A rare case of isolated unilateral pulmonary vein atresia presenting as interstitial lung disease in a young adult
Arnav Shandil, Mansi Verma, Sushma Makhaik, Sumala Kapila

TL;DR
A 21-year-old adult was diagnosed with a rare heart condition causing lung disease, typically seen in children.
Contribution
Presentation of a rare adult case of isolated unilateral pulmonary vein atresia with interstitial lung disease.
Findings
Unilateral pulmonary vein atresia was diagnosed in a 21-year-old adult.
The condition presented as unilateral interstitial lung disease.
This case highlights the rare occurrence of the condition beyond childhood.
Abstract
Unilateral pulmonary vein atresia is an unusual congenital cardiovascular abnormality. It occurs due to failure of incorporation of pulmonary veins into the left atrium. It is usually diagnosed in childhood and diagnosis after adulthood is very rare. Herein we present a case of 21-year-old young adult with isolated unilateral pulmonary vein atresia who presented with unilateral interstitial lung disease.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1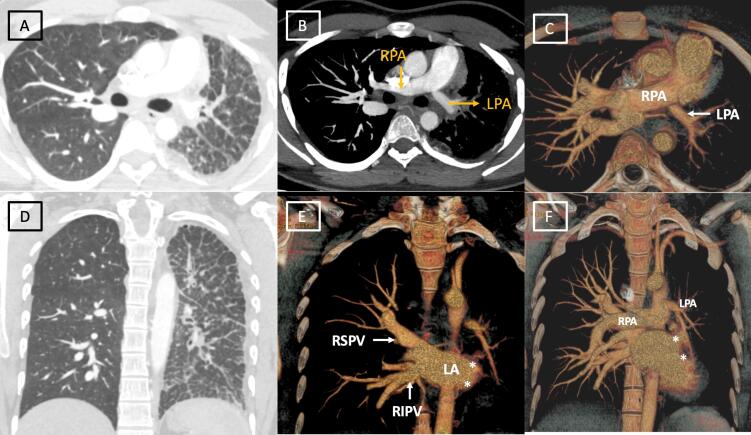 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Congenital Diaphragmatic Hernia Studies · Vascular Anomalies and Treatments
Introduction
Unilateral pulmonary vein atresia is a rare congenital anomaly which generally presents in infancy or childhood with pneumonia or recurrent hemoptysis.^1^ Cases of adult presentation are reported but are uncommon. The proposed mechanisms include presence of diaphragm completely occluding the veno-atrial junction or atresia of the extra pulmonary venous segment.^2^ It can be isolated or associated with other cardiovascular anomalies in 50% of the cases. ^3^
Case Presentation
A 21-year-old male presented with occasional dyspnea on exertion for 3 months. The patient did not have any respiratory symptoms during childhood with non-significant past medical history. There was no previous history of admission. He was afebrile and acyanotic with arterial oxygen saturation of 93%. Echocardiography revealed small left pulmonary artery with normal cardiac chambers, no valvular regurgitation and normal gradients across pulmonary valve.
Chest radiograph (Figure 1) demonstrated decreased volume of left hemithorax with diffuse reticular opacities and slight ipsilateral mediastinal shift. Computed tomography done for further evaluation revealed decreased left lung volume, ipsilateral mediastinal shift with interlobular septal thickening and areas of ground glass attenuation. (Figure 2 A, D) Interestingly, the left pulmonary artery was hypoplastic. (Figure 2 B, C) The right pulmonary artery was relatively dilated. However, there was absence of abrupt narrowing of peripheral pulmonary vessels, right ventricular hypertrophy or enlargement, thus excluding pulmonary artery hypertension.Pulmonary venous drainage to left atrium was normal on right side, however pulmonary veins were not visualized on left side with smooth lateral border of left atrium. (Figure 2 E, F) No bronchial obstruction was seen. No associated cardiac or venous anomaly was seen. Right heart catheterization revealed normal right pulmonary artery and right sided pressures. As the patient did not have any significant respiratory, cardiac or systemic symptoms, he is currently managed conservatively and is on follow up. Further plan is to perform left pneumonectomy as it will alleviate the nidus of infection and will remove the dead space causing exercise intolerance.
**
**
Discussion
Isolated unilateral pulmonary venous atresia (UPVA) is a rare congenital abnormality. To the best of our knowledge, few adult cases of isolated UPVA have been reported. UPVA results when common pulmonary vein fails to incorporate into the left atrium. This leads to inadequate gas exchange at the alveolar level leading to poor ventilation and oxygenation of the affected lung. Owing to markedly reduced flow, the ipsilateral pulmonary artery in the affected lung is underdeveloped with flow reversal towards the contralateral side and development of systemic to pulmonary artery collaterals.^4^
UPVA is associated with congenital heart defects like ventricular septal defect or double superior vena cava in approximately 50% of patients.^4^ On histological examination, these veins show intimal fibrosis without any inflammatory reaction.^5^ The most common presenting symptoms include recurrent infections of the respiratory tract and hemoptysis due to the systemic collateral supply to the affected lung. ^6^ The imaging findings on computed tomography include small hemithorax, a diminutive ipsilateral pulmonary artery and absence of ipsilateral pulmonary vein drainage into the left atrium. Parenchymal findings include ground-glass opacities and septal thickening, likely representing dilated lymphatics and bronchial veins.^5^ Later, unilateral interstitial lung disease develops due to chronic pulmonary edema.^7^
Unilateral pulmonary vein atresia is a diagnostic predicament, especially in adult patients. In presence of a confluent mediastinal soft tissue, lung malignancy and fibrosing mediastinitis that involves the hilar vessels, are the main differential diagnosis. However, the presence of a small hemithorax without any bronchial obstruction helps in diagnosing a congenital pathology. Pneumonectomy is the treatment option for alleviating the nidus of recurrent pneumonias and relieving significant left-to-right shunt.^5^ In long standing cases with severe pulmonary hypertension, lung transplantation is preferred.
Conclusion
UPVA is an unusual congenital anomaly with a diagnostic dilemma. Computed tomography aids in providing a definite diagnosis. Owing to variable clinical severity, the management has to be individualized in patients with no or mild symptoms.
Competing Interests
The authors declare no potential conflicts of interest with respect to research, authorship, and/or publication of this article.
Ethical Approval
As per institutional policy, ethical approval is not required for case reports.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cong CV Ly TT Duc NM Unilateral pulmonary vein atresia: literature overview and case report Radiol Case Rep 20221741313710.1016/j.radcr.2022.01.05735242258 PMC 8857560 · doi ↗ · pubmed ↗
- 2Sade RM Freed MD Matthews EC Castaneda AR Stenosis of individual pulmonary veins Review of the literature and report of a surgical case J Thorac Cardiovasc Surg 1974676953624827957 · pubmed ↗
- 3Latson LA Prieto LR Congenital and acquired pulmonary vein stenosis Circulation 20071151103810.1161/circulationaha.106.64616617200453 · doi ↗ · pubmed ↗
- 4Heyneman LE Nolan RL Harrison JK Mc Adams HP Congenital unilateral pulmonary vein atresia: radiologic findings in three adult patients AJR Am J Roentgenol 20011773681510.2214/ajr.177.3.177068111517073 · doi ↗ · pubmed ↗
- 5Pourmoghadam KK Moore JW Khan M Geary EM Madan N Wolfson BJ Congenital unilateral pulmonary venous atresia: definitive diagnosis and treatment Pediatr Cardiol 200324173910.1007/s 00246-002-0220-612360396 · doi ↗ · pubmed ↗
- 6Kim Y Yoo IR Ahn MI Han DH Asymptomatic adults with isolated, unilateral right pulmonary vein atresia: multidetector CT findings Br J Radiol 2011841002 e 1091310.1259/bjr/5134466121606062 PMC 3473637 · doi ↗ · pubmed ↗
- 7Nasrallah AT Mullins CE Singer D Harrison G Mc Namara DG Unilateral pulmonary vein atresia: diagnosis and treatment Am J Cardiol 19753679697310.1016/0002-9149(75)90092-21239185 · doi ↗ · pubmed ↗