Unlocking RAS: Finding the Right Combination Is the Key
Bjoern Papke, Channing J. Der

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
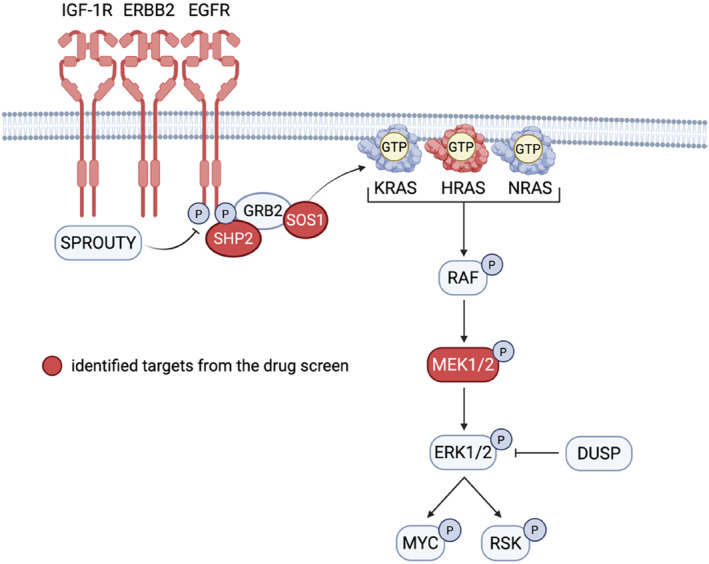 Figure 1
Figure 1- —National Cancer Institute10.13039/100000054
- —Pancreatic Cancer Action Network10.13039/100001784
- —U.S. Department of Defense10.13039/100000005
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Colorectal Cancer Treatments and Studies · Peptidase Inhibition and Analysis
The belief that RAS was “undruggable,” once etched in stone, was shattered with the first clinical approval of KRAS^G12C^ inhibitors in 2021 and 2022. Since then, numerous RAS inhibitors that target different oncogenic mutations, including pan‐RAS approaches, have entered clinical trials [1]. However, colorectal cancer (CRC) poses a significant therapeutic challenge for RAS inhibition due to robust feedback loops and compensatory receptor tyrosine kinase (RTK) activation, similar to resistance mechanisms previously observed in the early years of BRAF inhibitor clinical development [2, 3]. Consequently, combination therapy with EGFR inhibitors is essential to counteract these adaptive responses, an approach recently validated for KRAS^G12C^ inhibitors [4, 5]. Nevertheless, responses to the combination of KRAS^G12C^ inhibitors with EGFR antibodies remain incomplete, and resistance typically develops with a progression free survival of approximately 7 months [6].
In this issue of the United European Journal of Gastroenterology, Buchloh et al. investigate combination therapies for RAS inhibitor treatment specifically in rectal cancer (RC), which comprises one‐third of all colorectal cancer [7]. Notably, approximately half of RC harbor a RAS mutation, with 45% carrying KRAS mutations and 5% NRAS mutations (cBioPortal [MSK RC dataset]). The authors first to set out to investigate the clinical impact of RAS mutations on the patient's outcome after neoadjuvant therapy. In their Goettingen rectal cancer cohort (390 patients), they found that the disease‐free survival was significantly reduced in rectal cancer patients carrying KRAS^G12C^ and KRAS^G12V^ mutations compared to KRAS wild‐type patients.
Given the emergence of clinically approved KRAS^G12C^ inhibitors and the reduced survival associated with KRAS^G12C/V^ mutant RC, the authors turned to rectal cancer cell line models to investigate mechanisms of resistance and to identify effective combination strategies. In both model RC cell lines, SW1463 and SW837, they observed rapid adaptive resistance to RAS inhibition, consistent with previous findings in colon cancer. To systematically address this resistance, the authors performed a drug screen of 125 compounds in both cell lines. This drug screen identified eight candidate inhibitors that were effective in both models, targeting IGF‐1R, ERBB2/EGFR, MEK, PRMT1, SHP2, farnesyltransferase, SOS, and MDM2. Notably, the majority of these targeted either RTKs (ERBB2, EGFR, and IGF‐1R) or key signal components connecting RTKs with RAS (SOS1 and SHP2) and RAS effector signaling (MEK), highlighting recurrent vulnerabilities in RAS‐mutant contexts and underscoring the pivotal role of RTK‐RAS pathway reactivation in RC (Figure 1).
Subsequent combination studies using the approved KRAS^G12C^ inhibitor sotorasib, the pan‐KRAS inhibitor BI‐2865, and the clinical candidate multi‐RAS(ON) inhibitor daraxonrasib/RMC‐6236 together with the pan‐HER inhibitor neratinib demonstrated robust and consistent synergistical enhancement of proliferation inhibition across various assays and models including organoid cultures, further supporting the robustness of these combination approaches.
In conclusion, this study underscores the critical role of RTKs in RC and highlights that RAS inhibition alone is unlikely to be sufficient. Therefore, more effective combination strategies will be necessary to sensitize tumor cells and to overcome resistance.
Finally, the concept of the Goldilocks principle appears to apply to RTK inhibition as well: too little inhibition leads to rapid resistance, while excessive inhibition, such as that seen clinically with SHP2 and SOS inhibitors as pan‐RTK inhibitors, can result in adverse effects. However, we are only beginning to discover what “just perfect” means in terms of RAS‐RTK inhibition and which RTKs will play major roles.
Conflicts of Interest
C.J.D. is a consultant/advisory board member for AskY Therapeutics, Cullgen, Deciphera Pharmaceuticals, Mirati Therapeutics, Reactive Biosciences, Revolution Medicines and SHY Therapeutics. C.J.D. has received research funding support from Deciphera Pharmaceuticals, Mirati Therapeutics, Reactive Biosciences, Revolution Medicines, and SpringWorks Therapeutics. The other author declares no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1T. Isermann , C. Sers , C. J. Der , and B. Papke , “KRAS Inhibitors: Resistance Drivers and Combinatorial Strategies,” Trends in Cancer 11, no. 2 (2025): 91–116, 10.1016/j.trecan.2024.11.009.39732595 · doi ↗ · pubmed ↗
- 2R. B. Corcoran , H. Ebi , A. B. Turke , et al., “EGFR‐Mediated Reactivation of MAPK Signaling Contributes to Insensitivity of BRAF‐Mutant Colorectal Cancers to RAF Inhibition With Vemurafenib,” Cancer Discovery 2, no. 3 (2012): 227–235, 10.1158/2159-8290.CD-11-0341.22448344 PMC 3308191 · doi ↗ · pubmed ↗
- 3A. Prahallad , C. Sun , S. Huang , et al., “Unresponsiveness of Colon Cancer to BRAF(V 600E) Inhibition Through Feedback Activation of EGFR,” Nature 483, no. 7387 (2012): 100–103, 10.1038/nature 10868.22281684 · doi ↗ · pubmed ↗
- 4R. Yaeger , N. V. Uboha , M. S. Pelster , et al., “Efficacy and Safety of Adagrasib Plus Cetuximab in Patients With KRASG 12C‐Mutated Metastatic Colorectal Cancer,” Cancer Discovery 14, no. 6 (2024): 982–983, 10.1158/2159-8290.CD-24-0217.38587856 PMC 11152245 · doi ↗ · pubmed ↗
- 5M. G. Fakih , L. Salvatore , T. Esaki , et al., “Sotorasib Plus Panitumumab in Refractory Colorectal Cancer With Mutated KRAS G 12C,” New England Journal of Medicine 389, no. 23 (2023): 2125–2139, 10.1056/NEJ Moa 2308795.37870968 · doi ↗ · pubmed ↗
- 6R. Yaeger , J. Weiss , M. S. Pelster , et al., “Adagrasib With or Without Cetuximab in Colorectal Cancer With Mutated KRAS G 12C,” New England Journal of Medicine 388, no. 1 (2022): 44–54, 10.1056/NEJ Moa 2212419.36546659 PMC 9908297 · doi ↗ · pubmed ↗
- 7J. Buchloh , M. Spitzner , H. Zimmermann , et al., “Pan‐ERBB Inhibitors Synergize With KRAS Inhibitors in Rectal Cancer,” United European Gastroenterology Journal (2025): ueg 2.70086, 10.1002/ueg 2.70086.PMC 1260599140956140 · doi ↗ · pubmed ↗