Correlation study of fatty pancreas and fatty liver CT manifestations with biochemical parameters in middle-aged and young adult cholecystectomy patients
Yi Zhou, Chao He, Haipeng Zhang

TL;DR
This study found that cholecystectomy is linked to higher rates of fatty pancreas, especially compared to fatty liver, in middle-aged and young adults.
Contribution
The study identifies a significant association between cholecystectomy and increased pancreatic steatosis.
Findings
Cholecystectomy patients had higher rates of pancreatic and hepatic steatosis compared to controls.
Pancreatic steatosis was significantly associated with cholecystectomy, but not hepatic steatosis.
Post-cholecystectomy patients should be monitored for pancreatic steatosis to enable early intervention.
Abstract
To investigate the correlation between the occurrence of pancreatic steatosis, hepatic steatosis, and cholecystectomy, as well as the associated biochemical parameters. A retrospective analysis was conducted on 409 patients who underwent abdominal CT scans between November 2022 and March 2024. Among them, 127 patients had undergone cholecystectomy (experimental group), while 282 had not (control group). The incidence rates of pancreatic steatosis and hepatic steatosis were compared between the two groups, along with relevant biochemical parameters including total cholesterol, triglycerides, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, and fasting blood glucose levels. The incidence of pancreatic steatosis in the experimental group was 67.8%, and the incidence of hepatic steatosis was 22%. In the control group, the incidence rates were 54.3% for pancreatic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
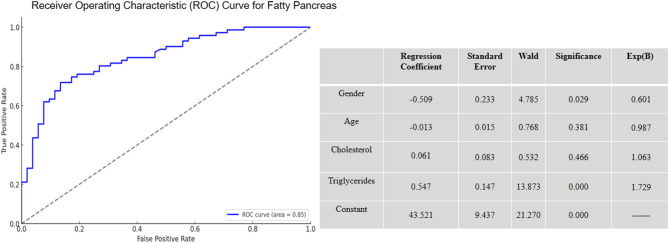 Figure 1
Figure 1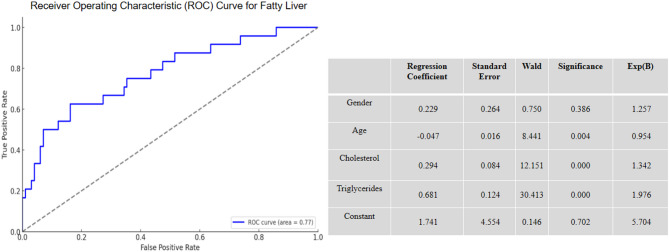 Figure 2
Figure 2- —the Health Research Fund Project of Shaanxi Province
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatitis Pathology and Treatment · Liver Disease Diagnosis and Treatment · Cardiovascular Function and Risk Factors
Introduction
In recent years, with continuous advancements in imaging techniques, research on pancreatic steatosis has garnered increasing attention [1]. Existing studies have found that pancreatic steatosis is closely associated with disorders of glucose metabolism, acute and chronic pancreatitis, and pancreatic malignancies. In routine clinical practice, it is often observed that patients who undergo cholecystectomy exhibit signs of pancreatic steatosis and hepatic steatosis in follow-up abdominal CT scans [2]. However, studies exploring the relationship between cholecystectomy, the incidence of pancreatic and hepatic steatosis, and their associated biochemical parameters are relatively sparse. This study aims to investigate the incidence of pancreatic and hepatic steatosis following cholecystectomy and their correlation with biochemical parameters [3–5].
Cholecystectomy, a common surgical procedure, is widely used to treat various gallbladder-related diseases [6]. Despite its significant efficacy in resolving gallbladder issues, cholecystectomy may lead to a series of metabolic problems, particularly the development of pancreatic and hepatic steatosis [7]. Post-cholecystectomy, bile flows directly from the liver into the intestines, potentially altering bile composition and subsequently affecting the normal metabolism of fats and sugars in the body. Furthermore, research indicates that the occurrence of pancreatic steatosis is often accompanied by hepatic steatosis, with a significant correlation between the two conditions [8–11].
To further elucidate the relationship between cholecystectomy, pancreatic steatosis, and hepatic steatosis, this study retrospectively analyzed clinical data from 409 patients who underwent abdominal CT scans at our hospital between November 2022 and March 2024. This cohort included 127 patients who had undergone cholecystectomy and 282 patients who had not. By comparing the incidence rates of pancreatic and hepatic steatosis and the associated biochemical parameters between these two groups, we aim to provide a basis for the early detection, diagnosis, and treatment of fat deposition post-cholecystectomy. The results of this study will contribute to a better understanding of the mechanisms behind the occurrence of pancreatic and hepatic steatosis following cholecystectomy and provide valuable insights for clinicians, thereby improving the management and prognosis of postoperative patients.
Methods
Study population
A retrospective study was conducted, including 409 patients who were hospitalized and underwent abdominal CT scans at our hospital between November 2022 and March 2024. Among these, 127 patients who had undergone cholecystectomy were assigned to the experimental group, while 282 patients who had not undergone cholecystectomy were designated as the control group. All patients were aged between 20 and 60 years. Informed consent was obtained from all participants.
Inclusion criteria
- Complete case data and laboratory tests.
- Underwent abdominal CT examination during hospitalization.
Exclusion criteria
- Chronic heavy alcohol consumption (ethanol intake ≥ 40 g/day for males and ≥ 20 g/day for females).
- History of drug-induced liver injury.
- Hepatitis virus infection.
- History of pancreatitis.
- Liver or pancreatic tumors.
Examination methods
- CT Scanning: Patients fasted for 10 h before undergoing an abdominal CT scan using a Toshiba Aquilion 64-slice CT scanner. The scanning range extended from the diaphragm to the lower edge of the liver, with a tube voltage of 120 kV, a slice thickness of 7 mm, a slice interval of 7 mm, a window width of 200 HU, and a window level of 40 HU. CT images were jointly reviewed by one attending physician and one associate chief physician to observe the size and morphology of the pancreas and liver, and to measure the CT values of the pancreas, liver, and spleen.
- Diagnostic Criteria: A normal pancreas on CT appears with clear and smooth borders, homogeneous parenchymal density, and a CT value approximately equal to that of the spleen, slightly higher than the kidneys. Pancreatic steatosis on CT manifests as reduced pancreatic volume, uneven edges, decreased parenchymal density, with punctate or patchy hypodense areas, and a pancreatic CT value lower than that of the spleen, comparable to that of the kidneys. A normal liver has a density higher than the spleen. In hepatic steatosis, the liver density is homogeneous or heterogeneous, lower than that of the spleen.
Blood tests
After fasting for 12 h, blood samples were collected from both groups of patients for laboratory tests. The biochemical tests and their normal ranges are as follows:
- Triglycerides (0.56 ~ 1.69 mmol/L).
- Total cholesterol (2.33 ~ 5.69 mmol/L).
- Glucose (3.89–6.11 mmol/L).
- Apolipoprotein A1 (1.00 ~ 1.60 g/L).
- Apolipoprotein B (0.60 ~ 1.10 g/L).
- High-density lipoprotein (1.05–1.91 mmol/L).
- Low-density lipoprotein (1.81–3.36 mmol/L).
Statistical analysis
Data analysis was performed using SPSS statistical software. The t-test was used for comparisons between groups, and the χ² test was used for comparison of proportions. A p-value of < 0.05 was considered statistically significant. Binary logistic regression analysis was conducted with significant factors as independent variables and pancreatic steatosis and hepatic steatosis as dependent variables to analyze the associated risk factors.
Results
Incidence rates and CT value analysis
In this study, 127 patients who underwent cholecystectomy were included in the experimental group (Table 1). The mean pancreas-to-spleen CT value difference was − 8.81 ± 10.47, the pancreas/spleen CT value ratio was 0.81 ± 0.23, the pancreatic CT value was 38.68 ± 11.63, and the splenic CT value was 47.48 ± 4.16. The CT scan results showed that the incidence of pancreatic steatosis in the experimental group was 67.8% (86 cases), hepatic steatosis was 22% (28 cases), and the concurrent incidence of pancreatic and hepatic steatosis was 20.5% (26 cases). In the control group, which included 282 patients who had not undergone cholecystectomy, the mean pancreas-to-spleen CT value difference was − 8.38 ± 10.20, the pancreas/spleen CT value ratio was 0.83 ± 0.21, the pancreatic CT value was 39.92 ± 10.77, and the splenic CT value was 48.31 ± 4.05. In this group, the incidence of pancreatic steatosis was 54.7% (153 cases), hepatic steatosis was 15.6% (44 cases), and the concurrent incidence of pancreatic and hepatic steatosis was 12.7% (36 cases). The results indicate that the incidence rates of both pancreatic and hepatic steatosis are significantly higher post-cholecystectomy, with the incidence of pancreatic steatosis being notably higher than that of hepatic steatosis. As shown in Table 2, there is no significant correlation between cholecystectomy and hepatic steatosis. However, there is a significant correlation between cholecystectomy and pancreatic steatosis, suggesting an increased likelihood of developing pancreatic steatosis in patients who have undergone cholecystectomy.
Table 1. Analysis of general dataGroupSample SizeMale/FemaleAge (years)Pancreas-Spleen CT ValuePancreas/Spleen CT RatioPancreas CT ValueSpleen CT ValueControl Group283137/14649.85 ± 8.24−8.38 ± 10.200.83 ± 0.2139.92 ± 10.7748.31 ± 4.05Experimental Group12842/8653.50 ± 6.63−8.81 ± 10.470.81 ± 0.2338.68 ± 11.6347.48 ± 4.16
Table 2. Correlation between cholecystectomy and the incidence of pancreatic steatosis and hepatic steatosisCorrelation AnalysisChi-square ValueP-valueSignificanceCholecystectomy and Fatty Liver2.9110.233Not SignificantCholecystectomy and Fatty Pancreas6.9910.030Significant
As shown in Table 3, the experimental group demonstrated statistically significant differences in age, gender, total cholesterol, and triglycerides compared to the control group (p < 0.05). However, there were no significant differences between the experimental group and the control group in fasting blood glucose, high-density lipoprotein, low-density lipoprotein, pancreas-to-spleen CT value difference, and pancreas/spleen CT value ratio (p > 0.05).
Table 3. Comparison of biochemical parameters between experimental and control groupsParameterLevene’s Test for Equality of Variances (F)Significance (P-value)t-test for Equality of Means (t)Degrees of FreedomSignificance (Two-tailed)Mean DifferenceStandard Error Difference95% Confidence Interval of the Difference (Lower)95% Confidence Interval of the Difference (Upper)Total Cholesterol0.0770.7823.52553400.4010.1130.1770.624Triglycerides4.4170.0362.135340.0340.2520.1180.0190.483Blood Glucose1.6730.196−1.8415340.066−0.2220.120−0.4580.014High-Density Lipoprotein (HDL)0.1330.7160.0495340.9610.0020.031−0.0590.0623Low-Density Lipoprotein (LDL)0.9480.331−0.5665340.572−0.0360.064−0.1630.090Gender35.55603.68253400.1550.04210.0720.238Pancreas-Spleen CT Value1.4780.225−0.3844070.701−0.4211.098−2.5811.738Pancreas/Spleen CT Ratio1.9390.165−0.6264070.532−0.0140.023−0.0600.031
Regression analysis of risk factors for pancreatic steatosis
The development of pancreatic steatosis is the result of multiple factors, with gender and triglycerides being two important independent risk factors. Males are predisposed to abdominal fat accumulation, which not only increases the risk of fat infiltration in abdominal organs, including the pancreas, but also is associated with other metabolic syndromes [1]. As shown in Fig. 1, Logistic regression analysis revealed that the significant risk factors for pancreatic steatosis were gender and triglycerides, with regression coefficients of −0.509 and 0.547, respectively. Triglycerides showed the strongest correlation with pancreatic steatosis (OR = 1.729). Men have a relatively higher risk of developing pancreatic steatosis, which may be related to specific physiological characteristics in fat metabolism. Males typically accumulate more abdominal fat, which may increase the risk of fat infiltration in the pancreas. Triglycerides are a major lipid in the blood, commonly used for energy storage and transport. Elevated triglyceride levels can lead to excessive fat deposition in pancreatic tissue, resulting in pancreatic steatosis.
Fig. 1. Regression Analysis of Risk Factors for Pancreatic Steatosis
Correlation analysis of risk factors for hepatic steatosis
The development of hepatic steatosis is the result of multiple factors. Elevated levels of total cholesterol and triglycerides directly reflect abnormal lipid metabolism in the body and are key indicators of hepatic steatosis. As shown in Fig. 2, Logistic regression analysis identified age, total cholesterol, and triglycerides as significant risk factors for hepatic steatosis, with regression coefficients of −0.047, 0.294, and 0.681, respectively. Triglycerides had the strongest correlation with hepatic steatosis (OR = 1.976), followed by total cholesterol (OR = 1.342). The results indicate that age, total cholesterol, and triglycerides are the primary risk factors for hepatic steatosis.
Fig. 2. Correlation Analysis of Risk Factors for Hepatic Steatosis
Discussion
This study retrospectively analyzed the CT images and laboratory data of 127 patients who underwent cholecystectomy and 282 contemporaneous patients who did not, to investigate the correlation between cholecystectomy and the incidence of pancreatic steatosis and hepatic steatosis. The results revealed that the incidence rates of pancreatic steatosis and hepatic steatosis were significantly higher in the experimental group compared to the control group, suggesting that cholecystectomy may play a clinically significant role in the development of these conditions. In the experimental group, the incidence of pancreatic steatosis (67.8%) was notably higher than that of hepatic steatosis (22%), consistent with previous studies.
Pancreatic steatosis and hepatic steatosis are common metabolic disorders. Pancreatic steatosis refers to the abnormal deposition of fat cells within the pancreas, which can be caused by factors such as inflammation and mechanical obstruction of the pancreatic ducts, leading to the replacement of pancreatic parenchyma with fatty tissue [1, 2]. Hepatic steatosis involves the excessive accumulation of fat, primarily triglycerides, in the liver. Given that both the pancreas and liver originate from the endoderm during embryonic development, there is a similarity in the mechanisms of fat deposition in these two organs.Pancreatic steatosis typically presents without specific clinical symptoms in the majority of cases and is often discovered incidentally during physical examinations or imaging studies for other conditions. A small subset of patients with severe fat infiltration or concurrent complications may exhibit non-specific manifestations, including epigastric pain, bloating, or a sensation of fullness. These abdominal discomforts are generally mild and may worsen after meals. Accompanying symptoms such as decreased appetite, nausea, and belching may also occur, reflecting underlying digestive disturbances. In rare instances, impairment of pancreatic exocrine function can lead to fat malabsorption, characterized by greasy, foul-smelling stools that are difficult to flush.Similarly, the clinical presentation of hepatic steatosis (fatty liver disease) varies widely. Most patients are asymptomatic, with the condition frequently identified incidentally during imaging examinations. In patients with progressive disease or associated comorbidities, non-specific symptoms such as right upper quadrant pain, bloating, or dull discomfort may occur. These may be accompanied by fatigue, loss of appetite, nausea, and abdominal distension. Jaundice is an uncommon finding. It is important to note that symptom severity does not always correlate with the degree of hepatic fat infiltration.Our study demonstrated a significantly higher incidence of pancreatic steatosis in the experimental group, indicating that cholecystectomy may increase the risk of pancreatic steatosis [12]. Post-cholecystectomy, bile flows directly from the liver into the intestines, potentially altering bile composition and affecting fat and glucose metabolism, thus increasing fat deposition in the pancreas [13]. Therefore, close monitoring, early diagnosis, and intervention are essential for preventing and managing fatty pancreas and fatty liver in cholecystectomy patients, ultimately improving their postoperative quality of life and prognosis.
The correlation analysis of biochemical parameters showed significant differences in total cholesterol and triglyceride levels between the experimental and control groups (p < 0.05). The experimental group had higher levels of total cholesterol and triglycerides, which correlated with the increased incidence rates of pancreatic steatosis and hepatic steatosis. Logistic regression analysis identified triglycerides and gender as independent risk factors for pancreatic steatosis, with triglycerides having the strongest correlation (OR = 1.729). Additionally, total cholesterol and triglycerides were found to be major risk factors for hepatic steatosis, with triglycerides showing the strongest correlation (OR = 1.976).Therefore, it is of definite clinical value to incorporate lipid indicators such as triglycerides into the long-term monitoring system after cholecystect and as key targets for lifestyle intervention and drug therapy.
Cholecystectomy, the gold standard for treating gallbladder diseases, effectively resolves gallbladder-related issues but has raised concerns regarding the incidence of postoperative metabolic syndrome [14, 15]. The direct flow of bile into the intestines post-surgery may disrupt the normal metabolism of bile acids and bile salts, affecting fat and glucose metabolism. These metabolic disturbances may increase fat deposition in the pancreas and liver, leading to pancreatic steatosis and hepatic steatosis. Our study also showed a significantly higher incidence of these conditions in the experimental group, further confirming the presence of metabolic issues post-cholecystectomy. Therefore, close monitoring, early diagnosis, and intervention for pancreatic steatosis and hepatic steatosis are recommended for patients undergoing cholecystectomy to prevent disease progression [16].
This study has several limitations, such as the retrospective design, which does not establish causality, and the relatively small sample size, which may affect the generalizability of the results. Future studies should include larger sample sizes and longitudinal research to further explore the causal relationship between cholecystectomy and the development of pancreatic and hepatic steatosis.At the same time, abdominal ultrasound and MRI both completely avoided the risk of ionizing radiation of CT, and both of them had irreplaceable core advantages the resolution of abdominal soft tissue and the evaluation of organ function, and therefore could be used as the preferred way of daily active monitoring in people who need long-term monitoring after chocystectomy.
Conclusion
our study indicates that the incidence rates of pancreatic steatosis and hepatic steatosis significantly increase post-cholecystectomy, particularly pancreatic steatosis. Enhanced monitoring and management of these conditions in patients who have undergone cholecystectomy are essential to improve their quality of life and prognosis. Pancreatic steatosis and hepatic steatosis, as rapidly increasing clinical conditions, warrant significant attention. Particularly in patients undergoing abdominal CT scans post-cholecystectomy, careful observation for the presence of pancreatic and hepatic steatosis is crucial. Our research shows that the incidence of hepatic and pancreatic steatosis after cholecystectomy has increased, with pancreatic steatosis being particularly prominent. As a rapidly developing clinical condition, pancreatic and hepatic steatosis urgently need to be given. At the same time, traditional management after cholecystectomy mostly focuses on short-term surgical complications and symptom relief. The results of this study call for the extension clinical management to the long-term metabolic health level. It is necessary to strengthen the implementation of active monitoring, early diagnosis and comprehensive intervention strategies for patients after surgery, and through the of blood lipids, dietary adjustment, and strengthening exercise and other behavioral interventions, to prevent the occurrence and development of pancreatic and hepatic steatosis, and thus the long-term quality of life and overall prognosis of patients.