Solid–Basaloid Adenoid Cystic Carcinoma of the Ipsilateral Breast Remnant in Postoperative Luminal HER2-Type Breast Cancer: A Case Report
Yuji Kobayashi, Kanako Miyazawa, Kayoko Shinseki, Akihiro Kushima, Masaya Takahashi, Mariko Fujibayashi

TL;DR
A rare case of solid–basaloid adenoid cystic carcinoma in the breast of a patient previously treated for breast cancer is reported.
Contribution
This paper presents a rare case of SB-AdCC in a postoperative breast remnant, highlighting its aggressive nature and triple-negative classification.
Findings
The patient had a high Ki-67 index of 80%, indicating high-grade malignancy.
The tumor was diagnosed as triple-negative and SB-AdCC following histological examination.
The patient showed no signs of metastasis one year after surgery and chemotherapy.
Abstract
Solid–basaloid adenoid cystic carcinoma (SB-AdCC) is a rare and aggressive variant of AdCC of the breast. Moreover, it is an extremely rare subtype of triple-negative breast cancer, accounting for <1% of all breast cancers. We report a case of SB-AdCC. Ten years ago, an 82-year-old woman underwent a partial mastectomy for the luminal HER2 (human epidermal growth factor receptor type 2)-type invasive ductal carcinoma of the left breast cancer. Ten years later, she noticed another lump in her left breast. A needle biopsy was performed, and an unclassified carcinoma was detected. Histological examination revealed that the carcinoma was of the triple-negative type. A mastectomy of the left breast and sentinel lymph node biopsy were performed. The postoperative pathological diagnosis was an SB-AdCC of the breast. The Ki-67 index was 80%, corresponding to a high-grade malignancy. She…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
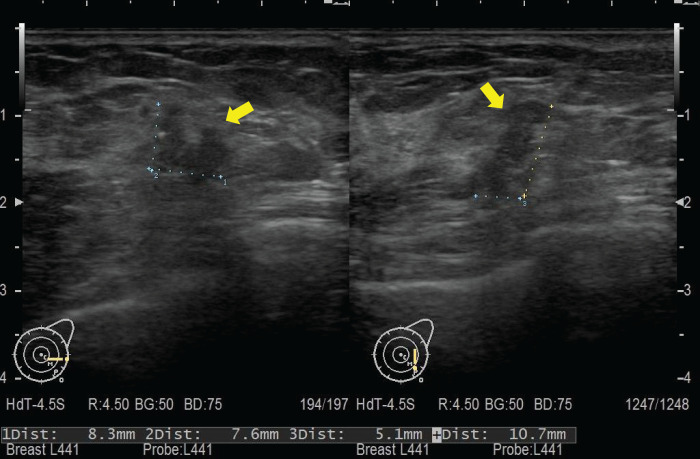 Fig. 1
Fig. 1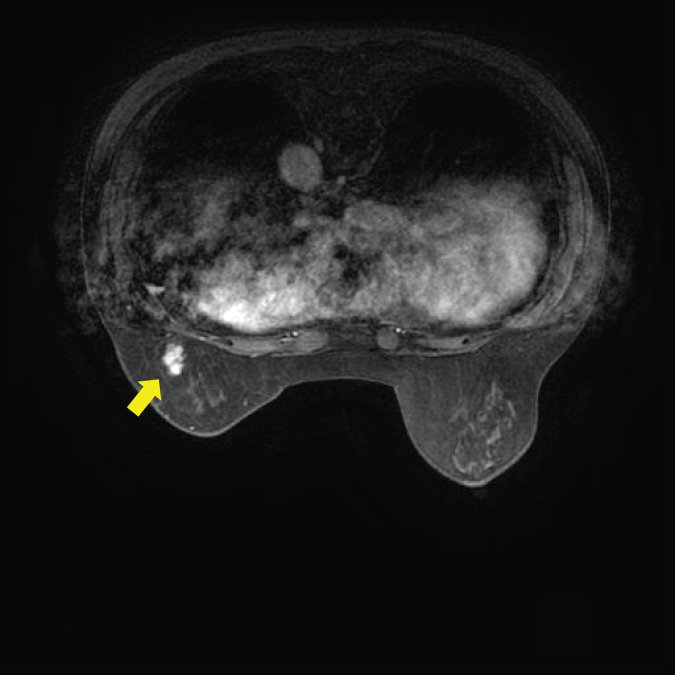 Fig. 2
Fig. 2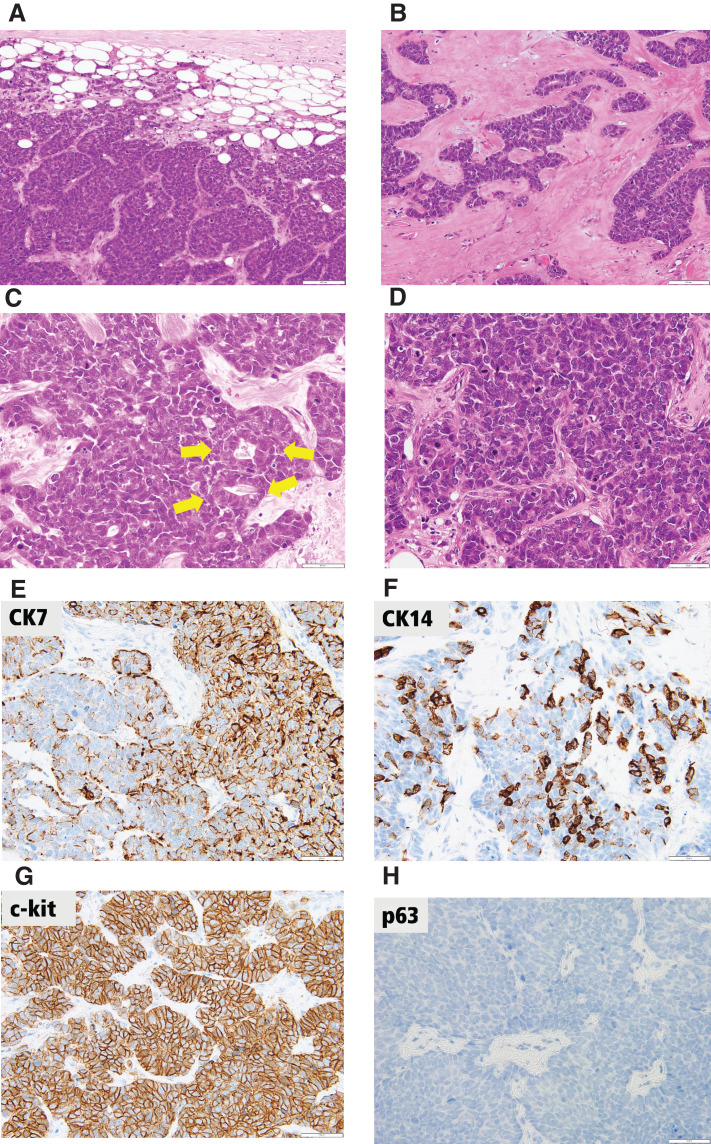 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalivary Gland Tumors Diagnosis and Treatment · Breast Lesions and Carcinomas · Vascular Tumors and Angiosarcomas
Abbreviations
AdCC adenoid cystic carcinoma C-AdCC classic adenoid cystic carcinoma CA15-3 cancer antigen 15-3 CEA carcinoembryonic antigen CK cytokeratin ER estrogen receptor GATA3 trans-acting T-cell-specific transcription factor HER2 human epidermal growth factor receptor type 2 INSM1 insulinoma-associated protein 1 PR progesterone receptor SB-AdCC solid–basaloid adenoid cystic carcinoma
INTRODUCTION
SB-AdCC is a rare and aggressive variant of AdCC of the breast. Furthermore, it is an extremely rare subtype of triple-negative breast cancer, accounting for <1% of all breast cancers.^1,2)^ It is considered as a variant of the more common classic AdCC (C-AdCC), which is known to have a good prognosis; however, SB-AdCC exhibits a more aggressive clinical behavior than C-AdCC, with a higher incidence of distant metastases. Shamir et al. reported that SB-AdCC cases showed nodal metastases (22%), distant metastases (33%), and poor response to neoadjuvant chemotherapy, with no pathological complete response observed in treated patients.^3)^ A high Ki-67 index (>30%) may be an adverse prognostic factor for metastasis. Although platinum- and anthracycline-containing regimens have demonstrated some efficacy,^1)^ no standardized treatment recommendations are available owing to the rarity of the disease. Furthermore, poor response to conventional chemotherapy underscores the need for alternative treatment strategies. We report here a case of SB-AdCC.
CASE PRESENTATION
Ten years ago, an 82-year-old woman underwent a partial mastectomy for a luminal HER2-type breast cancer located in the left upper inner quadrant. The pathological diagnosis was T1cN0M0, Stage I, invasive ductal carcinoma. The carcinoma expressed ER and HER2 but lacked PR expression. Subsequently, radiotherapy, anastrozole, and trastuzumab were administered during the postoperative period. Ten years later, she noticed another mass in the left breast, measuring approximately 10 mm in size. The mass was located in the lower outer quadrant of the left breast and had sufficient distance from the prior surgical scar. Left breast ultrasonography findings are depicted in Fig. 1. A needle biopsy was performed, detecting an unclassified carcinoma, which was identified as triple-negative breast cancer via histological examination. Breast MRI revealed a 17 × 8 × 8-mm irregularly enhanced mass with T2 hyperintensity (Fig. 2). No metastasis was noted in the lymph node on MRI or CT. The results for tumor markers CEA and CA15-3 were negative. As the histopathological type could not be identified through biopsy, surgery was performed first.
Ultrasonographic findings. Ultrasonography revealed an irregular mass in the outer region of the left breast, measuring 0.8 × 0.5 × 1.0 cm (yellow arrow). The nipple–tumor distance was 4.6 cm.
MRI findings. MRI revealed a 1.7-cm high-signal mass on DWI, which showed enhancement after contrast agent administration (yellow arrow).DWI, diffusion-weighted imaging
Mastectomy and sentinel lymph node biopsy were performed. As the sentinel lymph node biopsy results were negative, lymph node dissection was omitted. She was discharged from the hospital without postoperative complications on day 6. The excised specimen revealed a lesion composed of solid nests and trabeculae of basaloid cells with high nuclear-to-cytoplasmic ratios, which provided a dark-blue appearance. Glands containing ductal epithelial cells were occasionally detected. Dense collagenous stroma and focal myxohyaline matrix were present around the basaloid nests. Immunohistochemical staining revealed triple negativity with ER and PR non-expression and HER2 non-overexpression. The Ki-67 index was very high (approximately 80%). Luminal cell markers were expressed (CK7 patchy and c-kit diffuse), and basal cell markers were focally expressed (CK5/6 and CK14). Test results for myoepithelial markers (p40 and p63), GATA3 and neuroendocrine markers (chromogranin, synaptophysin, and INSM1) were all negative. Solid components account for more than 90% of the whole tumor. These findings were generally suggestive of the diagnosis of SB-AdCC (Fig. 3). The pathological diagnosis was T1cN0M0, Stage I, SB-AdCC as triple-negative breast cancer.
Pathological findings. (A) Basaloid cells composed of solid nests with geographic island patterns (H&E, original magnification ×200). (B) Trabecular growth pattern with myxohyaline stroma (H&E, original magnification ×200). (C) Glands comprising ductal epithelial cells are occasionally detected (yellow arrows) (H&E, original magnification ×400). (D) Basaloid neoplastic cells with hyperchromatic nuclei, inconspicuous nucleoli, and scant cytoplasm show prominent nuclear atypia and frequent mitotic figures (H&E, original magnification ×400). (E) CK7 expression is patchy and diffuse (original magnification ×400; scale bar at the lower right indicates 50 μm). (F) Basal cell marker CK14 expression is focal (original magnification ×400; scale bar at the lower right indicates 50 μm). (G) A luminal cell marker c-kit expresses diffusely (original magnification ×400; scale bar at the lower right indicates 50 μm). (H) Test result for myoepithelial cell marker p63 is negative (original magnification ×400; scale bar at the lower right indicates 50 μm).CK, cytokeratin; H&E, hematoxylin and eosin
SB-AdCC has a poor prognosis; therefore, we considered performing chemotherapy with anthracyclines or taxanes. However, owing to her advanced age, the side effects of such chemotherapy could have led to a decline in activities of daily living. Consequently, she underwent postoperative chemotherapy with tegafur–gimeracil–oteracil potassium. At 1 year postoperatively, she is recovering well without signs of metastasis.
DISCUSSION
AdCC is a rare type of cancer with histological characteristics of a biphasic tumor composed of epithelial–myoepithelial cells and has 3 main growth patterns: cribriform, tubular, and solid.^4)^ Regarding clinical behavior, compared with other breast carcinomas, AdCC is a slow-growing tumor and generally has an indolent clinical course despite the triple-negative status.^5)^ AdCC is a low-grade tumor with a favorable prognosis and a 5-year survival rate of 80%–89%.^6)^ In contrast to the favorable features of AdCC, SB-AdCC, although an AdCC variant, exhibits unfavorable features and prognosis. Although C-AdCC has favorable 5- and 10-year disease-free survival (DFS) rates of over 95% and 90%, respectively, SB-AdCC shows significantly reduced DFS rates. A previous study reported a median DFS of only 46.5 months for SB-AdCC, compared with 151.8 months for C-AdCC.^1)^ SB-AdCC should be differentiated from small cell carcinoma, Merkel cell carcinoma of the skin, and invasive ductal carcinoma of basal-like subtype. Our case demonstrated characteristic histologic features. Immunohistochemically, the lesion displayed a triple-negative status, a high Ki-67 index, and negativity for neuroendocrine markers. For accurate diagnosis of breast AdCC, especially for SB-AdCC, molecular pathology is becoming increasingly important. To detect MYB activation, molecular testing for gene rearrangements, amplifications, and enhancer hijacking is recommended. Furthermore, molecular analyses of other gene abnormalities, such as NOTCH pathway gene mutations and chromatin remodeling gene mutations, are needed. Unfortunately, we were unable to perform molecular analysis or immunohistochemical staining for MYB protein at our facility.
Tegafur–gimeracil–oteracil potassium is an oral fluoropyrimidine chemotherapy drug combination that has demonstrated potential in treating recurrent triple-negative breast cancer; however, it is not a standard 1st-line treatment in new primary triple-negative breast cancer.^7)^ Inoue et al. reported that the tegafur–gimeracil–oteracil potassium combination is feasible as add-on therapy in Japanese patients with triple-negative breast cancer following neoadjuvant or adjuvant chemotherapy.^8)^ This report indicates that adding tegafur–gimeracil–oteracil to anthracycline- or taxane-based therapy as adjuvant chemotherapy resulted in prolonged relapse-free survival and overall survival. We referred to tegafur–gimeracil–oteracil add-on therapy reported by Inoue et al. This case involved an elderly patient, making it difficult to use conventional chemotherapy due to its strong side effects. However, since SB-AdCC has high malignancy, we considered administering some form of adjuvant chemotherapy. Based on the report, we decided that tegafur–gimeracil–oteracil has a partial effect. The regimen administered as adjuvant therapy was 40 mg twice daily, in the morning and evening, for 14 consecutive days, followed by 7 days of rest. The recommended dose calculated based on the body surface area for this case was 50 mg. However, due to concerns about side effects, the dosage was reduced by 1 level. Adjuvant therapy was performed for 1 year without side effects.
CONCLUSIONS
We reported a case of SB-AdCC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Grabenstetter A, Brogi E, Zhang H, et al. Solid-basaloid variant of adenoid cystic carcinoma of the breast with near complete response to neoadjuvant chemotherapy. NPJ Breast Cancer 2022; 8: 93.35953528 10.1038/s 41523-022-00469-z PMC 9372162 · doi ↗ · pubmed ↗
- 2Ji J, Zhang F, Duan F, et al. Distinct clinicopathological and genomic features in solid and basaloid adenoid cystic carcinoma of the breast. Sci Rep 2022; 12: 8504.35590093 10.1038/s 41598-022-12583-w PMC 9120443 · doi ↗ · pubmed ↗
- 3Shamir ER, Bean GR, Schwartz CJ, et al. Solid-basaloid adenoid cystic carcinoma of the breast: an aggressive subtype enriched for notch pathway and chromatin modifier mutations with MYB overexpression. Mod Pathol 2023; 36: 100324.37660928 10.1016/j.modpat.2023.100324 · doi ↗ · pubmed ↗
- 4Moskaluk CA. Adenoid cystic carcinoma: clinical and molecular features. Head Neck Pathol 2013; 7: 17–22.23463073 10.1007/s 12105-013-0426-3PMC 3597152 · doi ↗ · pubmed ↗
- 5Miyai K, Schwartz MR, Divatia MK, et al. Adenoid cystic carcinoma of breast: recent advances. World J Clin Cases 2014; 2: 732–41.25516849 10.12998/wjcc.v 2.i 12.732PMC 4266822 · doi ↗ · pubmed ↗
- 6Thomas DN, Asarian A, Xiao P. Adenoid cystic carcinoma of the breast. J Surg Case Rep 2019; 2019: rjy 355.30697408 10.1093/jscr/rjy 355PMC 6344919 · doi ↗ · pubmed ↗
- 7Takashima T, Mukai H, Hara F, et al. SELECT BC Study Group. Taxanes versus S-1 as the first-line chemotherapy for metastatic breast cancer (SELECT BC): an open-label, non-inferiority, randomised phase 3 trial. Lancet Oncol 2016; 17: 90–8.26617202 10.1016/S 1470-2045(15)00411-8 · doi ↗ · pubmed ↗
- 8Inoue K, Nagai SE, Saito T, et al. TS-1 add-on therapy in Japanese patients with triple-negative breast cancer after neoadjuvant or adjuvant chemotherapy: a feasibility study. Invest New Drugs 2020; 38: 140–7.31289984 10.1007/s 10637-019-00829-w PMC 6985043 · doi ↗ · pubmed ↗