 · doi ↗ · pubmed ↗