Enhancing Equity in Access and Quality of Youth Out-of-School-Time Recreational Activities: Perspectives from Primary Caregivers and Parents in Under-resourced Urban Communities Using Semi-structured Interviews
Jaime La Charite, Mercedes Santoro, Cindy Flores, Alejandra Hurtado, Meachelle Lum, Yelba Castellon-Lopez, Rebecca Dudovitz

TL;DR
This study explores how caregivers in under-resourced urban communities perceive barriers and opportunities for youth recreational activities, aiming to improve equity and quality.
Contribution
The study provides new qualitative insights from caregivers in marginalized communities on factors influencing youth activity participation and offers actionable recommendations for improving access and quality.
Findings
Caregivers are highly motivated to enroll children in activities for lifelong wellbeing but face barriers like lack of awareness and enrollment challenges.
High-quality activities are defined by safety, inclusivity, and enjoyment, with recommendations for outreach, cost reduction, and staff training to improve access.
Caregivers emphasized structural investments and family engagement as essential for equitable and effective youth programming.
Abstract
Out-of-school-time recreational activities are linked to numerous socioemotional, health, and academic benefits for children. Racial and income disparities in participation persist, yet there is a lack of qualitative studies eliciting the experiences and input of primary caregivers to improve equitable access to high-quality recreational activities in marginalized communities. This study explores caregiver perceptions of the factors influencing motivations to enroll their child in activities, barriers to participation, how caregivers define quality programming, and caregiver recommendations to improve activity access and quality within under-resourced communities. We recruited primary caregivers of children aged 6–17 from under-resourced communities in an urban county by purposive sampling through urban parks and recreation and community organizations. We conducted semi-structured…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
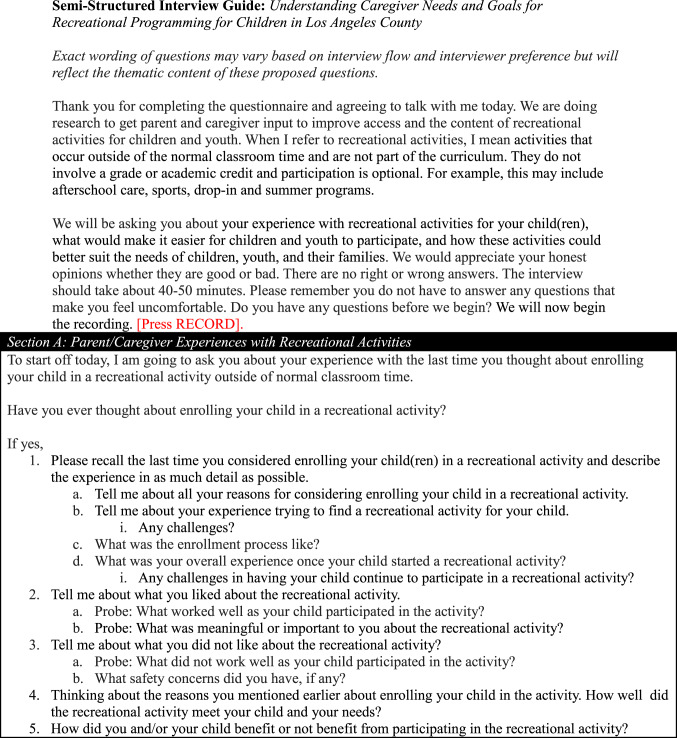 Figure 1
Figure 1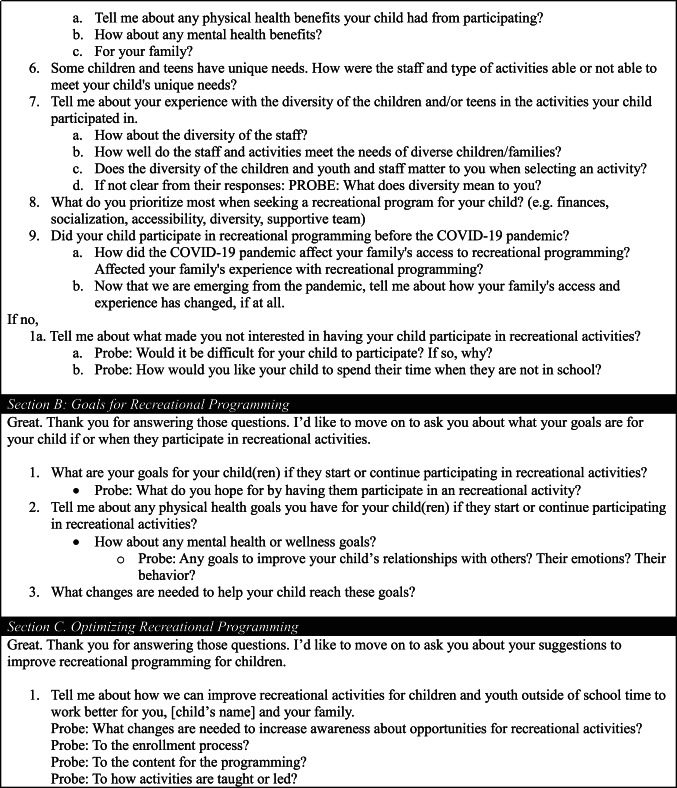 Figure 2
Figure 2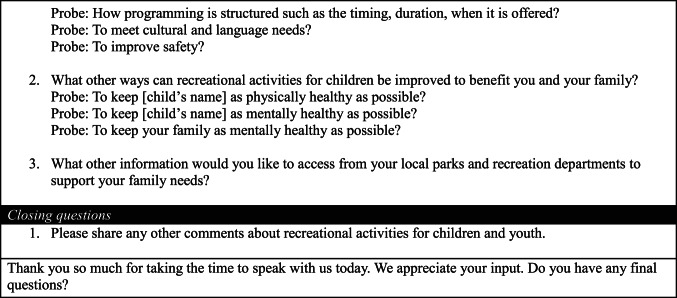 Figure 3
Figure 3- —Los Angeles Dodgers Foundation
- —http://dx.doi.org/10.13039/100006108National Center for Advancing Translational Sciences
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsYouth Development and Social Support · Urban Green Space and Health · Inclusion and Disability in Education and Sport
Introduction
Out-of-school time activities (“activities”) are optional, adult-supervised enrichment opportunities outside school time, including sports, arts, academic clubs, community programs, and summer experiences (Naff et al., 2024). Participation correlates with better academics and physical and socioemotional health, with benefits potentially extending into adulthood (“Committee on Summertime,” 2019; Easterlin et al., 2019; Gleeson et al., 2011; La Charite et al., 2023). Mechanisms linking activities to health outcomes include supportive adult and peer relationships, reduced screen time, skill development, and regular exercise (Easterlin et al., 2019; Gleeson et al., 2011; Guilmette et al., 2019; Mahoney et al., 2002; Oberle et al., 2020). Youth of color, immigrant youth, and youth from lower-income households may gain more benefits from participation than their more advantaged peers (Heath et al., 2022; Phillips et al., 2021).
Activity participation disparities exist at the intersection of race, ethnicity, and class within under-resourced communities. Children who identify as Black and/or Latinx, along with children in low-income households, report lower participation and higher unmet demand; nationally, 63% of families who identify as Black in the lowest income bracket reported participation versus 88% in the highest bracket (Afterschool Alliance, 2021, 2022; La Charite et al., 2023). These disparities coincide with community factors. Racially segregated neighborhoods - stemming from discriminatory policies - and neighborhood income affect resource distribution and the quality of amenities (America & Becoming, 2001; McKenzie et al., 2014; Schwartz et al., 2022). Community amenity availability correlates with activity participation (Donnelly et al., 2019; McKenzie et al., 2014).
Most research on disparities relies on non-peer-reviewed national caregiver surveys, revealing access barriers like cost, inconvenient locations and hours, transportation issues, limited program space, and cultural isolation (Afterschool Alliance, 2021). These surveys did not identify a lack of perceived benefit or quality as limiting participation (Afterschool Alliance, 2022). Existing qualitative studies with caregivers focused on specific activities or parental involvement (Duerden et al., 2013; Fisher et al., 2022; Ju et al., 2020). No known qualitative studies explore caregiver perspectives on improving youth engagement in predominantly Black and Latinx, under-resourced communities. Qualitative interviews enable caregivers to detail their experiences with youth programming and suggest ways to create a more accessible, quality, and equitable activity system that may not have been captured in surveys (Smith et al., 1995).
We conducted semi-structured interviews with caregivers of children ages 6–17 in under-resourced urban areas with predominantly Latinx and Black families. Our goal was to elucidate caregiver insights for redesigning out-of-school time activities to optimize access, quality, and equity. To that end, we sought to describe primary caregiver (1) motivations to have their child participate in activities, (2) perceptions of participation barriers and recommendations to reduce barriers, and (3) perceptions of activity quality and recommendations to enhance quality. For aims one and two, we interviewed caregivers whose children were engaged and not engaged in activities to capture perspectives along varying degrees of engagement.
Methods
Research Team
Personal Characteristics
Four bilingual (English/Spanish) female research assistants (RAs) with Bachelor’s or Master of Public Health degrees conducted the interviews. They attended two two-hour trainings on qualitative research methods, interview techniques, and content analysis. The first author, bilingual and experienced in qualitative methods, reviewed the transcripts and provided feedback.
Relationship with Participants
Participants had no prior relationships with the study team. During recruitment and consent, RAs explained the study’s goal of improving recreational activities. Linguistic and cultural congruence existed between RAs and Latinx participants; however, none of the RAs identified as Black or African American.
Study Design
Methodological Orientation and Theory
Our study was informed by Education Training Research (ETR)’s Health Equity Framework’s four domains (Systems of Power, Relationships and Networks, Individual Factors, and Physiological Pathways) (ETR, 2024). We conceptualized that policies, processes, and practices drive differential activity access (Systems of Power), influence family and peer relationships (Relationships and Networks), promote the development of health attitudes, skills, and behaviors (Individual Factors), and impact physical, cognitive, and psychological health (Physiologic Pathways). These concepts informed the development of our interview guide.
We conducted qualitative semi-structured interviews to identify caregivers’ perspectives about equity and quality. Semi-structured interviews are appropriate for narrating diverse caregiver perspectives (Kallio et al., 2016). We followed published steps to develop our interview guide: identifying prerequisites for semi-structured interviews, retrieving and using previous knowledge, formulating a preliminary guide, pilot testing, and presenting the guide (Kallio et al., 2016). Additional diversity and inclusion questions were added after the first two interviews. Our interview guide (Table 1) included questions to elucidate caregiver suggestions to achieve equity in activity access and quality (Systems of Power) and caregiver perceptions of how activity participation influences relationships, behaviors, and health (Relationships,* Individual Factors*,* Physiologic Pathways*).
Table 1. Interview guide
We used qualitative descriptive methodology and qualitative content analysis to describe the lived experiences of caregivers as they considered and navigated out-of-school-time programming to inform policy and program development rather than for theory development or meaning-making (Turale, 2020). Themes were data-driven rather than fit to a pre-existing theory.
Participant Selection
We prioritized caregivers from historically disinvested, predominantly Black and Latinx communities in East and South Los Angeles (LA) County. We sought to recruit families engaged and not engaged in activities to capture diverse perspectives. We used purposeful sampling recruiting across four categories: community park events in (1) East LA County and (2) South LA County, and community-based organizations engaging (3) Latinx residents in East LA County and (4) Black residents in South LA County. Community organizations received stipends to communicate study information to clients via email, social media, and community radio. RAs distributed recruitment flyers face-to-face during park events. Interested participants contacted the study team for eligibility screening.
Eligible participants were caregivers (18+) of children aged 6–17 living in East or South LA and accessible by email or phone. We interviewed 34 of 44 eligible caregivers (77%) until thematic saturation was reached (see Data Analysis).
Setting
Community Context and Partnership
East and South LA County is home to 2 million residents – over 300,000 of whom are Black and nearly 1 million Latinx (Klein, 2001). These regions make up 23% of the county’s population and have high concentrations of residents identifying as Latinx or Black (South LA: 62% Latinx, 31% Black; East LA: 73% Latinx, 3% Black), foreign-born (36–40%), and report high poverty rates (16–30% vs. 15% countywide) (Los Angeles County, 2014; Ong and Firestine et al., 2008). We focused on areas that experience concentrated poverty, limited park access, and lower scores on the Equity Index, which measures poverty and social determinants of health (County of Los Angeles, California State Parks, 2024; Galperin, 2021; Ong et al., 2008). We suspect findings are transferable outside LA as other US urban environments similarly face disparities in green space access and have concentrated populations of Black and Latinx and low-income residents (Frey, 2021; Kephart, Lindsay, 2022).
In LA County, urban parks and recreation service providers, schools, and community organizations deliver activities. This study focused on general caregiver perceptions and recommendations rather than feedback directed at specific local organizations, increasing the transferability of the findings. Community-Partnered Participatory Research principles guided the study, engaging parks and recreation staff in formulating aims, developing an interview guide, recruiting participants, preparing the manuscript, and disseminating findings (Jones & Wells, 2007).
Data Collection and Setting
Participants completed a 15-minute web-based (or phone) pre-interview survey on demographics, health, and activity history. The survey was adapted from a prior study with Latinx community members with lower educational attainment (DeCamp et al., 2019). We included three questions from the National Survey of Children’s Health asking caregivers to rate their child’s physical and mental health and indicate if their child had a diagnosed medical condition (yes/no), since we were interested in including caregivers of children with and without health conditions (CAHMI, 2025).
A RA conducted a 45-minute semi-structured interview in English or Spanish with one participant by phone or Zoom (four requested Zoom). Interviews took place in a private location outside of the earshot of others. The interview guide (Table 1) covered motivations, experiences, barriers, facilitators, and recommendations for youth activities. Probes clarified and elaborated on responses. Interviews were audio-recorded, de-identified, and transcribed. Participants received a $50 gift card.
Data Analysis
To describe the characteristics of our sample, we calculated frequencies and percentages for demographic items on the pre-interview survey stratified by language.
Transcripts were analyzed in five steps: (1) familiarization, (2) initial coding, (3) searching for themes, (4) refining themes, and (5) theme definition (Braun & Clarke, 2006). Transcripts were analyzed using Dedoose (v9.0.107) (Dedoose, 2024).
The coding team, consisting of four RAs supervised by the first author (JL), independently reviewed five transcripts, developed separate codebooks, and reconciled them through discussion. Two RAs then initially double-coded transcripts, and JL resolved discrepancies. This process continued until an interrater reliability score (kappa) of > 0.90 in Dedoose Training Center was achieved, after which transcripts were coded without a second reviewer. The four RAs and JL held weekly team meetings to address coding questions. Interviews and coding continued until thematic saturation, when no new information or codes emerged, was attained for both English and Spanish transcripts (Lincoln & Guba, 1985).
Following our inductive approach, we allowed themes to emerge from the data rather than fitting the data to a coding frame or pre-existing theory (Braun & Clarke, 2006). The Health Equity Framework informed the interview guide but did not drive data analysis. The coding team used Dedoose (Tong et al., 2007) visualization tools to review codes and organize themes (Braun & Clarke, 2006). They used group consensus to reconcile themes and reviewed them for internal consistency and distinctiveness (Braun & Clarke, 2006).
We used the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines for reporting (Tong et al., 2007). IRB approval was obtained (IRB#23–000231).
Results
We conducted 34 interviews (17 in English and 17 in Spanish). Sample demographics from the pre-interview survey are in Table 2. The analysis yielded a key theme for each study aim. Subthemes emerged to describe caregiver recommendations to improve motivation, access, and quality programming. Quotes are in-text and in Appendix Tables 5, 6 and 7. Tables 3 and 4 summarize caregiver recommendations for activity providers.
Table 2. Characteristics of interviewed participants stratified by preferred LanguageEnglish(N = 16*)Spanish(N = 17) Child Demographics No. of children in household 1 child6 (35%)4 (24%) 2 children7 (41%)8 (47%) 3 children2 (12%)4 (24%) ≥ 4 children1 (6%)1 (6%) Missing1 (6%)0Child Ages 6–8 years5 (29%)2 (12%) 9–12 years5 (29%)7 (41%) 13–17 years6 (35%)8 (47%) Missing1 (6%)0Child Genders Female3 (18%)4 (24%) Male13 (76%)13 (76%) Nonbinary0 (0%)0 (0%) Missing1 (6%)0Child Physical Health Households with a child with fair or poor physical health0 (0%)2 (12%)Child Mental Health Households with a child with fair or poor mental health2 (12%)2 (12%)Child Diagnosed Condition Households with a child with a diagnosed health condition7 (41%)8 (47%)Child Ever Participated in Out-of-School Time Activity Ever16 (94%)14 (82%)Child Participated in Out-of-School Time Activity in Past 3 Months Ever15 (88%)8 (47%) Caregiver Demographics Caregiver Gender Male4 (24%)2 (12%) Female12 (71%)15 (88%) Missing1 (6%)0Caregiver Age 18–290 (0.0%)2 (12%) 30–398 (47%)3 (18%) 40–497 (41%)9 (53%) 50–591 (6%)3 (18%) Missing1 (6%)0Country of Birth USA14 (82%)2 (12%) Mexico1 (6%)11 (65%) Central America1 (6%)4 (24%) Missing1 (6%)0Education < High School0 (0%)9 (53%) High School3 (18%)6 (35%) Some college4 (24%)0 (0%) 4-year university8 (47%)2 (12%) Missing1 (6%)0 Household Demographics Annual Family Income < 20,000–50,0007 (41%)10 (59%) >$50,0007 (41%)1 (6%) Missing1 (6%)0Public Benefits Enrolled in Medicaid, WIC, or SNAP12 (71%)15 (88%)Household Car No car in household3 (18%)2 (12%)One participant in the English-speaking category did not complete the pre-interview survey No.* Number
Table 3. Action statements to improve equitable access to out-of-school time programming based on caregiver interviewsAction Statements for Community OrganizationsOutreachCaregivers recommend comprehensive outreach strategies.Caregivers suggested using email listservs, mailers, social media profiles, flyer distribution through schools and parks, and community networking via churches and local businesses. They also recommended a consistent physical and online location where all local organizations could post their activities. Enough information about the activity and its benefits should be provided to help caregivers motivate their children to attend.Enrollment Caregivers recommend multiple easy-to-use ways to enroll in activities. Caregivers recommend refining the enrollment process by providing in-person, telephone, and digital registration options, simplifying application questions, and establishing help lines (via internet portal, telephone number). It is important to caregivers that organizations are accessible in terms of language, literacy, and communication.Accessibility Caregivers recommend investments to accommodate all interested families. Caregivers recommend sufficient program capacity to allow all interested children to enroll in programming. Families also wish for flexibility in program timing to account for caregivers’ working schedules. Some caregivers also suggest offering programming multiple times a year and incorporating more summer activities. Lastly, families want to see more neighborhood public pools and larger parks, so families do not need to travel far to participate in programming.Financial Caregivers recommend activity costs are low or free. Families recommend keeping programming low-cost or free as finances can often be a barrier to registration and participation. What is considered “low-cost” ranged from 50.Caregivers propose many suggestions, such as offering a waiver for caregivers who cannot afford associated costs, allowing payment plans, accepting payment on a lesson-by-lesson basis, developing a scholarship program, creating a system for caregivers to be able to borrow equipment and supplies, and making extra supplies/equipment are available. When an organization does offer financial supports, they should advertise openly so families are aware and can take advantage.To offset these costs to the organization, caregivers suggest organizations (1) find allies or sponsors who can provide uniforms, (2) host fundraisers, (3) partner with nonprofit organizations, (4) incorporate more volunteers, and (5) apply for grant funding.Beyond activities, caregivers also requested that these organizations offer referrals to other local community resources to address unmet basic needs.
Table 4. Action statements to improve the quality of out-of-school time programming based on caregiver interviewsAction Statements for Community OrganizationsSafetyInclusivityEnjoymentRecommendations to keep children safe during activities.Recommendations to promote a sense of belonging, celebrate diversity, reduce stigma, ensure language needs are met, and engage families as partners,Recommendations for diverse developmentally appropriate enjoyable activities.Structural InvestmentCaregivers recommend investing in sufficient supervision to protect their children from external factors, such as outside adults, drugs, and violence. Caregivers mention various strategies to improve supervision: on-site security guards, patrolling police officers, increased recreational staff, and sufficient lighting throughout the site. Comprehensive background checks of all staff and volunteersRequested multilingual forms and bilingual staff be available. Many families recommend culturally based activities that teach the community and their children about their cultural heritage.Caregivers of children with special needs (e.g. autism, ADHD) expressed the need for programming that can accommodate the developmental needs of their children.Caregivers mentioned activities such as: karate, science, technology, engineering and math (STEM) activities, dance, music lessons, life skills workshops, art, and many more. Caregivers express the importance of diversity in programming to stimulate children’s different interests.Staff and Volunteer TrainingCaregivers recommend staff training on injury prevention and management, conflict resolution, and rules of the sport.Caregivers recommend staff training on child development, supporting youth with mental and behavioral health conditions, and for children with historically marginalized communities.Caregivers suggested offering training on positive coaching strategies.Family-centered Approach to Activities and EngagementA community advisory board of caregivers to alert staff about safety concernsCaregivers recommend creating a caregiver/parent advisory board and getting input from families in the community about programming to improve service delivery.Caregivers also requested processes to facilitate communication with activity leadership about their child’s needs.Caregivers appreciate activities where multiple family members and children of different ages can participate together, such as “Mommy and Me” classes or allowing siblings to participate together. This would help families reduce the need for childcare and create bonding opportunities for families.
Aim 1: Motivations
Key Theme
Caregivers were highly motivated, believing activities facilitated lifelong healthy living and well-being for children, families, and communities. Caregivers believed activities promoted a child’s physical and socioemotional health and prepared them for future life stages. One caregiver shared, “I hope they develop a good healthy routine… so they look for that sport or exercise as they grow up.” They noted that activities provided space for physical activity and socioemotional skill building, such as teamwork and emotional regulation, while combating unhealthy habits like excessive screen time, substance use, and engaging in community violence. Caregivers felt youth participation improved family dynamics, reduced caregiver stress, and fostered community. One caregiver remarked, “The after-school program works wonderfully… being a single mom,* that helps take pressure off me.*” Activities helped caregivers build friendships, strengthen family bonds, and encourage gratitude and a desire to give back to the community.
Key Recommendations
More information about activities and their benefits may motivate families. One caregiver described, “I would like more information about the activities… if we know more [we can] better motivate the parents to take their children to activities.”
Aim 2: Barriers: Opportunities for Access Equity
Key Theme
Caregivers identified barriers to youth activity participation while recognizing opportunities for equitable access. The main barriers identified included a (1) lack of awareness, (2) enrollment challenges and accessing activities, and (3) financial obstacles.
- Lack of Awareness.
Some families lacked time or the knowledge to find suitable activities. One caregiver explained,Parents who are not in this area or do not have time to go to the park were unaware. Many people… are surprised at the [low] amount of money and [good] care provided to the children and they’re like,* ‘I didn’t even know about this. And they sign up*.
- (2)Enrollment and Access Challenges
Challenges included exclusive online enrollment and insufficient space for all interested children. One caregiver mentioned, “my daughter plays softball,* but if there’s not enough girls*,* we won’t build the team. If there’s not a coach*,* we will not build the team. I have to find another sport for her*.” Some families traveled outside their community for specialized activities like swimming, and science, technology, engineering, and math (STEM) programs.
- (3)Financial Obstacles
Financial burdens, including costs related to registration, uniform, supplies, equipment, snacks, and travel expenses, deterred families. One caregiver shared, “I had to pay [registration],* buy a uniform*,* and do many things*,* and I decided not to do it because I didn’t work*.”
Key recommendations
Parents proposed three recommendations for equitable access: (1) broad outreach using diverse strategies, (2) easy enrollment with accessible activities, and (3) low financial barriers
- Broad Outreach Using Diverse Strategies
Caregivers recommended broad outreach using diverse strategies (e.g., emails, social media, banners, flyers, commercials) through multiple channels (e.g., parks, schools, churches) and a centralized physical and online hub for activity information across organizations.
- (2)Easy Enrollment with Accessible Activities
Caregivers suggested multiple enrollment options (e.g., in-person, phone, online) with sufficient capacity for all youth to enroll in nearby activities. They recommended help lines, language-accessible low-literacy registration forms, and flexible drop-in options without prior registration required. Caregivers stressed that all children, especially those in minoritized communities, children with special needs, and girls in sports, should have equitable access to activities year-round. This includes offering diverse activities, sufficient space, and infrastructure (e.g., pools, park space) within these communities. One caregiver shared, “I live in a predominantly Black community… A lot of us don’t know how to swim,* and swimming can be life-saving. Every child should have the opportunity… the nearest pool is over 20 minutes away*.”
- (3)Low Financial Barriers
According to caregivers, low financial barriers would increase participation. One caregiver described, “It was $10 a week for the summer program… It was such a lifesaver.” Caregivers recommended reducing registration costs, offering registration waivers, scholarships, installment payments, lesson-by-lesson payments, free or rental supplies/equipment, uniform assistance, providing food, and offering transportation. To offset the costs accrued by the organization, caregivers suggested that organizations find sponsors/grants, host fundraisers, partner with nonprofits, and incorporate volunteers.
Aim 3: Definition of Quality Programs
Key Theme
High-quality activities consistently promote safety, inclusivity, and enjoyment. Caregivers reported varying levels of quality across their experiences with different activities, activity leaders, and organizations. Safety included protection from external (e.g., neighborhood violence) and internal (e.g., injuries) threats. Inclusivity meant fostering belonging for children from diverse backgrounds or with special needs. As one caregiver shared, “My son has Attention Deficit/Hyperactivity Disorder (ADHD). They make sure he is focused. They don’t mind repeating things… they know his brain works differently,* so they have him repeat it. They ensure he knows what’s going on*.” Enjoyment motivated engagement. Caregivers attributed enjoyment to the activity type, supportive and developmentally appropriate environments that built self-confidence, and opportunities to socialize and be in nature.
Key Recommendations
Caregivers recommended achieving consistent quality programming through (1) structural investments, (2) staff and volunteer training, and (3) family engagement.
- Structural Investment
Caregivers recommended investing in staff, infrastructure, and programming. Safety recommendations included hiring trained staff with background clearance, installing adequate lighting, providing onsite security, and arranging escorts for families. One caregiver requested, “Policemen will walk with them…through certain dangerous blocks.” For inclusivity, caregivers proposed supportive programming for underrepresented youth, such as sports for girls, activities accommodating children with physical, behavioral, or developmental needs, culturally relevant activities, language accessibility, and stigma reduction initiatives, noting stigma around water sports within the Black community. Lastly, caregivers recommended funding various developmentally appropriate and enjoyable activities to encourage engagement.
- (2)Staff and Volunteer Training
Caregivers recommended training for staff and volunteers. Many observed inconsistencies in instruction quality, especially among volunteers. A volunteer coach shared, “There should be more training for volunteer coaches because they just send us out there [to],* figure it out*.” It was unclear whether volunteer leaders were driven by cost-cutting or community preference. While some valued volunteers to reduce costs and increase community participation, others felt it contributed to dropouts. Suggested training topics included injury prevention and management, sports rules, child development, supporting youth mental health, caring for children from historically marginalized communities, and positive coaching strategies. Caregivers hoped this training would help staff and volunteers act as supportive, caring adults.
- (3) Family-centered Approach to Activities and Engagement
Caregivers requested opportunities for caregiver and sibling engagement. One caregiver proposed, “[Have] a community advisory board. We can be an asset,* right? Not only is our voice being heard*,* but we are helping you make this park better… so they can be part of the decision-making. For safety*,* with the board there are direct ears with the community of what’s going on*.” They also suggested processes for communication about children’s health and behavioral needs. Caregivers also appreciated options allowing siblings to participate together to simplify logistics and childcare.
Discussion
We found that caregivers living in under-resourced communities with many Black and/or Latinx identifying residents were motivated to engage their children in activities, recognizing the potential to help children develop essential skills, enhance their physical and mental health, and contribute to family and community well-being. Caregivers proposed practical strategies to promote equitable, high-quality programming, including broad outreach with diverse methods, easy enrollment with accessible activities, low financial barriers, structural investments, staff and volunteer training, and family engagement. Addressing structural causes of access and quality inequities may boost engagement and health equity.
Our findings align with the Health Equity Framework and build on earlier surveys. Caregivers recognized the impact of structural disinvestment as a key obstacle (Systems of Power Domain), linking disparities to missing infrastructure, such as pools and insufficient park space. Consistent with other studies, caregivers also highlighted cost as a primary barrier (Afterschool Alliance, 2021; Kelly Hinchcliffe, 2023). These interviews described other prohibitive costs like equipment and transportation. New barriers also emerged, including outreach and enrollment. Within the Individual Factor,* Physiological Pathways*,* and Relationships and Networks Domains*, caregivers noted skill development and physical health benefits, aligning with prior survey findings (Afterschool Alliance, 2021; Kelly Hinchcliffe, 2023). These interviews identified underexplored benefits, including mental health and family well-being, which are particularly relevant given the rise in youth and adult mental health challenges and is consistent with quantitative studies (La Charite et al., 2023; Parodi et al., 2022; Terlizzi & Zablotsky, Benjamin, 2024; Wilson & Dumornay, 2022).
Our study amplifies caregiver voices in under-resourced communities, offering their recommendations for improving access and quality equity in youth activities. Similarities to national surveys suggest broader applicability of our qualitative findings, while the narratives refine prior survey results (Afterschool Alliance, 2021; Kelly Hinchcliffe, 2023). Our findings can inform a caregiver-centered framework and survey tools for assessing ongoing activity access and quality, which was supported by the theme requesting family engagement. Researchers can evaluate whether caregiver-informed interventions boost engagement in health-promoting activities.
There are limitations to consider. Participants were recruited from one urban county in the United States, and eligibility was restricted to caregivers proficient in English or Spanish. The findings may be transferable to similar urban counties with a history of disinvestment and significant proportions of low-income Black and Latinx residents. We could not achieve cultural congruence for the participants who identified as Black or African American. Although we aimed to reach families that were and were not involved in activities, most families had current or past involvement, consistent with national data (La Charite et al., 2023).
The findings have implications for professionals and organizations who work with youth (e.g., activity providers, school nurses or counselors, pediatric clinicians). To facilitate child enrollment, youth-facing professionals can discuss activities as health-promoting tools, provide strategies to overcome barriers, and maintain up-to-date lists of low-barrier, high-quality activities in their area. Pediatric organizations may consider developing guidelines to inform training materials to ensure activity leaders are equipped to support children with special health needs.
Public agencies and activity organizations can collaborate to build a unified activity system, integrating tools for monitoring and continuous improvement to achieve equitable access and quality. Existing efforts include intermediary organizations aiding smaller organizations in offering activities and frameworks like Every Hour Counts for Measurement, Continuous Improvement, and Equitable Systems (Every Hour Counts, 2021). Our study emphasizes prioritizing family voices in these system-level improvements.
Policymakers and child health advocates should prioritize investments in infrastructure (parks, pools, lighting), reducing family costs, staff and volunteer training, and ensuring equitable access to specialized activities (e.g., swimming, STEM). This is important as the Coronavirus-2019 era emergency relief funding for afterschool programs ends. One caregiver noted, “It is important to build community pride in our children. If these services are not offered,* that sense of community will be lost; we need to invest in them*.”
Conclusion
Caregivers in under-resourced communities with high proportions of residents who identify as Black and/or Latinx are highly motivated to engage their children in out-of-school activities for skill development, relationship building, and overall well-being. They offer practical suggestions to enhance accessibility, quality, and equity in youth activities. Future efforts can assess whether these themes are consistent among different subpopulations or geographic regions and investigate whether increased caregiver input helps reduce disparities in activity participation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Afterschool Alliance (2021). America after 3pm for Black families and communities.https://afterschoolalliance.org/documents/AA 3PM-2020/AA 3PM-Black-Communities-2020-Fact-Sheet.pdf
- 2Afterschool Alliance (2022). Access to Afterschool Programs Remains a Challenge for Many Families. 1–5.
- 3America, & Becoming (2001). : Racial Trends and Their Consequences, Volume 1 (p. 9599). National Academies Press. 10.17226/9599
- 4County of Los Angeles, California State Parks (2024). Children with Easy Access to a Safe Place to Play. https://data.lacounty.gov/datasets/lacounty::children-with-easy-access-to-a-safe-place-to-play/explore?filters=ey J Qb GF 5X 1Bs YW Nl Ijpb N Dgu Niw 5N 119
- 5Dedoose (2024). https://www.dedoose.com/?gad_source=1&gclid=Cjw KC Ai Amfq 6Bh As Eiw AX 1js Z 7Hu Bp Bg LWA 9Vln Ileyk 5TA 3Bhp J_n Ekgr AJ Csql Je PCLEJI Rgt_A Ro CBKAQ Av D_Bw E.
- 6Duerden, M. D., Witt, P. A., & Harrist, C. J. (2013). The impact of parental involvement on a structured youth program experience: A qualitative inquiry. Journal of Youth Development, 8(3). 10.5195/jyd.2013.88
- 7ETR (2024). ETR’s Health Equity Framework. Advacing Health Equity. https://www.etr.org/about-us/health-equity-framework/
- 8Every Hour Counts. (2021). Putting data to work for young people: A framework for measurement, continuous improvement, and equitable systems. Wallace Foundation, 21. 10.59656/YD-OS 7384.001