Glomerular disease associated with cancer: a case series of paraneoplastic nephrotic syndrome
Mengsi Hu, Qiqi Ma, Liguang Wang, Tingwei Zhang, Jiangong Lin, Xiaowei Yang, Zhimei Lv, Rong Wang

TL;DR
This paper reports cases of kidney disease linked to cancer, showing improvement with cancer treatment alone.
Contribution
The study highlights rare cases of nephrotic syndrome linked to specific cancers and their response to oncological treatment.
Findings
PNS was observed in patients with ovarian, pancreatic, and bladder cancers.
Patients improved without corticosteroids or immunosuppressants.
Cancer treatment was sufficient for remission in these cases.
Abstract
The association between glomerular diseases and malignancies has been recognized since the 1920s. A diverse spectrum of glomerular lesions can occur in various neoplasms, including both hematologic malignancies and solid tumors. This study presents a case series of paraneoplastic nephrotic syndrome (PNS) associated with three solid tumors: ovarian cancer, pancreatic neuroendocrine tumor (NET), and bladder cancer. The occurrence of PNS is rarely reported in association with these malignancies. Notably, all patients achieved complete or partial remission without receiving corticosteroids or immunosuppressant therapy. These observations accentuate the critical role of malignancy in the pathogenesis of glomerulopathy and underscore the therapeutic primacy of oncological control in such patients.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
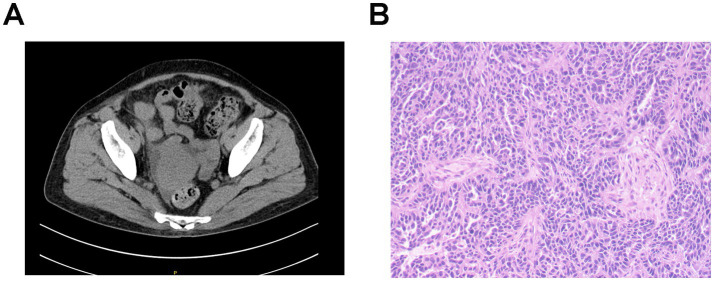 Figure 1
Figure 1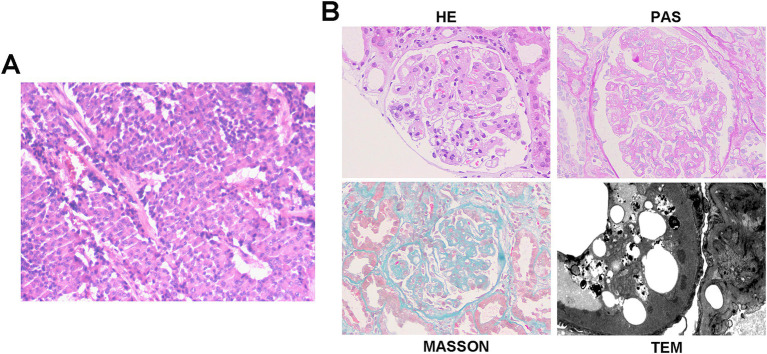 Figure 2
Figure 2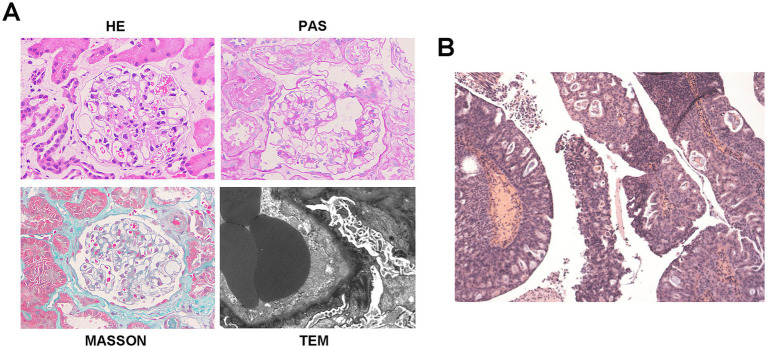 Figure 3
Figure 3| Indicators | Case 1 | Case 2 | Case 3 |
|---|---|---|---|
| Demographics | |||
| Age (years)/Sex | 71/F | 57/M | 72/M |
| Malignancy | |||
| Tumor type | Ovarian cancer | Pancreatic NET | Bladder cancer |
| Histology/Stage | Stage IIIC high-grade serous ovarian carcinoma | G2 | High-grade papillary urothelial carcinoma |
| Renal involvement | |||
| Pathology | NA | MPGN | MN |
| 24 h UTP (g/d) | 12.80 | 10.93 | 5.28 |
| Serum Albumin (g/L) | 19.30 | 23.20 | 28.50 |
| Treatment | |||
| Antitumor therapy | Cytoreductive surgery, Paclitaxel/Carboplatin, Bevacizumab | Surufatinib, Sandostatin LAR, TACE, Everolimus | TURBT, Pirarubicin irrigation, BCG immunotherapy |
| Renal therapy | Supportive care, Irbesartan | Supportive care | Losartan, Dapagliflozin |
| Steroids/Immunosuppression | None | None | None |
| Outcome | |||
| Renal response | Complete remission | Partial remission | Complete remission |
| Oncologic response | Progressive disease | Progressive disease | Stable disease |
| Cases | Age | Clinical onset of renal lesion | Discovery of neoplasm | Renal lesion | Type of cancer | Treatment | Outcome at last follow up | |
|---|---|---|---|---|---|---|---|---|
| Pathology | Histology of ovarian cancer | Renal outcome | Tumor outcome | |||||
| #1 ( | 65 | 1987 | 1987 | NA | Metastatic adenocarcinoma from an ovarian primary | Surgery and chemotherapy | Partial remission | Unknown |
| #2 ( | 68 | April 2000 | May 2000 | NA | Ovarian adenocarcinoma | Surgery and chemotherapy | Partial remission | Death |
| #3 ( | 73 | October 2008 | October 2008 | MCD | Papillary serous adenocarcinoma | Steroids and immunosuppressive therapy | No response | Unknown |
| #4 ( | 6 | NA | NA | MN | Sertoli-Leydig ovarian tumor | Surgery and chemotherapy | Remission | Unknown |
| #5 ( | 65 | 6 months before tumor | NA | MN | NA | Chemotherapy | Remission | Normalize CA125 |
| #6 ( | 59 | October 2000 | May 2001 | MN | Ovarian carcinoma | Chemotherapy | Complete remission | Complete remission |
| #7 ( | 7 | March 1979 | December 1979 | MN | Teratoma | Prednisone and surgery | Complete remission | Unknown |
| #8 ( | NA | 1988 | NA | MN | Ovarian adenocarcinoma | Steroids and surgery | Remission | Unknown |
| #9 ( | 55 | December 2002 | December 2002 | MCD | Papillary serous carcinoma | Prednisolone and adjuvant chemotherapy | Complete remission | Unknown |
| #10 ( | 65 | January 2007 | November 2004 | MN | Ovarian clear cell carcinoma | Surgery, steroid and cyclophosphamide | Remission | Alive |
| #11 ( | 55 | December 2008 | December 2008 | MCD | Teratoma | Surgery combined with corticosteroids | Complete remission | Unknown |
| #12 ( | 36 | 2013 | NA | MCD | Teratoma | Surgery and prednisone | Remission | Unknown |
| #13 ( | 46 | 2019 | NA | MN | Serous cyst adenofibroma | Steroids and surgery | Partial remission | Unknown |
| #14 ( | 16 | NA | 25 days after NS | MPGN | Teratoma | Prednisone, surgery and Cyclosporine A | Complete remission | Unknown |
| #15 ( | 65 | April 1960 | November 1961 | MN | Ovarian adenocarcinoma | Surgery | Unknown | Death |
| #16 ( | 64 | October 1992 | October 1993 | AL | Ovarian carcinoma | Surgery | Renal failure | Death |
| #17 ( | February 1992 | October 1994 | MPGN | Ovarian endodermal sinus tumor | Prednisone and ACEI; surgery and chemotherapy | Renal failure | Unknown | |
| #18/19 ( | 59/72 | NA | NA | MCD/MCD | NA | Surgery | One with renal failure for, the other unknown | Unknown |
| #20 ( | 28 | After tumor removal | NA | MN | Ovarian dermoid cyst | Steroid | No response | Unknown |
| Case | Age | Sex | Renal lesion | Type of cancer | Treatment | Outcome | |
|---|---|---|---|---|---|---|---|
| Pathology | Histology of NEN | Renal outcome | Tumor outcome | ||||
| #1 ( | 69 | Male | MN | High-grade neuroendocrine carcinoma (pT3N0) | Surgery | AKI | Unknown |
| #2 ( | 57 | Female | MN | Non-malignant NET | Surgery, Steroids, Telmisartan | Partial remission | Stable disease |
| Pathology | Histology of bladder cancer | Renal outcome | Tumor outcome | ||||
| #1 ( | NA | NA | NA | NA | NA | NA | NA |
| #2 ( | 66 | Female | MCD | Bladder transitional cell carcinoma | Surgery | Complete remission | Unknown |
| #3 ( | 50 | Male | MPGN | Bladder transitional cell carcinoma | Surgery | Complete remission | Unknown |
| #4 ( | 75 | Male | MN | Bladder transitional cell carcinoma | Surgery | Remission | Unknown |
| #5 ( | 54 | Male | MN | Low-grade transitional cell carcinoma | Surgery, BCG injection, Steroids | Remission | Remission |
| #6 ( | 68 | Male | MN | THSD7A-positive bladder cancer | Steroid; Surgery | No response; Remission | Unknown |
| #7 ( | 57 | Male | Renal amyloidosis | Bladder small cell carcinoma | Unknown | Unknown | Unknown |
| #8 ( | 76 | Male | NA | Bladder urothelial carcinoma | Surgery | Complete remission | Death |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal Diseases and Glomerulopathies · Amyloidosis: Diagnosis, Treatment, Outcomes · Renal cell carcinoma treatment
Introduction
The association between glomerular diseases and malignancies was first recognized as early as the 1920s by Galloway in patients with Hodgkin’s disease (1). Subsequent studies have reported that renal involvement may occur in over 7% of cancer patients. (2, 3). A recent Brazilian retrospective cohort analysis found that 1.97% of patients had concurrent glomerulopathy and neoplasms, with hematologic malignancies being the most common (35.8%), followed by colon and gynecologic tumors (4).
In this study, we present a case series of paraneoplastic nephrotic syndrome (PNS) in association with three solid tumors: ovarian cancer, pancreatic neuroendocrine tumor (NET), and bladder cancer. The occurrence of PNS in conjunction with these malignancies is rarely documented. Notably, all patients achieved complete or partial remission without corticosteroid or immunosuppressive therapy. These observations accentuate the critical role of malignancy in the pathogenesis of glomerulopathy and underscore the therapeutic primacy of oncological control in these patients.
Case report
Case 1
A 71-year-old Chinese woman presented with bilateral lower limb edema. Her medical history included well-controlled diabetes mellitus and hypertension, managed with irbesartan. Physical examination revealed periorbital and lower extremity edema with normal blood pressure. Laboratory tests demonstrated nephrotic-range proteinuria (24 h UTP 12.80 g/d), severe hypoalbuminemia (serum albumin 19.30 g/L), and marked hyperlipidemia (triglycerides 4.56 mmol/L, total cholesterol 8.83 mmol/L, and LDL-C 5.73 mmol/L). Renal function remained relatively normal (serum creatinine 0.70 mg/dL, eGFR 87.40 mL/min/1.73m^2^, CKD-EPI 2009). Serological tests, including phospholipase A2 receptor antibodies (PLA2R-Ab), autoantibodies, viral markers, serum complement, and immunofixation electrophoresis, were all negative. Fundoscopy showed no diabetic retinopathy, consistent with her glycemic control (HbA1c 6.1%).
Gynecological ultrasound and abdominal CT scanning revealed a right adnexal cystic-solid mass (9.1 × 7.4 × 6.2 cm) and an irregular peri-uterine soft tissue lesion with poorly defined boundaries (5.3 × 6.0 cm), respectively. Tumor markers were significantly elevated (CA125 311.00 U/mL [normal<25], HE4 1414.00 pmol/L [normal<140]). The patient declined a renal biopsy and underwent cytoreductive surgery, which confirmed stage IIIC high-grade serous ovarian carcinoma (Figure 1). Post-operative management included intraperitoneal carboplatin and supportive therapy (metformin, insulin, statins, irbesartan, low molecular weight heparin, and diuretics). Tumor markers significantly declined post-operatively (CA125 191 U/mL, HE4 145 pmol/L), while proteinuria persisted (3+), and serum albumin decreased to 16 g/L but increased to 25.9 g/L after albumin infusions. Her renal function remained stable throughout hospitalization, and the patient was discharged with persistent edema.
Imaging and pathological characteristics of ovarian cancer in patient 1. (A) Abdominal CT scanning indicates an irregular soft tissue near the uterus without obvious boundaries with the uterus. (B) Histopathology shows right adnexal high-grade serous carcinoma. Tumor dimensions: 6.5 × 5 × 4 cm. Lymphovascular space invasion present (cancer emboli identified). Metastatic lesions identified in: right fallopian tube, right parietal peritoneum, and omentum. Uterus and left adnexa: carcinomatous involvement of the uterine serosal surface, and the left ovary and left fallopian tube show no significant lesions. Immunohistochemistry results: WT-1 (+), Vimentin (−), P16 + (patchy/mottled staining pattern), P53 (−), Ki-67 + (60% proliferation index), ER (−), PR (−), and PAX8 (+).
During the 6-month follow-up, the patient received paclitaxel and carboplatin-based adjuvant chemotherapy. Notably, 1 month after surgery and prior to initiating chemotherapy, laboratory tests showed signs of NS remission, evidenced by reduced proteinuria (2+), improved serum albumin (30 g/L), and resolved edema, without albumin infusion, steroids, or immunosuppressants. Her tumor markers continued to decline at this time point (CA125 45.3 U/mL, HE4 89.0 pmol/L). Complete remission of NS was observed at 4-month post-surgery, with sustained normalization of both CA125 and HE4 levels. At 1-year follow-up, CT scanning showed disease progression with new soft tissue lesions in the left pelvic wall. Consequently, over the next 6 months, the patient received six cycles of combined paclitaxel/carboplatin chemotherapy, with bevacizumab added in the first and the last cycles, and her tumor markers increased (CA125 24.8 U/mL, HE4 299 pmol/L). Nevertheless, despite tumor progression, renal remission persisted throughout the subsequent 1.5 years, with no proteinuria (24 h UTP 0.09 g/d), normal serum albumin (38.2 g/L), and stable renal function (eGFR 90.0 mL/min/1.73m^2^).
Case 2
A 57-year-old Chinese man was admitted with bilateral lower limb edema for 2 months and elevated serum creatinine for 20 days. His medical history included hypertension, treated with calcium channel blockers, and a pancreatic NET G2 (Figure 2A), for which he had undergone distal pancreatectomy, splenectomy, and metastatic liver resection 18 months prior. Physical examination showed lower extremity edema. Laboratory tests revealed nephrotic-range proteinuria (24 h UTP 4.98 g/d), microscopic hematuria (17.2 RBCs/HPF), hypoalbuminemia (serum albumin 24.9 g/L), hyperlipidemia, and preserved renal function (eGFR 85.0 mL/min·1.73m^2^, CKD-EPI 2009). All serological tests were negative.
Histopathology of pancreatic NET and kidney in case 2. (A) Histopathology shows pancreatic neuroendocrine tumor, grade 2 (NET G2). Tumor size: 11 × 6 cm. Mitotic rate: 5 per 50 high-power fields (HPFs). Status of resection margins: Negative for tumor involvement. Adjacent structures: pancreatic transection margin: tumor-free; splenic parenchyma: no tumor identified; left adrenal gland: uninvolved. Hepatic metastases: left hepatic lobe: ingle metastatic deposit (10 × 9 cm) confirmed as metastatic NET; resection margin: clear; right hepatic lobe: two metastatic foci (4.5 × 3.5 cm and 2 × 1.8 cm), histologically consistent with metastatic NET; larger lesion abuts the capsular surface; resection margins: free of tumor. Lymph node status: peripancreatic lymph node (1/1): no metastatic involvement. Immunohistochemistry results: CK(AE1/AE3) (+), Vimentin (−), CK7(−), CK8/18(+), CK19 (+), CD56 (+), Syn (+), CgA (+), B-Catenin (+), and Ki-67(20%). (B) Representative of renal pathology of case 2.
Renal biopsy showed 29 glomeruli, eight with segmental sclerosis and adhesions, diffuse capillary wall thickening with double contours, mild-to-moderate mesangial proliferation, and scattered deposits on Masson staining. Interstitial fibrosis (10–20%) and tubular atrophy (20%) with inflammation were present. A diagnosis of mesangial proliferative glomerulonephritis (MPGN) was made (Figure 2B). Retrospective reviews indicated pre-existing proteinuria (2+) with hypoalbuminemia before surgery (38.5 g/L). Postoperatively, the patient received surufatinib for 16 months, with stable disease, and his proteinuria resolved and albumin normalized 3-month post-surgery without any additional interventions.
One month before admission, routine follow-up revealed the onset of NS (4 + proteinuria, 24 h UTP 10.93 g/d, serum albumin 23.2 g/L, LDL-C 8.76 mmol/L) with acute kidney injury (AKI) (serum creatinine 138.2 μmol/L) and radiographic disease progression. Surufatinib was then switched to sandostatin LAR due to suspected nephrotoxicity. Paraneoplastic MPGN was diagnosed based on temporal association, exclusion of other causes, and atypical pathology. Symptomatic treatment was initiated with diuretics, statins, and indobufen due to his intolerance of AECI/ARBs and recent AKI. At discharge, his renal function improved (serum creatinine 86.8 μmol/L) with partial edema resolution.
At the 1-month follow-up, the disease progressed despite sandostatin LAR therapy, prompting transarterial chemoembolization (TACE) and a switch to everolimus. Laboratory results showed decreased proteinuria (2+, 24 h UTP 3.89 g/d) with improved albumin levels (28.5 g/L), lipid profile (LDL-C 2.98 mmol/L), and renal function (serum creatine 71.6 μmol/L, eGFR 107.0 mL/min·1.73m^2^). At 4 months, disease progression continued, complicated by a liver abscess requiring drainage and antibiotic therapy, and NS was exacerbated (3 + proteinuria, serum albumin 23.3 g/L, LDL-C 7.22 mmol/L), leading to everolimus suspension. Partial remission of NS was observed after 6 months (albumin 30.3 g/L without infusion), allowing everolimus resumption. Sustained partial remission was noted at the 1-year follow-up (2 + proteinuria, albumin 34.0 g/L) with stable renal function (serum creatinine 66.3 μmol/L), which persisted over subsequent local follow-up until the last assessment at 1.5 years.
Case 3
A 72-year-old Chinese man presented with a 5-month history of bilateral lower limb edema. His medical history included atrophic gastritis, treated with rebamipide, and a varicectomy a decade earlier. The patient denied any history of smoking or alcohol consumption. Physical examination revealed mild lower extremity edema. Laboratory findings indicated nephrotic-range proteinuria (24 h UTP 5.28 g/d), microscopic hematuria (4.8 RBCs/HPF), hypoalbuminemia (28.5 g/L), hyperlipidemia (total cholesterol 6.2 mmol/L, LDL-C 4.33 mmol/L), and normal renal function (eGFR 98.0 mL/min·1.73m^2^, CKD-EPI 2009). All serological tests were negative. Abdominal and urinary ultrasonography showed mild fatty liver, prostatic hyperplasia, and vascular atherosclerosis.
Renal biopsy of 17 glomeruli revealed diffuse capillary wall thickening and podocyte swelling without mesangial proliferation, along with scattered deposits on Masson staining. There was minor tubular atrophy and interstitial fibrosis with mild inflammation. Immunofluorescence showed granular deposits of IgG (IgG1) and light chain deposits along the capillary walls, and PLA2R staining was negative. A diagnosis of atypical membranous nephropathy (MN) or PLA2R-unrelated MN was made (Figure 3A). The patient responded well to diuretics and statins and was discharged on losartan, statins, and indobufen.
Histopathology of bladder cancer and kidney in case 3. (A) Representative of renal pathology of case 3. (B) Histopathology shows high-grade papillary urothelial carcinoma. Morphological variant: Focal glandular differentiation. Tumor dimensions: 2.0 × 1.5 × 0.5 cm.
At the 4-month follow-up, partial NS remission was observed with reduced proteinuria (24 h UTP 1.56 g/d) and normalized serum albumin (41.6 g/L), though hematuria persisted (40.5 RBCs/HPF). At 5 months, urinary ultrasonography and CT urography showed multiple bladder masses (largest 1.4 × 1.2 cm) and retroperitoneal lymphadenopathy. NS was still in partial remission (24 h UTP 1.44 g/d, serum albumin 39.6 g/L, LDL-C 3.58 mmol/L), with improved urinalysis. The patient underwent transurethral resection of the bladder tumor (TURBT) with postoperative pirarubicin irrigation, which confirmed high-grade papillary urothelial carcinoma with focal adenoid differentiation (Figure 3B). Post-operatively, the patient received Bacillus Calmette–Guerin (BCG) immunotherapy and continued conservative treatment with losartan and dapagliflozin. Three-month post-operatively, near-complete renal remission was achieved, evidenced by minimal proteinuria (24 h UTP 0.62 g/day), normal serum albumin (41.4 g/L), normal lipid levels (LDL-C 1.96 mmol/L), and stable renal function (eGFR 92.49 mL/min/1.73m^2^). This remission was sustained at the 8-month postoperative follow-up, with repeat urinary ultrasonography showing no evidence of recurrence and a further reduction in proteinuria (24 h UTP 0.10 g/day).
Discussion
Paraneoplastic glomerular diseases refer to glomerular lesions that are indirectly caused by the presence of malignancy through tumor-related mechanisms and which tend to improve following effective treatment of the underlying cancer (5). The clinical diagnosis is often supported by the following characteristics (6, 7): (1) Clinical manifestations of renal injury have a time correlation with tumor (5, 8), especially within 2 years (9); (2) effective treatment of tumor, either surgical or chemical, is the premise for clinical and histologic remission of renal injury (10); (3) deterioration of renal function attributed to tumor relapse (5, 11); and (4) a pathophysiological connection between glomerular lesion and tumorigenesis, namely tumor antigens or antibody components detected by pathological examination (6). Among these, MN represents the most frequently reported histologic pattern, although other pathological alterations may occur (5, 12, 13). Importantly, there are currently no established consensus guidelines for the management of both cancer and paraneoplastic glomerulopathy (14, 15). In this context, we present three rare instances of solid malignancy-associated NS, including ovarian cancer, pancreatic NET, and bladder carcinoma, which are highly suggestive of a paraneoplastic etiology. A paramount and unifying observation across all cases is the achievement of complete or partial NS remission solely through antitumor and supportive therapies, without the use of corticosteroids or immunosuppressive agents. This finding accentuates a critical role of underlying malignancy in the pathogenesis of glomerulopathy in these patients and underscores the therapeutic primacy of oncological control. Clinical characteristics, management, and outcomes of three presenting cases are summarized in Table 1.
Ovarian cancer, one of the most common gynecologic malignancies, frequently presents with non-specific symptoms in its early stages (16, 17). Its association with paraneoplastic glomerulopathy remains rare, with only 20 documented cases to date (including 5 benign teratomas) (Table 2) (18–33). Notably, 70% (14/20) of these patients achieved renal remission during follow-up, despite approximately half receiving steroids or immunosuppressive therapy, suggesting a favorable renal prognosis in ovarian cancer-associated PNS, although oncologic outcomes were frequently unreported. Recent studies have also indicated associations between gynecological neoplasms and glomerular lesions, although the histological characteristics remain undefined (4). In our first case, the temporal dynamics between tumor activity and renal response were particularly revealing. Although a definitive histological diagnosis is lacking, complete and sustained NS remission was induced following cytoreductive surgery and chemotherapy, providing strong clinical evidence for a paraneoplastic etiology. Although the patient had been on long-term irbesartan therapy prior to the onset of NS, and spontaneous remission could not be entirely ruled out, the immediate response to tumor debulking remains the most plausible explanation and underscores the value of steroid-sparing approaches in such scenarios. Another important point is the potential nephrotoxicity of oncological therapies, such as bevacizumab, used in this case. Bevacizumab is a monoclonal antibody targeting vascular endothelial growth factor (VEGF-A) and is known to be associated with proteinuria and other glomerular lesions, such as glomerular microangiopathy (34, 35). Critically, the temporal sequence of events in this patient, which showed significant renal improvement after tumor-directed therapy but persisted despite the administration of bevacizumab, supports the primacy of a paraneoplastic mechanism–rather than drug-induced nephrotoxicity—is the primary cause. Notably, the renal remission in this case proved remarkably resilient, persisting even upon subsequent oncologic progression, a phenomenon rarely documented in prior ovarian cancer-associated PNS cases. This suggests that initial reduction in tumor burden might disrupt paraneoplastic pathways sufficiently to induce prolonged stabilization of glomerular permeability, independent of later tumor progression, which is consistent with previous findings that glomerular lesions may be indirectly related to tumor burden, invasion, or metastasis (5, 6).
In this case, the initial parallel decline of both CA125 and HE4 with NS remission, followed by their subsequent dissociation (isolated HE4 elevation during cancer progression without NS relapse), revealed a fascinating nuance not previously emphasized in the literature. This dissociation may be clinically significant, since HE4 has been shown to possess higher specificity for ovarian malignancy than CA125 (36, 37), and its elevation has been observed in chronic kidney disease (CKD) independent of renal function (38, 39). Therefore, the isolated HE4 increase likely reflected genuine tumor progression, whereas the sustained NS remission suggested a decoupling of the paraneoplastic mechanism. This observation suggests complex biomarker interactions in PNS that merit further investigation.
Neuroendocrine neoplasms (NENs) represent a diverse group of tumors predominantly originating from gastroenteropancreatic (GEP) tissues (40, 41). The majority are indolent neuroendocrine tumors (NETs), while approximately 10–20% are neuroendocrine carcinomas (NECs) with rapid disease progression (41, 42). To date, only two cases of NEN-associated PNS have been reported worldwide, one including a case of pancreatic NEC (43), and another a pancreatic NET (Table 3) (44). Our study presents the third global case and the first Asian case of pancreatic NEN-related PNS. Of particular interest is the temporal pattern of the paraneoplastic glomerulopathy, occurring before the administration of sunitinib and remitting during postoperative surufatinib therapy, and recurring with tumor progression. This pattern strongly suggests that tumor burden, rather than drug toxicity (45, 46), serves as the primary driver of renal injury, similar to our first case. More notably, subsequent tumor progression under everolimus therapy was paradoxically associated with partial NS remission, indicating a complex and non-linear relationship between tumor burden and paraneoplastic glomerulopathy. This observation also suggests a potential nephroprotective role for everolimus through mTORC1 inhibition, as demonstrated in previous studies (36, 37), adding a novel therapeutic dimension to the management of such complex cases that has not been adequately described in the existing literature.
In the literature, only eight cases of bladder tumor-related paraneoplastic NS have been reported (47–54), with four cases demonstrating partial or complete NS remission after surgical treatment. Corticosteroid therapy failed to improve proteinuria in two of these cases (49, 50), contrasting with the more favorable renal outcomes observed in ovarian cancer-associated PNS. Our third case of bladder cancer-associated MN provides critical new insights into its diagnostic and therapeutic challenges. Although the pathological pattern itself may not be unusual, the clinical presentation and course were highly instructive, expanding upon the eight previously reported cases of bladder tumor-related PNS (47–54). Different from prior cases (Table 3), in our patient, the manifestation of NS preceded bladder malignancy detection by several months. Significantly, partial remission was achieved with losartan monotherapy even before tumor detection, and this remission was further accelerated following surgical resection. This might be attributed to diagnostic limitations, since initial urological screening with ultrasonography revealed no masses at the time of NS diagnosis, while sensitive methods, including CT urography or contrast-enhanced ultrasound, are not routinely applied for scanning NS patients in the clinical setting, even in the elderly. Furthermore, while malignancy-associated MN is associated with other antigens such as THSD7A (13, 55), these biomarker assays are not yet widely integrated into routine clinical practice in our institution, due to cost constraints. Importantly, the observed treatment response in the third case indicates a dual potential mechanism: first, the reduction in tumor burden removes the antigenic stimulus; second, angiotensin receptor blockers (ARBs) may exert nephroprotective and potential antitumor effects by inhibiting the renin–angiotensin–aldosterone system (RAAS), which has been implicated in tumorigenesis via signaling pathways including Ras/RAF/MAPK/ERK, PI3K/AKT/mTOR, and Wnt/β-catenin (56–61). Therefore, this case highlights the importance of maintaining a high index of suspicion for occult malignancy in patients with NS, even after an initially negative urological evaluation, and the importance of scheduled monitoring, even after treatment initiation.
Current understanding of paraneoplastic glomerulopathy pathogenesis remains incomplete despite several proposed molecular mechanisms (62–66). Our cases contribute to this understanding by demonstrating that: (1) the relationship between tumor burden and glomerulopathy is not always linear and may exhibit complex temporal dynamics; (2) different cancer types may use distinct pathophysiological pathways to induce glomerular injury, which may be reflected in variations of specific biomarkers; (3) non-immunosuppressive treatments, including both RAAS inhibition and targeted antitumor agents, can be effective while potentially minimizing side effects; and (4) certain antineoplastic agents may possess underrecognized nephroprotective effects in PNS. Future research should prioritize the identification of novel biomarkers through the analysis of renal biopsy specimens from cancer patients with glomerular involvement, combined with functional validation in reliable in vitro and in vivo models. Large-scale cohort studies are needed to identify epidemiological characteristics, including the influence of race, ethnicity, age, and gender, as well as temporal relationships between tumor diagnosis and renal manifestations. Such investigations would advance our understanding of disease mechanisms and contribute to the establishment of more precise diagnostic criteria and prognostic indicators for this complex paraneoplastic phenomenon.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Galloway J, Remarks ON HODGKIN'S DISEASE. Br Med J, (1922). 2: p. 1201–1208.2.20770949 10.1136/bmj.2.3234.1201 PMC 2417333 · doi ↗ · pubmed ↗
- 2Puolijoki H Mustonen J Pettersson E Pasternack A Lahdensuo A. Proteinuria and haematuria are frequently present in patients with lung cancer. Nephrol Dial Transplant. (1989) 4:947–50. doi: 10.1093/ndt/4.11.947, PMID: 2516885 · doi ↗ · pubmed ↗
- 3Sawyer N Wadsworth J Wijnen M Gabriel R. Prevalence, concentration, and prognostic importance of proteinuria in patients with malignancies. Br Med J (Clin Res Ed). (1988) 296:1295–8. doi: 10.1136/bmj.296.6632.1295, PMID: 3133055 PMC 2545767 · doi ↗ · pubmed ↗
- 4Laferreira MS Kirsztajn GM. Potentially paraneoplastic glomerulopathies in a Brazilian cohort: a retrospective analysis. J Bras Nefrol. (2025) 47:e 20240131. doi: 10.1590/2175-8239-jbn-2024-0131 en, PMID: 39878345 PMC 11781679 · doi ↗ · pubmed ↗
- 5Lien YH Lai LW. Pathogenesis, diagnosis and management of paraneoplastic glomerulonephritis. Nat Rev Nephrol. (2011) 7:85–95. doi: 10.1038/nrneph.2010.171, PMID: 21151207 PMC 3058941 · doi ↗ · pubmed ↗
- 6Ronco PM. Paraneoplastic glomerulopathies: new insights into an old entity. Kidney Int. (1999) 56:355–77. doi: 10.1046/j.1523-1755.1999.00548.x, PMID: 10411717 · doi ↗ · pubmed ↗
- 7Bacchetta J Juillard L Cochat P Droz JP. Paraneoplastic glomerular diseases and malignancies. Crit Rev Oncol Hematol. (2009) 70:39–58. doi: 10.1016/j.critrevonc.2008.08.003, PMID: 18790651 · doi ↗ · pubmed ↗
- 8Pani A Porta C Cosmai L Melis P Floris M Piras D. Glomerular diseases and cancer: evaluation of underlying malignancy. J Nephrol. (2016) 29:143–52. doi: 10.1007/s 40620-015-0234-9, PMID: 26498294 PMC 4792341 · doi ↗ · pubmed ↗