Integrated treatment utilizing both Chinese and Western medicine for refractory diabetic foot ulcers: a case report
Luyao Wang, Changting Sheng, Jiaxin Liu, Rong Chen, Rensong Yue, Maoyi Yang, Zhipeng Hu

TL;DR
A 57-year-old man with severe diabetic foot ulcers showed significant improvement using a combined Chinese and Western medicine treatment approach.
Contribution
Demonstrates the effectiveness of integrative treatment for advanced diabetic foot ulcers.
Findings
The ulcer showed near-complete closure after 144 days of integrative treatment.
HbA1c levels improved from 13.5% to 7.0%, indicating better metabolic control.
Functional recovery and full epithelialization were confirmed at follow-up.
Abstract
Diabetic foot ulcer (DFU) is a severe complication of diabetes associated with a high risk of amputation and long-term disability. We report the case of a 57-year-old man with a Wagner grade IV DFU whose condition continued to deteriorate despite two toe amputations. An integrative treatment strategy combining traditional Chinese medicine (TCM) and western medicine was subsequently employed and proved effective. The TCM regimen included oral decoctions and topical herbal applications, while the western medical approach encompassed targeted therapies including glycemic control, anti-infective therapy, circulatory enhancement, anticoagulation, neurotrophic support, and nutritional management. Over a 144-day course, the ulcer demonstrated near-complete closure at discharge, with full epithelialization and functional recovery confirmed at follow-up. HbA1c decreased from 13.5% to 7.0%,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1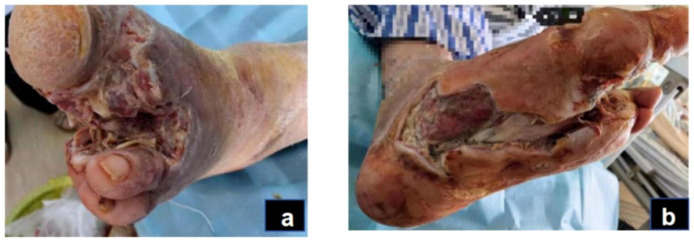 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5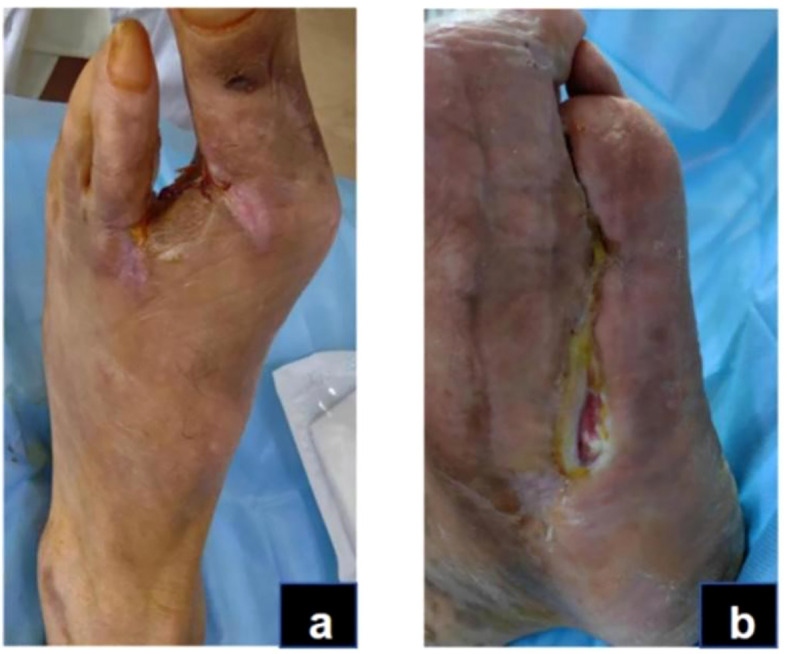 Figure 6
Figure 6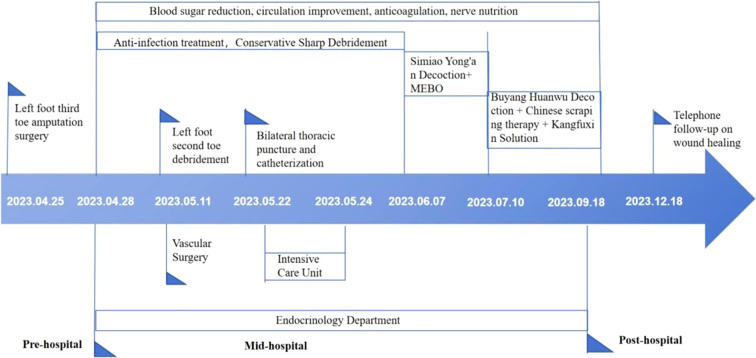 Figure 7
Figure 7| Laboratory examination results | Day 1 | Day 14 | Day 25 | Day 43 | Day 75 | Day 115 | Day 144 |
|---|---|---|---|---|---|---|---|
| White blood cell count (109/L) | 9.82 | 7.04 | 2.47 | 4.24 | 3.98 | 4.62 | 4.76 |
| Neutrophil counts(109/L) | 8.86 | 5.81 | 1.89 | 3.42 | 3.35 | 2.74 | 3.02 |
| Red blood cell count (109/L) | 3.11 | 2.86 | 2.64 | 3.45 | 4.48 | 4.57 | 4.62 |
| Hemoglobin(g/L) | 97 | 89 | 81 | 106 | 128 | 135 | 141 |
| C-reactive protein(mg/L) | 91.86 | 13.34 | 64.33 | 2.45 | 1.97 | 1.3 | 0 |
| K+(mmol/L) | 3.99 | 4.17 | 3.21 | 4.5 | 4.17 | 4.68 | 4.14 |
| Total Protein(g/L) | 52 | 55.4 | 51.7 | 60.6 | 63.1 | 66.4 | 68 |
| Albumin(g/L) | 28.3 | 31.1 | 29.4 | 35.3 | 38.1 | 40.2 | 41.9 |
| Creatinine(umol/L) | 55.1 | 59.5 | 50.9 | 59.5 | 62.6 | 67.4 | 62 |
| Uric Acid(umol/L) | 118 | 167 | 142 | 214 | 230 | 279 | 262 |
| HbA 1c(%) | 13.5 | – | – | – | – | 7 | – |
| fasting blood glucose (mmol/L) | 30.66 | 9.94 | 16.46 | 11.86 | 8.87 | 7.57 | 5.11 |
| Wound secretion culture | Candida parapsilosis,Enterococcus faecalis.Sensitive to gentamicin 120, ampicillin, ciprofloxacin, levofloxacin, linezolid, etc., and highly resistant to streptomycin, erythromycin, and tetracycline. | Candida albicans,Staphylococcus lugdunensis.Sensitive to amphotericin B, fluconazole, ciprofloxacin, clindamycin, gentamicin, levofloxacin, linezolid, etc., and resistant to oxacillin and penicillin. | Candida albicans is sensitive to amphotericin B, fluconazole, voriconazole, caspofungin, and micafungin. | no bacteria cultured | no bacteria cultured | no bacteria cultured | no bacteria cultured |
| Treatment | Measures | Usage and dosage |
|---|---|---|
| Blood sugar control | Metformin Hydrochloride Tablets;Insulin Glargine | 0.5g,oral administration,ter in die,1-144d;14 iu of insulin subcutaneous injection before bedtime,1-144d. |
| Anti-infection therapy | Latamoxef Sodium;Ornidazole;levofloxacin;Cefuroxime sodium;Piperacillin and Tazobactam | 1g, intravenous drip, quaque 12 hours,1-18d,28-42d;0.5g, intravenous drip,quaque 12 hours,1-24d;0.5g, intravenous drip,quaque die,18-24d;1.5g, intravenous drip, quaque 8 hours,25-26d;4.5g, intravenous drip, quaque 8 hours,26-27d. |
| Improve circulation | Alprostadil Injection | 20ug,intravenous drip,quaque die,1-144d. |
| Anticoagulation | Enoxaparin sodium Injection | 40mg,intravenous drip,quaque die,1-144d. |
| Nutrition of the nervous system | Thioctic Acid Injection | 0.6g,intravenous drip,quaque die,1-144d. |
| nutrition management | Human Albumin Injection | 10g,intravenous drip,quaque die,3-20d. |
| lower body temperature | Bupleurum Injection | 2ml,intramuscular injection,quaque die,15-20d. |
| potassium supplement | Potassium Chloride Sustained-release Tablets | 1g,oral administration,ter in die,15-25d. |
| Prescription | Composition | Main components | Medicinal efficacy | Pathways | References |
|---|---|---|---|---|---|
| Simiao Yong’an Decoction (SYD) | Radix Scrophulariae,Flos onicerae Japonicae, Radix Angelicae Sinensis, Radix et Rhizoma Glycyrrhizae | Chlorogenic acid, ferulic acid, caffeic acid, glycyrrhizin, cinnamic acid, quercetin, kaempferol and β-sitosterol | Clears heat and detoxifies, promotes blood circulation, unblocks channels | 1. Regulates MAPK and TNF pathways, promotes wound angiogenesis, reduces inflammatory response: reduces serum CRP and TNF-α levels, increases bFGF, EGF, and VEGF levels; downregulates TNF-α, IL-1β; increases MAPK, VEGF, IFN-γ levels. | ( |
| Moist exposed burn ointment (MEBO) | Rhizoma Coptidis,Radix Scutellariae, Cortex Phellodendri Chinensis,Pheretima,Pericarpium Papaveris | Quercetin, baicalein, wogonoside, palmitic acid methyl ester, and homogentisic acid | clear heat and detoxify, relieve pain, and promote tissue regeneration | 1. Inhibits the AGEs-RAGE/NF-κB signaling pathway: downregulates AGEs, RAGE mRNA, and NF-κB levels. | ( |
| Buyang Huanwu Decoction (BHD) | Radix Astragali, Radix Angelicae Sinensis, Radix Paeoniae Rubra, Flos Carthami, Semen Persicae, Rhizoma Chuanxiong and Pheretima | Astragaloside, formononetin glucoside, ferulic acid and paeoniflorin | tonifying Qi, promoting blood circulation, and unblocking channels | 1. Regulates the AGEs-RAGE pathway, inhibiting the inflammatory response: downregulates TNF-α and IL-6 expression, reduces the expression of AGEs, RAGE, ICAM-1, VCAM-1, MMP-2 proteins and mRNA. | ( |
| KangFuXin Solution (KFXS) | American cockroach | amino acids, nucleosides, and peptides | Promotes blood circulation, nourishes Yin, and promote tissue regeneration | 1. Regulates the AGEs-RAGE pathway:downregulates the expression of AGEs, RAGE, and HIF-1α proteins. | ( |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetic Foot Ulcer Assessment and Management · Wound Healing and Treatments · Peripheral Artery Disease Management
Introduction
According to the International Diabetes Federation (IDF) Diabetes Atlas, approximately 500 million adults globally currently suffer from diabetes mellitus (DM), and this number is expected to increase by 46% by 2045 (1). Diabetic foot ulcers (DFUs) are one of the most severe complications of DM, affecting 6.3% of patients (2), and a DM patient undergoes an amputation due to DFU every 20 seconds (3). DFUs significantly contribute to disability and infection-related mortality among DM patients. They often occur in the distal extremities and are commonly associated with neuropathy and peripheral vascular disease, leading to infections, ulcer formation, and/or deep tissue damage. Local tissue infection, peripheral neuropathy, and peripheral arterial disease are key risk factors influencing DFU onset (4–8).
Current clinical treatments involve systemic adjustments (such as blood sugar control, anti-infection measures, improved microcirculation, anticoagulation, and nerve nutrition) as well as wound management strategies (including debridement and repair techniques like skin grafting, stem cell therapy, and phototherapy) (9–17). In recent years, the Ilizarov method has also been employed to enhance local blood flow and promote ulcer healing in refractory DFU cases, particularly when conventional therapies fail (18–20). However, its application is often limited by technical complexity and patient tolerance, and managing high-grade DFUs complicated by comorbidities remains a major clinical challenge in achieving wound healing and limb preservation (21, 22).
TCM categorizes DFUs under gangrene and boasts a history of substantial clinical experience in treating these conditions. TCM treatments can be classified into internal and external therapies, renowned for their diverse approaches and effectiveness in promoting skin healing. TCM addresses deficiency (“xu”), stasis (“yu”), evil influences (“xie”), and decay (“fu”), offering targeted therapies to accelerate wound healing and reduce recurrence. Modern medical research has evidenced TCM’s significant efficacy in DFU treatment by exploring cells, proteins, molecules, and signaling pathways (23–27). This case report describes the successful treatment of a patient with a Wagner grade IV DFU and multiple comorbidities using an integrative regimen combining TCM and western medicine. To our knowledge, few detailed cases have documented complete healing of such advanced DFUs with integrative therapy, highlighting its potential value in complex diabetic wound management.
Case report
A 57-year-old male patient was admitted on April 28, 2023, with a five-year history of elevated blood sugar and a one-week history of a skin ulcer on the second toe and sole of his left foot. He was diagnosed with Type 2 diabetes five years ago, with a peak blood glucose level of 20 mmol/L, and began treatment with metformin, glimepiride, and gliclazide. However, he did not consistently monitor his blood sugar levels or adhere to his oral hypoglycemic medication regimen. One week prior to admission, he observed redness, swelling, numbness, and pain in his left foot, followed by ulceration on the second and third toes and the sole, emitting a pale yellow purulent discharge. The skin was dark and emitted a foul odor. He sought medical attention at Deyang People’s Hospital, where the third toe of his left foot was amputated. Post-operative care focused on infection control, boosting circulation, and debridement. A CT scan of the left foot indicated the absence of the third toe, slightly decreased bone density at the distal ends of the second to fourth metatarsals, and swelling in the surrounding soft tissues. Irregularities were noted at the proximal end of the left first metatarsal, likely due to degeneration or a previous injury. Three days ago, his wound ulcers worsened; the second toe became necrotic and black, with persistent pain, redness, and swelling, prompting treatment at our hospital. He reported numbness and pain in the left foot, dry mouth with excessive thirst, a bitter taste, frequent urination, twice-nightly nocturia, and sticky stools. Clinical examination revealed a yellow, greasy tongue coating, a dark red tongue body, and a slippery, rapid pulse.
Physical examination
The physical examination of the patient revealed a body temperature of 36.3°C, a pulse rate of 74 beats per minute, a respiratory rate of 20 breaths per minute, and blood pressure of 135/79 mmHg. The patient was conscious but displayed depressive symptoms. Cardiac, pulmonary, and abdominal assessments showed no significant abnormalities. Mild pitting edema was noted in both lower limbs, with non-palpable dorsal pedal and posterior tibial arteries bilaterally. The right foot had intact skin but a slightly reduced skin temperature. Conversely, the left foot presented with a lower skin temperature, absence of the third toe, and multiple ulcerations on the second toe and sole; the second toe appeared necrotic. The ulcerated area on the dorsum of the foot measured approximately 3 x 4 cm, while ulcerations on the sole reached up to 10 x 12 cm. The wound was red and discharged a white secretion with a foul odor (Figure 1).
Acute infection phase (Day 1): The red arrow indicates gangrene of the second toe of the left foot,and the black arrows show the necrotic boundary of the foot (A). The redness and swelling of the sole are obvious, and the boundary of necrosis is unclear (B).
Laboratory tests
Upon admission, the patient exhibited poor metabolic control (HbA1c 13.5%, fasting plasma glucose 30.66 mmol/L), systemic inflammation (CRP 91.86 mg/L, WBC 9.82 × 10^9^/L), and hypoproteinemia (albumin 28.3 g/L).The results of all laboratory examinations are summarized in Table 1. A bilateral lower limb vascular ultrasound revealed plaque formation in both common femoral arteries, varicose veins in the left great saphenous vein, a hypoechoic nodule in the left popliteal area, and enlarged lymph nodes in the left inguinal region. The chest and foot CT scans indicated several findings (1): pulmonary emphysema and pulmonary bullae in the upper lobes of both lungs, with slight interstitial changes and scattered small fibrous stripes (2); scattered small solid and ground-glass nodules in both lungs, considered low-risk, with an annual review recommended (3); slight coronary artery calcification (4); small amounts of pleural effusion on both sides (5); extensive bone absorption and destruction in the metatarsal and phalangeal bones of the left foot, most notably in the distal fourth metatarsal, with loss of joint structures, widespread swelling of the surrounding soft tissue accompanied by scattered air, and partial discontinuity of the skin, suggesting the possibility of a diabetic foot; clinical correlation is advised. The wound pathogen culture identified infections with Candida parapsilosis and Enterococcus faecium, which are sensitive to levofloxacin, gentamicin, ampicillin, ciprofloxacin, linezolid, and penicillin, but highly resistant to streptomycin, erythromycin, and tetracycline.
Admission diagnoses
- Type 2 diabetic foot disease; 2. Type 2 diabetes with multiple complications; 3. Lower limb skin infection; 4. Hypoproteinemia; 5. Protein-energy malnutrition; 6. Moderate anemia; 7. Emphysema.
Course of diagnosis and treatment
Given the patient’s severe infection, compromised baseline health, and significant clinical fluctuations, we implemented a staged treatment strategy.
Acute infection phase (days 1-42)
The acute infection phase was defined in this case as the period showing active local necrosis, purulent discharge, and elevated inflammatory markers (e.g., CRP >10 mg/L or WBC >9×10^9^/L), consistent with the clinical manifestations of moderate-to-severe diabetic foot infection as described in the IWGDF guidelines (28). Upon admission, the patient received symptomatic treatments including glucose control, anti-infection measures, circulation support, anticoagulation, neuro-nutrition, and nutritional management (Table 2).
Antimicrobial therapy was dynamically adjusted based on wound culture and drug-sensitivity results. Empiric broad-spectrum coverage with latamoxef sodium (Days 1–18) and ornidazole (Days 1–24) was initiated to control mixed aerobic–anaerobic infection. After Candida parapsilosis and Enterococcus faecalis (fluoroquinolone-sensitive) were identified on Day 1, the regimen was de-escalated to levofloxacin (Days 18–24) while continuing ornidazole. Later cultures on Days 14 and 25 revealed Candida albicans and Staphylococcus lugdunensis. When systemic deterioration and CRP elevation occurred on Day 25, therapy was temporarily escalated to cefuroxime sodium (Days 25–26) and piperacillin–tazobactam (Days 26–27) for broader Gram-positive and Gram-negative coverage. After stabilization and ICU discharge, the patient was stepped down to latamoxef sodium (Days 28–42) for consolidation. From Day 43 onward, serial cultures were negative, inflammatory markers normalized, and systemic antibiotics were discontinued. Candida species were regarded as surface colonizers; thus, no systemic antifungal therapy was required (Table 2).
For wound care, we disinfected the wound with iodine from the periphery to the center within a 15 cm diameter, followed by conservative sharp debridement of necrotic tissue and iodine with saline irrigation of the wound and sinus tract, then covered with sterile gauze. Dressing changes were conducted every morning. After local redness and swelling diminished, amputation of the second toe of the left foot, along with debridement, was performed on day 14 (Figure 2), followed by daily debridement and dressing changes post-surgery. The patient experienced recurrent fevers, peaking at 38.9°C, treated with cooling and potassium replacement therapy. On day 25, the patient suffered respiratory distress, with blood oxygen saturation under a mask oxygenation of only 82-89%. CT scans and bedside ultrasonography indicated significant bilateral pleural effusion, prompting an ICU transfer for further care, including bilateral thoracic puncture and catheter drainage. Pleural fluid analysis showed no significant abnormalities, and the drainage tubes were removed once vital signs stabilized on day 27, allowing the patient to return to our department. Concurrently, a nutritional consultation crafted a weekly diet plan aimed at providing 1.25-1.5 g/kg of high-quality protein per day, with additional supplements of 17–30 g of arginine, 0.57 g/kg of glutamine, and 70–90 mg of vitamin C, recommending short-term omega-3 fatty acid supplementation to enhance nutritional status. Laboratory examinations were conducted at clinically indicated milestones rather than predetermined intervals. During the acute infection period, tests were repeated when the patient’s condition fluctuated (e.g., fever, elevated CRP, or treatment adjustment). After Day 27, when vital signs and wound condition stabilized, laboratory testing frequency was reduced to once every two to three weeks until Day 43, in line with routine clinical practice for stable post-infectious patients.
Acute infection phase (day 14): After the patient underwent amputation of the second toe on the left foot (A). Debridement of plantar wound after amputation (B).
Wound healing period (days 43-144):inflammatory phase (days 43-75)
In this case, the inflammatory phase was characterized by local redness, swelling, necrotic wound edges, and purulent discharge, while systemic infection was largely controlled. These manifestations corresponded to the TCM pattern of Damp-Heat Toxin Syndrome (29, 30).The wound presented abundant exudation and malodor, accompanied by a greasy yellow tongue coating, dark-red tongue body, and slippery rapid pulse—features indicative of this syndrome (Figure 3). Treatment during this stage focused on clearing heat, resolving dampness, and detoxifying. A modified Simiao Yong’an Decoction (SYD) was prescribed (Radix Scrophulariae, 30g; Flos Lonicerae Japonicae, 30g; Radix Angelicae Sinensis, 20g; Radix et Rhizoma Glycyrrhizae, 10g; Rhizoma Coptidis, 20g; Radix Scutellariae, 20g; Cortex Phellodendri Chinensis, 20g; Fructus Gardeniae, 20g), boiled into a 400 ml decoction. The patient ingests 100 ml orally 30 minutes post-breakfast and dinner, each dose covering two days. For wound care, cleaning with saline-soaked gauze precedes the application of Moist exposed burn ointment (MEBO) (produced by Shantou Meibo Pharmaceutical Co., Ltd., National Drug Approval Number Z20000004) on the wound, spread 0.5 to 0.8 cm thick with a disposable tongue depressor, and bandaged with sterile gauze. Dressing changes are performed every morning. By day 75, foot swelling subsided, leaving minimal exudate, and surface necrotic tissue was entirely removed, advancing the wound from the inflammatory to the regenerative and remodeling phase.
Inflammatory phase (day 43): The swelling on the dorsum of the foot has subsided, but there is still a small amount of secretion (A). The dorsal foot wound has decreased in size, and the wound has shrunk (B).
Granulation and re-epithelialization phase (days 76-144)
In this case, the transition from the inflammatory to the remodeling phase was defined clinically when exudation and necrosis subsided, granulation tissue became dominant, and inflammatory markers such as CRP had already normalized. These criteria were based on the clinical features described in current wound-healing guidelines and literature (31, 32). During this stage, granulation tissue on both the sole and dorsum of the foot proliferated rapidly, filling the wound bases (Figure 4). Due to pathogenic impact, the patient exhibited significant Qi and blood depletion, fatigue, weakness, and a pale complexion with watery discharge, a pale red tongue, white coating, and a deep fine pulse, diagnosed as Qi and blood deficiency syndrome. Treatment involves supporting Qi, invigorating blood, and promoting muscle growth with Buyang Huanwu Decoction (BHD) (Radix Astragali, 20g; Radix Angelicae Sinensis, 15g; Radix Paeoniae Rubra, 15g; Flos Carthami, 15g; Semen Persicae, 15g; Rhizoma Chuanxiong, 15g; Pheretima, 10g). The administration mirrors prior methods. For wound care, cleaning with gauze soaked in KangFuXin Solution (KFXS) (manufactured by Sichuan Good Doctor Panxi Pharmaceutical Co., Ltd., National Drug Approval Number Z51021834) precedes KangFuXin-soaked gauze as an outer dressing, bandaged with sterile materials. Daily dressing changes occur in the morning. By day 115, the granulation tissue largely filled the sole wound. However, the wound size impeded epithelial migration, necessitating sole wound suturing (Figure 5) to expedite re-epithelialization. Post-surgery, the wound size reduced to 0.5 x 2.5 cm on the sole, and the dorsum wound fully healed (Figure 6). The patient requested discharge, advised to continue oral BHD and topical KFXS usage until complete wound healing. (Figure 7).
Granulation and re-epithelialization phase (Day 76): The granulation tissue on the dorsum and plantar of the foot grew well (A, B).
Granulation and re-epithelialization phase (Day 115): The dorsal and plantar wounds of the foot after wound closure of the plantar surface (A, B).
Granulation and re-epithelialization phase (Day 144): The dorsal foot wound healed completely (A). The area of the plantar wound was reduced to 0.52.5cm. (B).*
The timeline of the medication process of the patient.
Discussion
The wound healing process is typically divided into four continuous and overlapping stages: hemostasis, inflammation, proliferation, and remodeling. Upon completion of the repair process, scars form, resulting in wound healing. DFUs, a type of chronic and difficult-to-heal wound, are marked by persistent and excessive inflammatory responses. This significantly prolongs the transition from the inflammatory phase to the tissue proliferation phase, keeping the body in a state of elevated inflammation (33). The persistent inflammatory response induces the destruction of newly formed blood vessels and granulation tissue by metalloproteinases, leading to local wound edema and sustaining the inflammatory cascade, thereby affecting ulcer healing (34). Moreover, sustained hyperglycemia increases oxidative stress levels (35), downregulates growth factor receptors, and accelerates the degradation of growth factors (4), exacerbating ischemia, hypoxia, and nerve damage in diabetic wounds. In this case study, the patient presented with elevated blood glucose levels and was diagnosed with a moderate infection and medium-risk nutritional status according to the IWGDF/IDSA infection severity classification and COUNT score. The patient had a Wagner grade IV diabetic foot ulcer, accompanied by severe bone destruction, osteomyelitis, Gram-negative opportunistic pathogens, and mixed infections, indicative of a severe diabetic foot case with a poor prognosis, primarily leading to limb amputation. Consequently, we implemented systematic antimicrobial treatment, glycemic control, improved blood supply, nutritional support, and other symptomatic treatments. Resecting a single toe can significantly preserve the limb’s function with minimal impact on balance and gait (36). However, due to the low amputation level, the risk of proximal spreading of nerve and vascular lesions increases, resulting in new ulcers, infections, and non-healing wounds as postoperative complications (37). Postoperatively, the patient exhibited substantial redness, swelling, heat, and pain at the wound site, with purulent discharge along the wound edge. Cultures showed Candida albicans and Staphylococcus lugdunensis, indicating recurrent infection. The inflammatory response from foot infection and related complications can lead to high metabolic rates; infection-induced ulcer expansion or deepening worsens protein exudation, subsequently heightening the risk of malnutrition. Protein exudation reduces albumin levels, resulting in hypo-osmotic plasma, which can lead to pleural effusion, further compromising blood oxygen saturation and destabilizing vital signs. Guidance from the critical care department on antibiotic selection and pleural drainage, alongside nutritional prescriptions to correct hypoproteinemia and supplement albumin, helped the patient gradually stabilize, establishing a foundation conducive to wound healing.
TCM utilizes syndrome differentiation combined with internal and external treatments to address DFUs. This comprehensive approach enables a deeper understanding of the underlying causes and mechanisms, resulting in improved wound healing rates and symptom management (38–40). During the inflammatory phase, oral administration of the SYD and external application of MEBO are employed. The SYD contains multiple anti-inflammatory active ingredients, such as chlorogenic acid, ferulic acid, caffeic acid, glycyrrhizin, and cinnamic acid, which suppress inflammatory responses across various targets and pathways, forming the biological basis for the prescription’s anti-inflammatory properties (41–43). Additionally, it has effects on immune modulation, antioxidation, protection of vascular endothelium, regulation of angiogenesis, and improving insulin resistance, thereby facilitating diabetic foot wound healing (44–46).MEBO, an ointment preparation, interacts with necrotic tissues through hydrolysis and saponification upon adherence to the wound. It liquefies necrotic tissues, replaces surgical debridement, disrupts bacterial habitats, reduces bacterial activity, provides a moist environment for healing, and prevents bacterial invasion (47–49). Moreover, it contains amino acids, carbohydrates, and fatty acids which nourish the wound, promoting growth (50). For patients with extensive necrotic tissues and slow granulation growth, SYD and MEBO help regulate inflammation, reduce bacterial load, control infection, and transition the wound from inflammation to proliferation phase (Table 3). During the granuloma and re-epithelialization phase, BHD and Chinese scraping therapy combined with KFXS are used. BHD exhibits anti-inflammatory effects, inhibits secretion of inflammatory substances, prevents thromboxane synthesis, improves microcirculation, reduces inflammatory exudation, alleviates inflammation, promotes wound repair, and enhances VEGF expression, inducing neovascularization and improving hypoxia in wounds (51–56). KFXS, derived from Periplaneta americana extracts, up-regulates glutamine levels, stimulates protein synthesis, supporting cell proliferation, granulation growth, and angiogenesis, and enhances immune functions for rapid ulcer healing (57–60). Due to aged granulation tissue in this patient, Chinese scraping therapy was used to ensure drainage, remove aging tissue, and stimulate fresh growth (61). This approach accelerates granulation tissue and new blood vessel development, reduces wound size, promotes epithelial growth, and accelerates healing (Table 3). The treatment plan, involving Chinese medicine, vasodilators, and neurotrophic agents, improved symptoms, including numbness, pain, dry mouth, and fatigue. Follow-up calls after three months confirmed complete wound healing, allowing normal foot function and walking.
Although this case highlights the potential benefits of integrative Chinese and western medicine for diabetic foot ulcer management, its conclusions are inherently limited by the single-patient nature of a case report. Within the hierarchy of clinical evidence, such reports primarily serve as hypothesis-generating observations. Therefore, future prospective cohort or randomized controlled studies are warranted to provide higher-level evidence and verify the reproducibility of these integrative approaches.
Conclusion
This case report demonstrates that the integration of Chinese and western medicine in treating DFUs effectively controls disease progression, improves systemic symptoms, and promotes wound repair, suggesting it is a viable treatment strategy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sun H Saeedi P Karuranga S Pinkepank M Ogurtsova K Duncan BB. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. (2022) 183:109119. doi: 10.1016/j.diabres.2021.109119, PMID: 34879977 PMC 11057359 · doi ↗ · pubmed ↗
- 2Zhang P Lu J Jing Y Tang S Zhu D Bi Y. Global epidemiology of diabetic foot ulceration: a systematic review and meta-analysis. Ann Med. (2017) 49:106–16. doi: 10.1080/07853890.2016.1231932, PMID: 27585063 · doi ↗ · pubmed ↗
- 3Gu Y. Diagnosis and treatment of diabetic foot. Beijing: People’s Medical Publishing House (2016). p. 9.
- 4Patel S Srivastava S Singh MR Singh D. Mechanistic insight into diabetic wounds: Pathogenesis, molecular targets and treatment strategies to pace wound healing. Bio Med Pharmacother. (2019) 112:108615. doi: 10.1016/j.biopha.2019.108615, PMID: 30784919 · doi ↗ · pubmed ↗
- 5Brem H Tomic-Canic M. Cellular and molecular basis of wound healing in diabetes. J Clin Invest. (2007) 117:1219–22. doi: 10.1172/JCI 32169, PMID: 17476353 PMC 1857239 · doi ↗ · pubmed ↗
- 6Li Z Guo S Yao F Zhang Y Li T. Increased ratio of serum matrix metallo Protein-ase-9 against TIMP-1 predicts poor wound healing in diabetic foot ulcers. J Diabetes Complications. (2013) 27:380–2. doi: 10.1016/j.jdiacomp.2012.12.007, PMID: 23357650 · doi ↗ · pubmed ↗
- 7Basu Mallik S Jayashree BS Shenoy RR. Epigenetic modulation of macrophage polarization- perspectives in diabetic wounds. J Diabetes Complications. (2018) 32:524–30. doi: 10.1016/j.jdiacomp.2018.01.015, PMID: 29530315 · doi ↗ · pubmed ↗
- 8Singh K Agrawal NK Gupta SK. Decreased expression of heat shock proteins may lead to compromised wound healing in type 2 diabetes mellitus patients. J Diabetes Complications. (2015) 29:578–88. doi: 10.1016/j.jdiacomp.2015.01.007, PMID: 25746357 · doi ↗ · pubmed ↗