Strategies to improve healthcare team communication structure and quality in resource-variable childhood cancer hospitals (TeamTalk): a study protocol
Asya Agulnik, Dylan E. Graetz, Bobbi J. Carothers, Jocelyn Rivera, Erin Abu-Rish Blakeney, Samantha Hayes, Veronica L. Chaitan, Leopoldo Cabassa, Charles W. Goss, Douglas A. Luke, Sara Malone

TL;DR
This study aims to improve communication among healthcare teams caring for children with cancer, especially in hospitals with limited resources.
Contribution
The study co-develops and pilots a multilevel communication intervention tailored for resource-variable settings.
Findings
The study will identify modifiable determinants of communication quality using social network analysis and CritCom.
A multilevel intervention will be co-developed with clinicians and tested in eight hospitals.
The intervention's feasibility and preliminary efficacy will be evaluated in a cluster-randomized trial.
Abstract
Healthcare team communication is essential to high-quality childhood cancer care, especially during high-acuity events such as clinical deterioration and in resource-variable settings, where supportive interventions to resolve deterioration are less available. Communication quality has traditionally been understudied in these settings, and there is a notable lack of communication interventions that are appropriate and feasible in settings across resource levels. We propose addressing this challenge in this study protocol, which will co-develop and pilot a multi-level intervention to improve communication and outcomes for children receiving cancer treatment. This study leverages systems and implementation science methodologies to evaluate and improve communication quality in the care of hospitalized children with cancer. We will use a newly developed reliable and multilingual measure of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
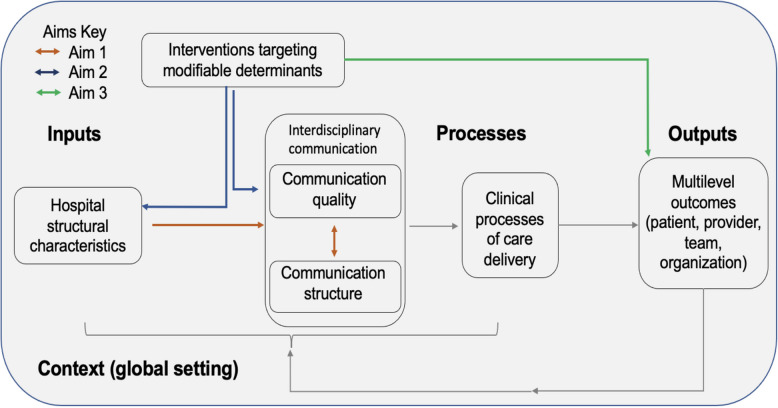 Figure 1
Figure 1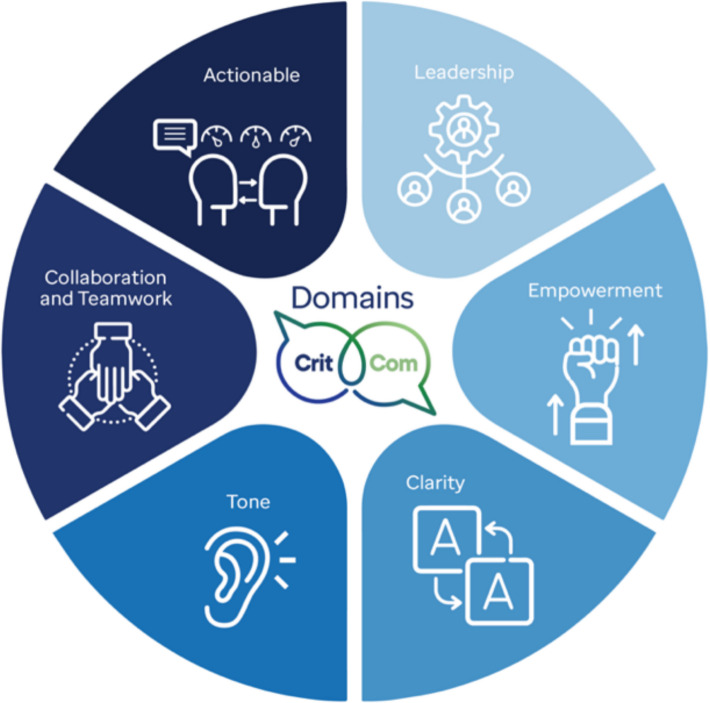 Figure 2
Figure 2- —http://dx.doi.org/10.13039/100000054National Cancer Institute
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChildhood Cancer Survivors' Quality of Life · Interprofessional Education and Collaboration · Patient-Provider Communication in Healthcare
Contributions to the literature
- This work will provide a foundational understanding of modifiable determinants of communication that impact healthcare delivery in resource-variable settings.
- We will develop and test an intervention to improve healthcare team communication, a field that currently lacks effective interventions.
- We will use social network analysis, a systems science method, to describe structural variation in communication and compare it to organizational communication quality.
- This study will address two notable barriers to team communication during patient deterioration: (1) lack of understanding of specific modifiable determinants of communication structure and quality and (2) lack of appropriate, feasible, and measurable communication interventions.
Background
To reduce global disparities in childhood cancer survival, the World Health Organization (WHO) Global Initiative for Childhood Cancer [1] and others [2] emphasize the need to improve childhood cancer treatment globally. Many hospitals providing childhood cancer care, however, face a range of resource limitations, including limited staff, supplies, and medications, challenging their ability to provide high-quality childhood cancer care and achieve this imperative [3]. A major barrier to childhood cancer survival, particularly in low-resource settings, is treatment-related mortality, or death during cancer treatment [4]. Clinical deterioration, defined as a decline in a patient’s clinical state that requires rapid identification and intervention, is a common cause of morbidity and mortality in children with cancer [5, 6]. Our prior work demonstrated a 30% mortality among pediatric oncology patients with deterioration in low-resource hospitals [7–13]. To date, however, there are limited effective interventions to improve outcomes for children with cancer who experience deterioration in resource-variable hospitals [14].
Optimal outcomes during clinical deterioration in children with cancer require excellent care coordination across multiple teams, necessitating high-quality team communication [15]. Over 70% of treatment delays, preventable harm, and death occur due to poor communication [16–23]. Prior studies have demonstrated that better communication leads to safer care, fewer medication errors [24], higher rates of rescue [25], and increased consistency in patient care across clinical teams [26]. High-quality communication between clinicians (e.g., physicians, nurses, pharmacists, respiratory therapy, etc.) directly impacts how teams utilize available resources and skills to identify and manage deterioration, thereby preventing mortality and improving health outcomes [27, 28]. Deterioration events, however, are highly stressful for clinical team members due to high patient acuity and time pressures, resulting in a risk of ineffective communication and lack of psychological safety, conceptualized as having a sense of safety in speaking up [16, 22]. Low-resource settings face additional communication challenges, including hierarchical systems, lower staff-to-patient ratios, and varying roles and responsibilities [29]. Addressing healthcare team communication, especially during acute events like clinical deterioration, offers a theoretically effective, low-cost intervention to improve childhood cancer outcomes across different settings. Previously studied interventions to improve pediatric oncology communication, however, focus on planned, controlled settings such as rounds or tumor boards and have been primarily developed and tested in high-resource settings [19, 30–33]. There is an urgent need for effective communication interventions to target complex systems and subsequently improve outcomes related to deterioration.
To improve communication in the care of children with cancer, we must identify modifiable factors that affect the quality of team communication [16, 21, 34, 35]. **“**Team communication” in this context must focus on the process of information exchange among the entire healthcare team, encompassing the quality of this exchange both between clinicians of different professions (physicians, nurses, respiratory therapist, social workers, etc.) and different disciplines(oncology, intensive care, surgery, etc.). However, there is a lack of a robust understanding of modifiable components of healthcare team communication structure and quality that can be targeted with interventions. Few effective interventions improve team communication and those that exist were primarily developed in high-resource settings [19, 30–33]. Low-resource settings are understudied [36], creating disparity between the high burden of childhood cancer mortality and poor understanding of communication determinants in these settings. This highlights a need for co-developed communication interventions appropriate for resource-diverse settings [37–39].
To address this knowledge gap, the TeamTalk study will develop and test a multilevel intervention that focuses on modifiable determinants of healthcare team communication structure and quality in global pediatric oncology hospitals, aiming to improve childhood cancer outcomes*.* To achieve this goal, we will 1) evaluate the relationship between team communication structure and quality in the care of children with cancer, 2) co-develop a multilevel intervention to improve communication quality in resource-variable hospitals, and 3) test the feasibility, acceptability, appropriateness, and preliminary efficacy of this intervention in resource-variable hospitals through a pilot cluster-randomized wait list control trial.
Methods and design
TeamTalk is an observational, formative study of team communication in resource-variable pediatric oncology hospitals, followed by intervention co-development and pilot testing (Table 1). We will engage members of the global oncology community to assess the relationship between team communication structure and quality (Aim 1) and use a mixed-method approach to co-develop and test an intervention to address these challenges across settings (Aims 2/3). Table 1. Overview of study aimsOverall Question: What are common modifiable determinants of healthcare team communication during deterioration and how might interventions target these determinants to improve outcomes for children with cancer in resource-variable settings?Aim 1: Communication structure and qualityQuestionsWhat is the relationship between structure and quality of team communication around deterioration in children with cancer?MethodCross sectional social network analysis from 10 high- and 10 low-quality communication hospitals selected from previous cross-sectional data (total n = 20)OutcomeEmpirical relationship between communication quality, communication structures, and provider and hospital level determinantsAim 2: Develop intervention to improve communicationQuestionWhat are potential multi-level interventions to address common modifiable challenges to communication quality across both high- and low- resource hospitals?Method(1) Sequential mixed methods study using quantitative data from Aim 1 supplemented by qualitative interviews with clinicians and (2) implementation mapping with global experts to co-develop an intervention to address common communication challengesOutcomeMulti-level intervention co-developed and selected for pilot testingAim 3: Pilot trial of communication interventionQuestionIs the identified intervention effective to improve communication quality and provider and patient outcomes while being perceived as feasible and acceptable by providers?MethodPilot identified multilevel intervention at 8 resource-variable hospitals using a wait list controlled, cluster randomized trialOutcomeIdentify feasibility, acceptability, appropriateness, and preliminary efficacy, of intervention to improve communication quality during deterioration
Conceptual framework
This study is informed by implementation science, health services research, and network communications theories, specifically the cancer Multiteam System (cMTS) framework (Fig. 1) [40, 41]. This conceptual framework illustrates how complex teams collaborate to deliver coordinated cancer care, highlighting the importance of effective communication structures and quality in care delivery. cMTS informs this study through its description of care processes and how teams are composed and organized, including team structure and hierarchy. Within the cMTS framework, communication is described as part of the processes of teamwork, while structure is an input. Care processes include both teamwork between and across teams as well as tasks that are accomplished through care delivery. These result in multilevel outcomes, including clinical patient outcomes, provider outcomes (burnout and job satisfaction), and unit/team outcomes (guideline adherence and efficiency of care) [40, 41].Fig. 1. Overview of conceptual framework for this research, focusing on assessing communication structure and quality within resource-variable settings. This is adapted from the cancer Multiteam System (cMTS) framework
Communication can be conceptually divided into two components: (1) quality of communication and (2) structure of communication [42, 43]. High-quality communication improves patient care, and we conceptualize this in alignment with the CritCom framework, a novel, reliable, multilingual measure of team communication quality comprised six domains (Fig. 2) [44, 45]. Less is known about how communication structurescan promote enhanced care, although examples of this include hierarchies, standard communication norms, and escalation protocols. For this study, we conceptualize communication structure as informed by network theory. Network communication theory describes the structures of communication to understand individual interactions, feedback, and behavior constraints among those involved within complex systems [46–48]. While network theory views each individual actor as following fairly simple rules or behaviors, complexity occurs when these simple behaviors multiply into a system of behaviors [49, 50]. Network communication theories point to network analysis as the appropriate methodology to understand communication structure in complex healthcare systems.Fig. 2. CritCom measure domains of quality team communication
Using these complementary frameworks, we posit that communication structure and quality interact to directly impact the quality of patient care. For example, lack of clarity and poor tone (communication quality) can impact clinician understanding of patient status and delay necessary intervention (care quality). Similarly, communication that must flow through a single lead physician has a high degree of hierarchy (communication structure), which can delay the flow of communication and necessary intervention, thus impacting patient outcomes. These interactions also impact providers, as poor communication experiences contribute to increased burnout and intentions to leave. This, in turn, further impacts patient outcomes, including safety events, mortality, and morbidity.
Our study aims (Table 1) are directly incorporated into this conceptual framework. Aim 1 focuses on the interrelationship between communication structure and quality to identify determinants of high-quality team communication. Aim 2 focuses on co-developing an appropriate multilevel intervention to target modifiable determinants of communication. Aim 3 tests the intervention’s feasibility and preliminary efficacy to improve team communication, and provider and patient outcomes in a pilot trial.
Setting
The proposed work will be conducted in collaboration with resource-variable pediatric oncology hospitals participating in the St. Jude Global Alliance [2], an international global health research and advocacy program that aims to strengthen care for children with cancer and other catastrophic diseases through innovative interventions, education, research, and team collaboration. Currently, the alliance has collaborators from more than 300 institutions in 77 countries. Over 110 St. Jude Global Alliance hospitals have completed the CritCom survey, and many others have participated in other large studies evaluating pediatric oncology care in resource-variable settings [51–56]. Hospitals with prior CritCom participation will be eligible sites for this study. While most hospitals are located in low- and middle-income countries, several are situated in World Bank-designated high-income countries. Aligned with our previous work, we will include hospitals self-identifying as having limitations in a broad range of resources, including inadequate nursing and physician staffing to identify and manage clinical deterioration events, limited Pediatric Intensive Care Unit space to accommodate children with cancer, and patients with low socioeconomic, educational, and nutritional indicators [3, 57–59]. These challenges result in an increased frequency of deterioration events with high mortality [12, 13], and their involvement enriches our study of communication across a range of resource limitations.
Study measures
Study measures (Table 2) align with our conceptual model, including measures of care inputs, team communication, care processes, and multilevel outcomes. Table 2. Overview of study measuresData DomainMeasuresData Collection MethodsCommunication qualityCritCom (6 domains, 30 questions)^a^- Individual survey, distributed confidentially and electronically through REDCap [60]- Distributed to all frontline clinical staff caring for children with cancer at risk of deterioration at each participating hospital- 3 weeks for data collection with weekly remindersIndividual demographics6 questions on role, unit worked, length of experience, sex, and hospital of employmentProvider outcomesQuestions about burnout, intent to leave, and job satisfactionHospital characteristicsHospital type, funding, bed capacity, pediatric oncology/critical care staffing, annual new diagnoses, and region- Collected and confirmed by local site leadCommunication structuresSocial network survey using a roster-based approach asking clinicians about overall communication patterns and changes during deterioration events^a^- Individual survey distributed confidentially through REDCap, 20–30 min. to complete- Distributed to all frontline clinical staff caring for children with cancer- 3 weeks for data collection with weekly remindersChallenges to communication and potential communication interventionsPerspectives of clinicians on communication challenges related to hospital and individual barriers, as well as potential interventions to improve team communication during care delivery- Semi structured interviews of frontline clinicians caring for children with cancer (physician, nurse, respiratory therapy, etc.)- Purposive sample for diversity including country income level, hospital size, professional role, etcIntervention feasibility, acceptability, and appropriatenessAfter intervention implementation, measures to assess how individual clinicians view the feasibility of intervention and their ratings of how appropriate and acceptable it is for them to receive the intervention in their setting- Individual survey, distributed confidentially through REDCap, 5 min. to complete- Distributed to all frontline clinical staff caring for children with cancer at 8 hospitals- 3 weeks per hospital for data collection, with weekly remindersPatient OutcomesClinical Deterioration Events (CDEs) [13] defined as an unplanned transfer to a higher level of care (i.e., ICU), use of an ICU intervention on the ward (vasoactive infusion, invasive or noninvasive mechanical ventilation, or cardiopulmonary resuscitation), or a ward death in a patient without limitations on resuscitation- Prospective de-identified registry of all CDEs in hospitalized pediatric oncology patients collected by the site team- For each CDE, a de-identified case report form is completed by local site leads and entered in REDCap database by a study team member- Data analysis checks for missing and incorrect values assure data quality- Pre and post intervention measurements^a^CritCom and the network survey will be collected concurrently during Aim 1, with CritCom collected alone during Aim 3
Social network survey
A social network survey will be conducted among 20 hospitals. These hospitals have previously completed CritCom and all provide pediatric cancer care. All critical care and ward clinicians caring for children with will be surveyed. Questions relate to communication patterns with all other clinicians sharing the same shift, communication during deterioration, role-based communication patterns, and other questions about the structure of team communication in their setting.
CritCom
CritCom is a novel, valid, reliable, and multilingual measure of team communication quality in the care of children with cancer experiencing deterioration [44, 45]. CritCom was designed for use by clinical healthcare teams across different hospital settings and resource levels. Our work will continue to provide construct validity for this pragmatic measure, advancing communication measurement in different linguistic settings, which is a major scientific barrier within the field. This work will shift approaches in how team communication quality can be measured in clinical settings, resulting in opportunities to assess and intervene on communication quality.
Hospital characteristics
For each participating hospital, we will conduct a hospital-level survey to assess organizational characteristics, such as hospital type, funding structure, size, annual number of new childhood cancer diagnoses, and other relevant variables.
Implementation outcomes
During Aim 3, we will conduct surveys of the clinical team members receiving the intervention to assess perceived feasibility, acceptability, and appropriateness of this intervention in their unit/team. We will use brief, validated measures of these constructs [61].
Expert panel
The research team will work closely with an expert panel of 20 members of the global pediatric oncology community with expertise in (1) clinical childhood cancer care in resource-variable settings, (2) healthcare team communication, and/or (3) health services delivery. The expert panel members will be specifically chosen to represent diverse geographic, contextual, and content expertise relevant to the care of children with cancer, inclusive of all WHO regions and country-income levels. This expert panel will meet quarterly, in English, to review study progress, provide feedback on findings and intervention development, participate in manuscript writing, and address any needs that arise throughout the grant period. This expert panel will also co-develop the communication intervention (Aim 2) and provide feedback throughout the pilot trial of the intervention (Aim 3).
Aim 1: Relationship between communication structure and qualit
We will use social network methods to assess the relationship between team communication structure and quality, and how communication structures vary among hospitals providing childhood cancer care.
Study setting and participants. From hospitals providing childhood cancer care that completed the communication quality assessment (CritCom) between March 2023—March 2025, 20 hospitals will be identified for eligibility. Hospitals will be selected using a modified positive and negative deviance approach, targeting 10 high- and 10 low-performing hospitals as defined through the cross-sectional assessment of communication quality (CritCom scores) [44, 45]. These hospitals will be recruited to obtain variability in CritCom score, with attention paid to the region of the hospital. After identification, the site lead from prior work will be contacted. Additional hospitals will be approached should the first 20 not agree to participate. Site leads will be responsible for obtaining hospital approval for participation and guiding local data collection. Each participating hospital will receive a report that includes hospital-level strengths and weaknesses.
Participant recruitment
Within each participating hospital, all clinicians who care for children with cancer at risk of deterioration will be eligible. A roster of all clinicians will be developed by site leads and revised with input by the study team, as is standard in network data collection. Individuals will be consented into this aim, and their participation will conclude at the end of the social network analysis and CritCom survey. Participation will be voluntary. We will provide incentives appropriate for each region for individuals who complete the assessment.
Data collection
Participants will be asked to complete a single survey containing the social network and CritCom questions. The social network survey inquires about communication patterns between individuals in routine care and how these patterns change when a patient is experiencing clinical deterioration. Participants will respond to questions including their communication contacts, and frequency of communication for both routine inpatient care and deterioration events. The CritCom assessment portion measures communication quality using 5-point Likert scores across 6 domains [44, 45]. The survey will be administered through email online methods including email and WhatsApp, and participants will complete the survey online using REDCap. CritCom surveys are completed individually and averaged to obtain an institutional overall CritCom score and scores for each of six domains.
Data management and analysis. Data will be cleaned, managed, and analyzed in R [62]. The analysis will consist of two phases. First, we will produce network maps of team communications within each hospital. These maps will highlight how each team member communicates with other professions and disciplines at each hospital. Second, we will produce descriptive network statistics for each hospital, focusing on the interconnectedness, cross-profession connection patterns, and betweenness centralization [63–66]. Producing these statistics will identify any subgroups or other unique network patterns that arise within each of the hospital systems [64]. We are particularly interested in the network measure of betweenness centralization, which characterizes the hierarchical nature of clinical communication networks. Finally, we will build statistical models (exponential random graph model) [67] and explore the association of quality (CritCom scores) with structure (i.e., density) using the hospital-specific communication networks. This statistical model will help assess the probability that nodes (individuals) will have ties between them, allowing for the evaluation of predictors of communication based on individual characteristics and dyad attributes.
Aim 2. Co-develop a multilevel intervention to improve team communication quality in resource-variable hospitals
We will combine perspectives of clinicians across 20 hospitals regarding modifiable determinants of team communication to co-develop a multilevel intervention to improve communication quality. This convergent mixed methods design will consist of two phases: (1) qualitative assessment of staff perspectives on determinants of communication quality and how this relates to provider/patient outcomes, using quantitative data from prior work and Aim 1; and (2) intervention mapping to co-develop a feasible, implementable interventions across hospitals of varying resource levels.
Participant recruitment
Any individual who is eligible in Aim 1 will be eligible for Aim 2. Participants will complete individual interviews to allow for honest description of potential communication struggles at their hospital and between coworkers. Participants will be sampled purposively for a range of characteristics, including country income level, hospital size, professional role, and primary unit of clinical work. We aim to enroll around 15 individuals [68] with additional recruitment using snowball sampling as necessary until we achieve information power.
Data collection
Interviews will be conducted using Zoom in individuals’ preferred language (English, Spanish, Portuguese, or Arabic) using native-speaking research team members. The interviewers will be individuals who are not on the participant clinical team or involved in clinical care at the hospital to facilitate honest dialogue, and interviews will be audio-recorded. There will be three main sections to the interview guide: (1) communication quality, including questions about working relationships with other professionals, the six CritCom domains of quality communication, their experience during patient care events and how they would describe effective communication in their setting; (2) communication structure, including questions such as the frequency of communication types in their setting, experience of hierarchy in the work environment, and typical processes of communication during deterioration events; and (3) interventions, including questions about perceived barriers to improving communication (modifiable determinants) and strategies that would improve communication in their setting. We will not re-collect CritCom scores, but will use the data collected in Aim 1 during the synthesis phase.
Analysis plan
Audio recordings will be translated and transcribed into English using a professional service [69–72]. Transcripts will be de-identified, segmented, and uploaded to MAXQDA for analysis. A qualitative analysis team will develop an initial codebook with a priori codes informed by CritCom domains, structural analysis, and the conceptual frameworks (Figs. 1 and 2), including barriers and facilitators to communication and potential interventions. Additionally, inductive codes will be developed using a constant comparative approach with iterative memoing of transcripts to allow for novel themes. Iterative revision of the codebook will be conducted across three transcripts until a final codebook is developed. Once finalized, transcripts will be independently coded by two coders, with monitoring for interrater reliability. Discrepancies will be resolved through consensus and a third adjudicator. We anticipate using two approaches: categorical coding, describing the data according to broad domains, and thematic coding, describing the relationship between concepts included in our conceptual framework.
Data synthesis
Convergent analysis will include quantitative output from Aim 1 with qualitative data collected in Aim 2 to understand the relationship between organizational and team determinants of communication quality and between communication structure and quality. We will use joint displays [73, 74] to understand the results of both assessments, focusing on the six domains of communication quality and structural components elucidated through the network analysis. The research team and expert panel will review these results to gain a deeper understanding of modifiable determinants of communication quality. Identified communication barriers will be reviewed and discussed to identify determinants that could be foci for intervention. Non-modifiable determinants include organizational or individual factors that cannot be changed, such as participant length of experience (hypothesized quality determinant) or building layout (hypothesized structural determinant). However, modifiable factors will be targeted for potential intervention development.
Intervention mapping
We will use these mixed methods results to conduct intervention mapping with members of the expert panel to co-develop a multilevel team communication intervention. Intervention mapping is an evidence-informed six-step process to develop an intervention. The expert panel and engagement with the global oncology community will inform the selection and design of an intervention to address identified team communication challenges. We will use results from Aims 1 and 2 to define the problem. We will conduct a series of workshops both in person and virtually to complete the process. Through these workshops, the team will: (1) select intervention methods and change targets that are responsive to identified needs, (2) produce key implementation strategies and attributes for intervention implementation, and (3) combine these components into a coherent multilevel intervention that is appropriate for diverse resource-variable contexts [75–77]. We will use rigorous intervention mapping procedures consistent with prior research [78–80]. At the end, we will conduct a modified Delphi to prioritize interventions and select a multilevel intervention targeting different levels of action (provider, unit, hospital). We anticipate that this multi-level intervention will focus on provider behaviors and communication structures relevant during deterioration events.
Aim 3. Test feasibility, acceptability, appropriateness, and preliminary efficacy of a multilevel intervention to improve team communication quality in resource-variable hospitals
We will use a pilot waitlist control cluster randomized trial to assess the feasibility and preliminary efficacy of the intervention developed in Aim 2, which aims to facilitate a future hybrid implementation-effectiveness trial.
Study settings and recruitment
Eight hospitals will be identified from the lowest quartile of communication quality based on prior CritCom data and measured as the overall CritCom score. Previous site leads will be contacted for study participation. In partnership with the local site lead, the research team will send emails to all clinicians who meet the inclusion criteria. Identified participants will include all clinicians who care for hospitalized children with cancer at risk of deterioration. We will use marketing and materials at the hospital to increase awareness and will send up to four emails to complete the survey instruments at each time point.
Randomization to intervention
We will use a parallel-arm, pilot cluster-randomized wait list-controlled trial to evaluate the intervention compared to control. A wait list control is a group that does not receive an intervention during the study period, serving as an untreated comparison during the study, although they will receive the intervention after study completion [81]. This methodology was selected due to ethical concerns of restricting interventions in these settings. We will balance randomization on baseline CritCom scores to ensure distribution of communication quality across groups. Hospitals will be randomized to either the multilevel intervention or a wait list control using a 1:1 ratio via randomization protocol generated by the study biostatistician and implemented through REDCap’s randomization module. All baseline hospital and participant data will be collected prior to randomization.
Intervention
We will implement the multilevel intervention developed in Aim 2. We anticipate that this intervention might contain a training or series of trainings in conjunction with other systems changes, such as changing workflows and communication pathways. For this study, the intervention will be delivered by study team members but we anticipate that in the future it can be developed by local clinical team members. We will develop a full intervention manual following Aim 2 with input from the Expert Panel.
Training
To ensure the intervention is implemented consistently and all procedures are followed and assessed, the research team will facilitate and deliver the intervention components. A training on the intervention will be developed and refined to ensure consistent intervention delivery in the future and across hospitals. This will be consistent with our prior work [82, 83], and include information on hospital-level tailoring of the intervention. Training will also ensure consistency and accurate assessment of study outcomes.
Measures
We selected outcomes and covariates for this study in alignment with our prior work, expert guidance, and the conceptual framework. As a pilot study, the primary measures, in addition to assessing feasibility and recruitment in the trial, will focus on early implementation outcomes, including provider perception of the intervention's feasibility, acceptability, and appropriateness at their hospital. These will be assessed via brief, previously validated measures [61]. These items (4 questions for each measure) will be completed at 1 and 6 months following the completion of the intervention. To assess for feasibility of the study design and procedures, we will also track hospital and clinician recruitment and retention across the study.
The study will also assess preliminary effectiveness of the intervention. Communication quality, as measured by the CritCom survey, is the primary effectiveness outcome. This outcome will be calculated as changes in CritCom score (communication quality) from baseline to 6 months. The CritCom measure is collected at the individual level but will be analyzed as a hospital-level outcome, reflecting overall changes in hospital communication quality. Clinicians will be asked to complete the CritCom assessment and accompanying demographic questions at enrollment, one month after intervention delivery, and at the conclusion of the pilot (6 months after intervention). These time points are selected to allow for preliminary identification of when communication quality changes begin and align to the implementation outcome measures as described above.
In addition to impact on communication quality, we will explore intervention impact on secondary provider and patient effectiveness outcomes. Provider outcomes include burnout and retention and patient outcomesinclude clinical deterioration event mortality and safety/adverse events (cardiopulmonary arrest, cardiac arrest) [84]. These are considered exploratory as the trial is not powered to evaluate intervention effectiveness. We will evaluate these exploratory outcomes at three time points: baseline, three months after intervention, and six months after intervention. Provider outcomes will be based on self-report survey items collected along with the CritCom survey and demographic information. Patient outcomes will be reported by site leads via a de-identified prospective registry of all clinical deterioration events, defined as unplanned transfers to intensive care (ICU), the use of ICU interventions on general wards, or unplanned death on the ward [12]. All exploratory outcomes will be assessed as changes from baseline at 6 months.
Individual and hospital-level covariates
Participant-level demographic covariates include profession, role on the team, years working at the hospital, and sex. Hospital-level covariates include hospital type, funding structure, country income-level, staffing ratios, bed capacity, and annual new cancer diagnoses managed at the hospital per year.
Data collection
Implementation outcomes, communication quality (CritCom), demographic questions, and provider outcomes will be collected at the individual provider level. As described, eligible participants are clinicians who provide care to hospitalized children with cancer at risk of deterioration. Surveys will be distributed to study participants via confidential REDCap links at baseline, one month after the intervention, and at the study's completion (six months post-intervention). Hospital-level information and patient outcomes (clinical deterioration events) will be collected at the hospital level by the site lead. A de-identified report form will be completed by the site lead, or their delegate, for each deterioration event and will be entered into a REDCap database at the three data collection time points, consistent with our prior work [85–87]. Research team coordinators will complete analysis checks for missing and incomplete data and iteratively provide feedback to study teams.
Data analysis
Data will be managed, cleaned, and analyzed in R. As a pilot, this study is not powered to formally test effectiveness, and data analysis will focus on the feasibility of the intervention and procedures in preparation for a future trial. Data will be reported using descriptive comparisons by randomization assignment. We will describe participant and hospital characteristics overall and separately by arm. Categorical variables will be reported as N (%) and continuous variables will be reported as mean ± SD or median and interquartile range, as appropriate.
The measures of feasibility, appropriateness, and acceptability are assessed on a 5-point Likert scale. Therefore, we will report descriptive statistics of these measures prior to assessing variation via Kruskal–Wallis and Mann–Whitney tests. Data will be analyzed both at the individual and organization levels, to understand how individual and organizational factors influence intervention feasibility, appropriateness, acceptability and preliminary effectiveness. Recruitment and retention across the study will also be reported via descriptive statistics to assess feasibility of the study design and procedures for a future trial.
To evaluate the preliminary effectiveness of the intervention on perceived communication quality, we will use a linear mixed model approach where intervention is included as a fixed effect (intervention or control) along with randomization assignment, baseline score, time, and the interaction between time and intervention. We will evaluate the preliminary efficacy using a linear contrast to estimate the mean difference in communication quality (CritCom scores overall and by domain) from baseline to 6 months. To account for clustering due to individual- and hospital-level repeated measurements, we will include random terms for both in our mixed model. Exploratory provider and patient outcomes will be compared between the two randomization arms using the same mixed-effect analytic approach described for the primary effectiveness outcome. We will also conduct hospital-specific subgroup analyses to explore heterogeneity in intervention effects across hospitals.
Missing data
We anticipate having little missing data, due to our oversight and engagement strategies and observed response rates in our prior work [88, 89]. However, we will evaluate patterns in missing data and will analytically address missing data to avoid biasing the results. We will assume that data are missing at random, and mixed-effects models produce unbiased estimates in the presence of data missing at random [90]. We will ensure that our data meets all assumptions for statistical tests and will use data transformation or appropriate test alternatives as needed.
Dissemination plan
Our dissemination plan incorporates different audiences, including clinicians, researchers, and funders. We will share our findings through publication and conference presentations. All study team members, including members of the Expert Panel, will participate in authoring and publishing manuscripts. During the study, we will disseminate data to participating hospitals via reports, dashboards, and annual webinars [91]. Findings will also be shared with the global pediatric oncology community regularly through the St. Jude Global Alliance. All data that are produced will be made publicly available. We will focus on translational products to amplify impact and future scale, including dissemination of public goods [92] such as our measurement tools and intervention materials. Quantitative data from this study will be made available after data collection, cleaning, and de-identification. Additionally, we will make available all codebooks and results from the qualitative components.
Discussion
The TeamTalk study aims to develop a rigorous understanding of modifiable aspects of communication quality and structure to inform a co-developed, contextually responsive, feasible, and effective intervention to improve team communication and care for children with cancer across resource-variable hospitals globally. This study will provide a foundational understanding of modifiable determinants of team communication that impact pediatric cancer care to inform a multilevel intervention that responds to these determinants to improve childhood cancer outcomes. Ultimately, this work will improve team communication and outcomes for children with cancer in hospitals of all resource levels, thus advancing health equity globally.
This study is innovative in several ways. We will leverage implementation science and social network methods to focus on the relationship between communication structure and quality, and how they impact health outcomes, an important conceptual innovation. Additionally, this study will advance pragmatic multi-lingual measurement for team communication by using CritCom, a novel, reliable, multilingual measure of team communication. This measure was designed for clinical healthcare team use globally. This work will continue to provide construct validity for this pragmatic measure, advancing communication measurement in different linguistic settings, which is a major scientific barrier within the field. This work will shift approaches in how communication quality can be measured in clinical settings, resulting in opportunities to assess communication more broadly. Finally, this study emphasizes that improving team teamwork is a priority within cancer care [93–95], and quality of communication within teams impacts patient and provider outcomes [25, 26, 96–99]. To our knowledge, this will be the first study in pediatric oncology connecting provider- and hospital-level determinants to team communication structure and quality. Taken with prior work linking communication to outcomes, this research will provide novel empirical evidence to inform rigorous development of interventions to improve communication.
This study integrates implementation science theory to expedite the implementation of an evidence-informed, co-designed novel communication intervention in resource-variable settings. Many barriers limit implementation of new healthcare innovations [100]. On average, it takes 17 years for evidence to progress from discovery to delivery [101], and this timeframe is likely longer in low-resource settings. However, some models promote the continual improvement of care processes, which would ultimately increase high-quality healthcare. This proposal uses rapid, streamlined, participatory methods to identify local strengths along with relevant challenges to care delivery, then quickly leverage this contextual knowledge to develop and implement interventions to address identified challenges. This work thus provides important knowledge about how to effectively intervene on communication barriers by identifying communication facilitators and building on existing communicating supports to improve care. We have informed this study with implementation science principles to promote accelerated knowledge translation [102, 103] thus enhancing dissemination and the future scalability of these efforts. We expect the results of this work to advance health services research by establishing a rigorous approach for developing theoretically driven, empirically informed novel interventions that result in advances in care delivery in a range of clinical settings across all resource-levels.
Prior work demonstrates that effective team communication is a crucial determinant of quality care for children with cancer [93, 104, 105], yet little is known about how clinician communication networks vary across hospitals with different resource-levels and how these variations relate to care delivery. This study directly addresses this knowledge gap. This work will broaden our understanding of the role of healthcare team communication in pediatric cancer care through advancing the use of a novel measure of team communication quality and the development of an appropriate and feasible intervention. Ultimately, this research will design an intervention to make high-quality communication more likely, therefore having a direct impact on clinical practice and improve childhood cancer outcomes. This study will also allow for future work to evaluate both the implementation and effectiveness of this novel intervention in a larger hybrid-effectiveness trial, with a focus towards global scale-up and sustainability.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Global Initiative for Childhood Cancer. . http://www.who.int/cancer/childhood-cancer/en/
- 2St. Jude Global. Accessed March 2, 2020, https://www.stjude.org/global.html
- 3Agulnik A M-THPLTDCYCAKC-AARAGGMZTVD. Effect of paediatric early warning systems (PEWS) implementation on clinical deterioration event mortality among children with cancer in resource-limited hospitals in Latin America: a prospective, multicentre cohort study. Lancet Oncology. 2023;10.1016/S 1470-2045(23)00285-110.1016/S 1470-2045(23)00285-1PMC 1072709737433316 · doi ↗ · pubmed ↗
- 4The Joint Commission. http://www.jointcommission.org/sentinel_event.aspx
- 5Inadequate hand-off communication. Sentinel Event Alert. Sep 12 2017;(58):1–6.28914519 · pubmed ↗
- 6El Saghir NS, Keating NL, Carlson RW, Khoury KE, Fallowfield L. Tumor boards: optimizing the structure and improving efficiency of multidisciplinary management of patients with cancer worldwide. Am Soc Clin Oncol Educ Book. 2014:e 461–6. 10.14694/Ed Book_AM.2014.34.e 46110.14694/Ed Book_AM.2014.34.e 46124857140 · doi ↗ · pubmed ↗
- 7Mielke J, De Geest S, Zúñiga F, et al. Understanding dynamic complexity in context—Enriching contextual analysis in implementation science from a constructivist perspective. Hypothesis and Theory. Frontiers in Health Services. 2022-July-22 2022;210.3389/frhs.2022.95373110.3389/frhs.2022.953731 PMC 1001267336925847 · doi ↗ · pubmed ↗
- 8Agulnik A, Gonzalez Ruiz A, Muniz-Talavera H, et al. Model for regional collaboration: Successful strategy to implement a pediatric early warning system in 36 pediatric oncology centers in Latin America. Cancer. 2022;10.1002/cncr.3442710.1002/cncr.34427 PMC 982818636161436 · doi ↗ · pubmed ↗