Hemopericardium Following Norovirus Gastroenteritis in a Child: An Uncommon Presentation
Maha Hamed, Venkatachalam Karuppaswamy

TL;DR
A child developed a rare heart complication called hemopericardium after a norovirus stomach infection, highlighting the need for early detection and treatment.
Contribution
This is the first reported case of hemopericardium in a child linked to norovirus infection.
Findings
A 20-month-old child developed hemopericardium following norovirus gastroenteritis.
Pericardiocentesis successfully treated the condition, with full recovery observed.
The case suggests clinicians should consider cardiac complications in children with post-viral symptoms.
Abstract
Norovirus is a leading cause of acute gastroenteritis in children and is typically a self-limiting illness. Cardiac complications are exceptionally rare. To our knowledge, this is the first reported case of hemopericardium associated with norovirus infection in a child. We describe a 20-month-old previously healthy boy who presented with respiratory distress and fatigue two weeks after an episode of acute norovirus gastroenteritis. Investigations revealed severe anemia, elevated D-dimer, and a large hemorrhagic pericardial effusion with echocardiographic evidence of tamponade. Extensive workup excluded trauma, coagulopathy, autoimmune disease, and other infectious causes. The patient underwent urgent pericardiocentesis, draining 200 mL of hemorrhagic fluid. He improved rapidly and remained asymptomatic, with serial echocardiograms showing complete resolution of the effusion up to six…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
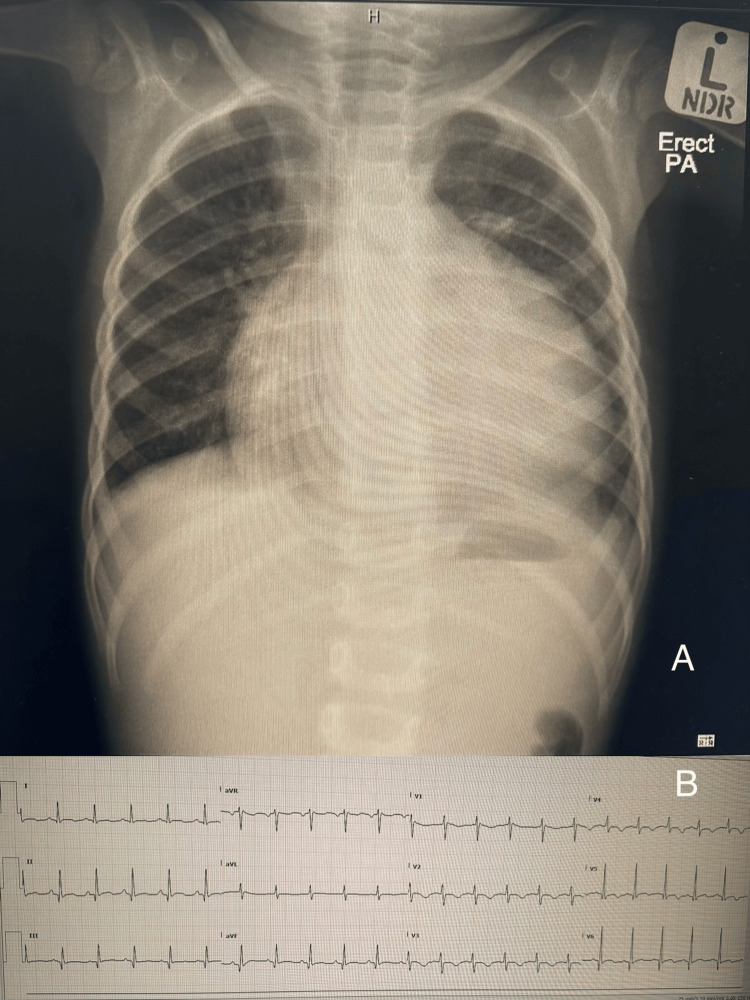 Figure 1
Figure 1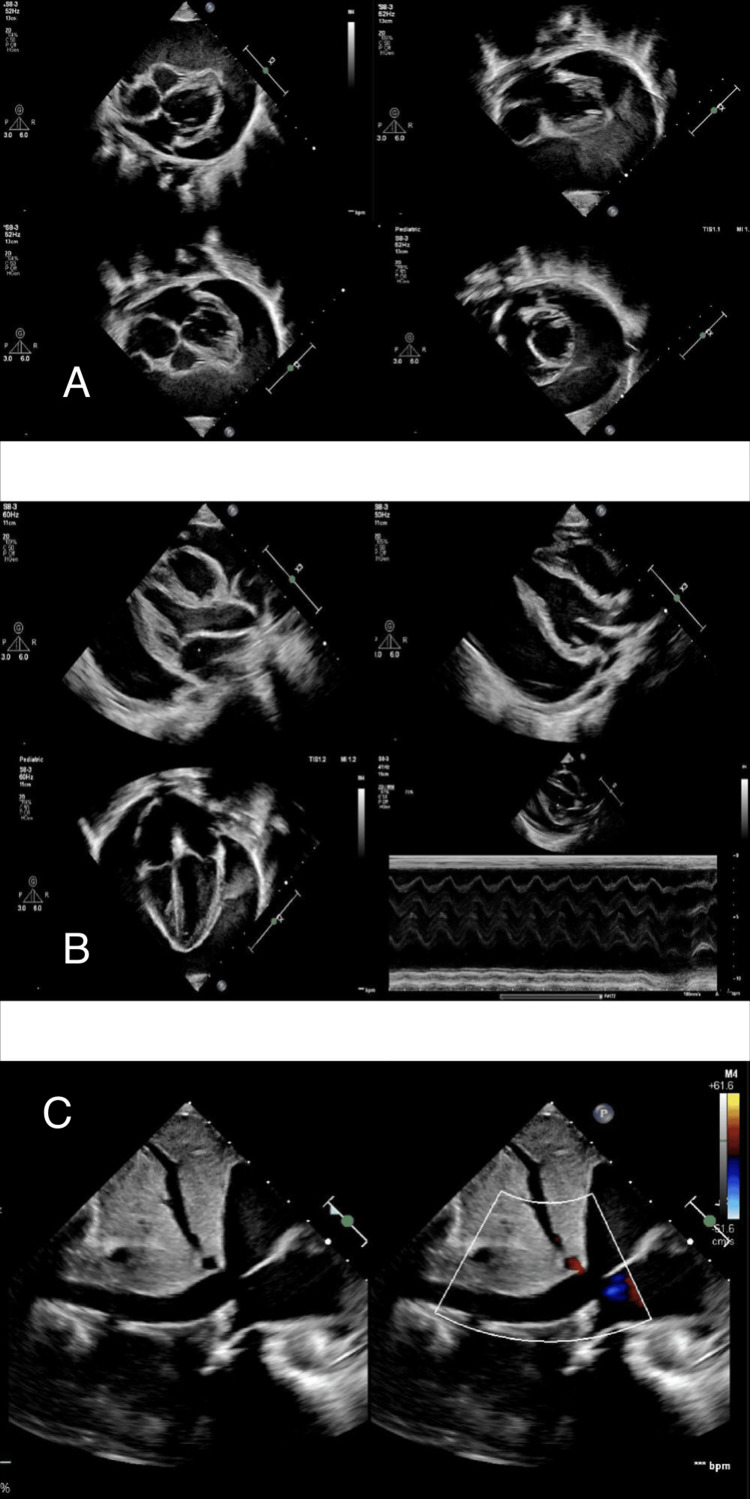 Figure 2
Figure 2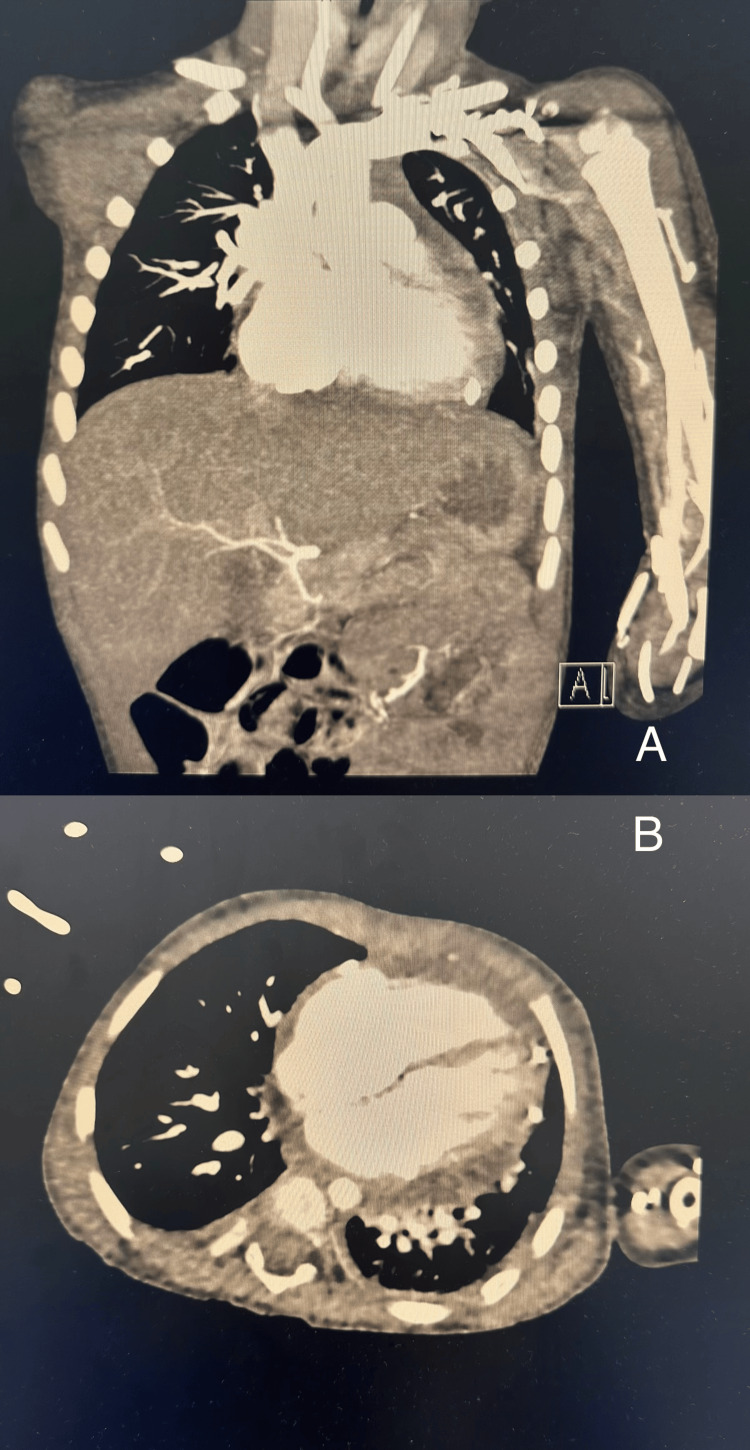 Figure 3
Figure 3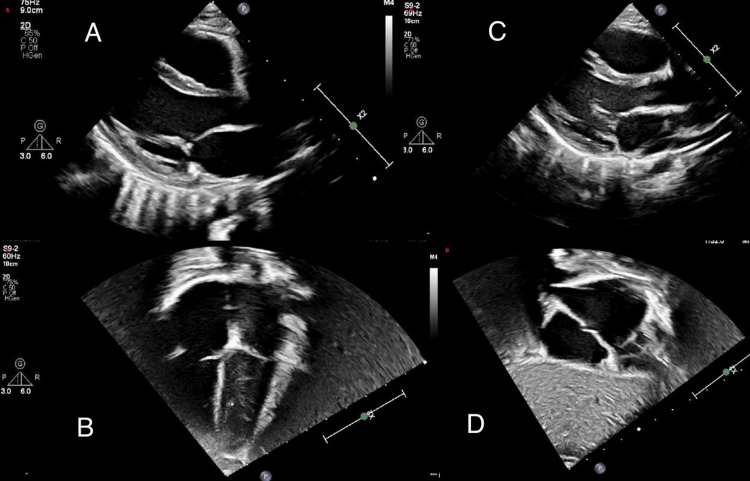 Figure 4
Figure 4| Parameter | Patient’s Value | Normal Range |
| Heart rate | 145/min | 80-130/min |
| Respiratory rate | 47/min | 20-30/min |
| Systolic blood pressure | 106 mmHg | 85-105 mmHg |
| Diastolic blood pressure | 75 mmHg | 35-65 mmHg |
| Parameter | Admission | Post-Pericardiocentesis | Follow-up (6 wks) | Normal Range* |
| Red blood cell count (RBC) | 2.93 ×10¹²/L | 4.56×10¹²/L | 4.51×10¹²/L | 3.8-5.2×10¹²/L |
| Hemoglobin | 6.8 g/dL | 11.5 g/dL | 11.1 g/dL | 11–13 g/dL |
| Hematocrit | 0.23 | 0.35 | 0.35 | 0.34-0.39 |
| Platelets | 643×10⁹/L | 620×10⁹/L | 237×10⁹/L | 150-450×10⁹/L |
| White blood cell count (WBC) | 10.8×10⁹/L | 7.4×10⁹/L | 8.44×10⁹/L | 6-17×10⁹/L |
| Reticulocyte (%) | 6.2% | 5.5% | 2.0% | 0.5-2.0% |
| Reticulocyte# | 201.2 ×10⁹/L | 180×10⁹/L | 60×10⁹/L | 25-75×10⁹/L |
| D-dimer | 11,520 ng/mL | 8,420 ng/mL | - | <500 ng/mL |
| Prothrombin time (PT) | 11.7 seconds | 11.4 seconds | 12.1 seconds | 10–14 seconds |
| Internationalized normal ratio (INR) | 1.07 | 1.04 | 1.11 | 0.9-1.2 |
| Activated partial thromboplastin time (APTT) | 26.3 seconds | 24.4 seconds | 25.6 seconds | 25-35 seconds |
| Fibrinogen | 2.91 g/L | 2.91 g/L | 2.97 g/L | 2-4 g/L |
| N-terminal pro-B-type natriuretic peptide (NT-proBNP) | 1,239 pg/mL | 1,108 pg/mL | - | <125 pg/mL |
| Troponin-T | 7.8 ng/L | 7.6 ng/L | - | <14 ng/L |
| C-reactive protein (CRP) | 9 mg/L | 6.1 mg/L | 1.9 mg/L | <5 mg/L |
| Erythrocyte sedimentation rate (ESR) | 81 mm/h | — | 18 mm/h | 0–10 mm/h |
| Parameter | Result | Normal Range* |
| Sodium | 140 mmol/L | 135–145 mmol/L |
| Potassium | 5.0 mmol/L | 3.5–5.5 mmol/L |
| Chloride | 105 mmol/L | 98–107 mmol/L |
| Carbon dioxide (CO₂) | 20 mmol/L | 20-28 mmol/L |
| Creatinine | 17 µmol/L | 18–35 µmol/L |
| Urea | 1.4 mmol/L | 1.8-6.4 mmol/L |
| Glucose (Random) | 5 mmol/L | 3.3-5.5 mmol/L |
| pH | 7.43 | 7.35-7.45 |
| Partial pressure of carbon dioxide (pCO₂) | 36.4 mmHg | 35-45 mmHg |
| Partial pressure of oxygen (pO₂) | 48.8 mmHg | 35-45 mmHg (venous) |
| Hydrocarbonate (HCO₃⁻) | 24 mmol/L | 22–26 mmol/L |
| Base excess | -0.2 | -2 to +2 mmol/L |
| Total hemoglobin (Hb) | 7.3 g/dL | 11-13 g/dL |
| Oxygen (O₂) Saturation | 83.5% | 75-80% (venous) |
| Parameter | Result | Normal Range* |
| Total Protein | 35.4 g/L | 35–50 g/L |
| Albumin | 28.0 g/L | 30–45 g/L |
| Globulin | 7.4 g/L | 20–35 g/L |
| Total Bilirubin | 4.5 mg/dL | 0.3–1.2 mg/dL |
| Direct Bilirubin | 3.2 mg/dL | 0–0.3 mg/dL |
| Alkaline Phosphatase | 229 U/L | 150–420 U/L |
| Aspartate aminotransferase (AST) | 23 U/L | 10–50 U/L |
| Alanine aminotransferase (ALT) | 22 U/L | 5–45 U/L |
| Carnitine profile | Normal | Normal |
| Acylcarnitine profile | Normal | Normal |
| Parameter | Result | Normal Range* |
| Phosphate | 1.68 mmol/L | 1.3-2.3 mmol/L |
| Calcium (total) | 2.27 mmol/L | 2.2-2.7 mmol/L |
| Magnesium | 0.85 mmol/L | 0.7-1.0 mmol/L |
| Lactate dehydrogenase (LDH) | 406 U/L | 120-300 U/L |
| Total creatine kinase (CK0 | 66 U/L | 24-170 U/L |
| Creatine kinase-myocardial band (CK-MB) | <1 U/L | <5 U/L |
| Triglycerides | 0.71 mmol/L | 0.3-1.1 mmol/L |
| Immunoglobulin G (IgG) | 7.78 g/L | 3.4-12.0 g/L |
| IgA | 0.95 g/L | 0.2 – 1.0 g/L |
| IgM | 1.15 g/L | 0.3 – 1.5 g/L |
| Ferritin | 66 µg/L | 7 – 140 µg/L |
| Interleukin-6 | 18.9 pg/mL | < 7 pg/mL |
| Procalcitonin | 0.16 ng/mL | < 0.5 ng/mL |
| Parameter | Result |
| Appearance | Bloody |
| Color | Bloody |
| Red blood cell (RBC) count | 3,320,000/µL |
| Nucleated cells | 5,640/µL |
| Neutrophils | 6% |
| Lymphocytes | 88% |
| Monocytes | 3% |
| Eosinophils | 3% |
| Albumin | 22 g/L |
| Protein | 51 g/L |
| Glucose | 3.0 mmol/L |
| Lactose dehydrogenase (LDH) | 686 U/L |
| Bacterial and viral polymerase chain reaction (PCR) | Negative |
| Fluid culture | Negative |
| Acid-fast bacilli (AFB) smear | Negative |
| AFB culture | Negative |
| Cytology | No abnormal cells detected |
| Parameter | Result |
| ANA | Normal |
| c-ANCA (PR3) | Normal |
| p-ANCA (MPO) | Normal |
| C3 | Normal |
| C4 | Normal |
| CMV IgG/IgM | Negative |
| EBV IgG/IgM | Negative |
| Mycoplasma IgM | Negative |
| Parvovirus B19 IgM/IgG | Negative |
| Quantiferon-TB | Negative |
| HIV Ag/Ab screen | Negative |
| SARS-CoV-2 total Ab | Negative |
| Test | Result |
| EBV PCR | Not detected |
| CMV PCR | Not detected |
| Respiratory PCR | Negative |
| Blood culture | Negative |
| Urine culture | Negative |
| Candida auris screening | Negative |
| VRE culture | Negative |
| Stool PCR (2 weeks prior) | Norovirus genogroup II detected |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral Infections and Immunology Research · Pericarditis and Cardiac Tamponade · Viral gastroenteritis research and epidemiology
Introduction
Hemopericardium refers to the accumulation of blood within the pericardial sac and may progress to cardiac tamponade, a life-threatening emergency [1]. In children, it is most commonly associated with trauma, cardiac surgery, neoplasms, or anticoagulant therapy [1,2]. Viral causes are extremely rare. Norovirus is among the most common causes of acute viral gastroenteritis in children worldwide, responsible for an estimated 200,000 pediatric hospitalizations annually, and is generally confined to the gastrointestinal tract [3]. Although typically perceived as a mild and self-limiting infection, rare extraintestinal complications such as myocarditis and pericarditis have been reported [4]. To our knowledge, hemopericardium associated with norovirus infection in children has not previously been described.
We present a unique case of hemopericardium following norovirus gastroenteritis in a 20-month-old child, representing the first reported pediatric case and expanding the clinical spectrum of this common viral infection. The patient demonstrated complete clinical recovery with resolution of the effusion on serial echocardiography up to six weeks post-discharge.
Case presentation
A 20‑month‑old previously healthy boy was brought to the emergency department with respiratory distress, fatigue, and reduced oral intake. Two weeks earlier, he had experienced an episode of acute viral gastroenteritis with vomiting, watery diarrhea, and fever, which resolved spontaneously. There was no history of trauma, bleeding disorders, or anticoagulant use.
On examination, he appeared pale and tachypneic with subcostal retractions. His vital signs were: heart rate (HR) 145/min, blood pressure (BP) 106/75 mmHg, respiratory rate (RR) 47/min, temperature 36.5°C, and peripheral oxygen saturation (SpO₂) 95% on room air (Table 1). Jugular venous distension and muffled heart sounds were noted, while the lungs were clear and the abdominal examination was unremarkable.
The investigations revealed severe microcytic anemia (hemoglobin 6.8 g/dL, decreased from 10 g/dL measured one week earlier at another private hospital) with reticulocytosis and thrombocytosis. The coagulation profile was normal apart from a markedly elevated D-dimer, consistent with active fibrinolysis and recent hemorrhage. Liver, renal, and coagulation studies, G6PD activity, hemoglobin electrophoresis, and blood film were otherwise unremarkable. Carnitine and acylcarnitine profiles were normal, excluding major metabolic defects or fatty acid oxidation disorders. Cardiac biomarkers showed elevated N-terminal pro-B-type natriuretic peptide (NT-proBNP) and troponin-T, indicating cardiac strain with mild myocardial injury. An extensive infectious, metabolic, and autoimmune workup was otherwise negative; however, stool polymerase chain reaction (PCR) performed two weeks earlier was positive for norovirus genogroup II, suggesting a potential viral trigger for the hemorrhagic pericardial effusion (Tables 2-8).
**Table 2: Key Laboratory Findings Over Time *Normal range for a 20-month-old child.
#Absolute reticulocyte count.
†Blood film, G6PD, and hemoglobin electrophoresis were normal at admission (not shown in
*Table 3: Electrolytes, Renal Function, and Venous Blood Gas Normal range for a 20-month-old child.
*Table 4: Liver Function and Metabolic Workup Normal range for a 20-month-old child.
*Table 5: Other Biochemical Markers Normal range for a 20-month-old child
Chest radiography demonstrated cardiomegaly, characterized by a globular cardiac silhouette and a cardiothoracic ratio of 0.58 (Figure 1). Electrocardiography revealed sinus tachycardia with low QRS voltage. Transthoracic echocardiography showed a large pericardial effusion measuring approximately 2.5 cm, with echogenic densities suggestive of hemopericardium and echocardiographic features of tamponade physiology (Figure 2). Chest computed tomography (CT) angiography confirmed the presence of a large pericardial effusion without vascular anomalies, with Hounsfield unit (HU) values ranging between 39 and 62, consistent with hemorrhagic content (Figure 3).
Initial Investigations Panel A: Chest radiograph (posteroanterior (PA) view) demonstrating cardiomegaly with a cardiothoracic ratio of 0.58 (normal ≤0.55 for 20 months of age), consistent with pericardial effusion.Panel B : 12-lead ECG showing sinus tachycardia (~150 bpm) with low QRS voltage in the limb leads, consistent with pericardial effusion.
Echocardiography on admission Representative echocardiographic views demonstrating a large circumferential pericardial effusion (2.5 cm) with echogenic densities and tamponade physiology.Panel A: Parasternal short-axis.Panel B: Parasternal long-axis views, apical four-chamber view and M-mode.Panel C : Plethoric (dilated) IVC with reduced inspiratory collapse (<50%), indicating elevated right atrial pressure.
Chest CT Angiography Panels A and B : Coronal and axial CT views showing large circumferential pericardial effusion without vascular or structural abnormalities.Region of interest (ROI)-based attenuation measurements of pericardial effusion in all views revealed values between 39 and 62 HU, which confirm hemorrhagic fluid.One ROI (179 HU) was excluded as artifact.
The child was admitted to the pediatric intensive care unit (PICU) and managed with supplemental oxygen, intravenous fluids, nonsteroidal anti-inflammatory drugs (NSAIDs), and empirical antibiotics. He subsequently underwent urgent pericardiocentesis, which drained approximately 200 mL of hemorrhagic fluid. Cytological and microbiological analyses of the fluid were negative for bacterial, viral, mycobacterial, and malignant causes. No recurrence of effusion was noted during hospitalization.
The patient achieved complete clinical recovery and was discharged after 14 days. At six-week follow-up, he remained asymptomatic, and repeat echocardiography demonstrated complete resolution of the pericardial effusion with normal cardiac function (Figure 4). He continues to be followed by pediatric cardiology, with a plan for reassessment and repeat echocardiography at six months post-discharge.
Post-Pericardiocentesis and Follow-Up EchocardiographyPanels A, B: Post-pericardiocentesis parasternal long-axis and apical four-chamber views showing resolution of effusion.Panels C, D: Six-week follow-up parasternal long-axis and short-axis views demonstrating absence of residual effusion.
Discussion
Hemopericardium in children is exceptionally rare and is most commonly associated with trauma, cardiac surgery, anticoagulant therapy, or malignancy [1,2]. Viral etiologies of hemorrhagic pericardial effusion are uncommon but have been reported with pathogens such as coxsackievirus, influenza virus, Epstein-Barr virus, and bacterial gastroenteritis, including Salmonella and Campylobacter species [4-11]. These cases demonstrate that infections, even outside the cardiovascular system, can occasionally lead to life-threatening cardiac complications.
Norovirus is one of the most common causes of pediatric gastroenteritis worldwide, typically resulting in self-limited gastrointestinal illness [3]. Extraintestinal manifestations are extremely rare. While myocarditis, pericarditis, and cardiogenic shock have been described in pediatric patients following viral gastroenteritis [6], hemopericardium associated with norovirus has not previously been reported. To our knowledge, this is the first documented case of pediatric hemopericardium following norovirus infection, expanding the clinical spectrum of this common viral pathogen.
The pathophysiology of viral-associated hemopericardium remains incompletely understood. Two mechanisms are most plausible: (1) direct viral invasion of the myocardium or pericardium causing local vascular injury and hemorrhagic effusion, and (2) a post-infectious immune-mediated process, consistent with the delayed presentation observed in our patient [7-9]. The markedly elevated D-dimer (11,520 ng/mL) in the absence of systemic coagulopathy suggests localized pericardial endothelial injury with active fibrinolysis. Similar patterns of elevated D-dimer without systemic clotting abnormalities have been reported in viral pericarditis, reflecting localized vascular damage rather than generalized coagulopathy. This finding supports a mechanism of hemorrhagic effusion driven by local inflammation or immune-mediated endothelial injury. Similar immune-mediated mechanisms have been described in bacterial gastroenteritis complicated by myocarditis or pericarditis [5,11-13].
While norovirus was detected in stool two weeks prior, viral RNA was not identified in pericardial fluid or blood, limiting definitive attribution. Rigorous exclusion of alternative causes - including trauma, cardiac surgery, anticoagulant therapy, malignancy, and other viral or bacterial infections - supports a possible association rather than a confirmed causality. The temporal sequence of gastroenteritis followed by hemopericardium, combined with consistency with known viral pericarditis mechanisms, strengthens the inference, though it remains at a “possible” level. Future investigations, such as pericardial fluid PCR or metagenomic sequencing, or paired serology, could provide stronger evidence for causal linkage.
Although other viral infections, such as COVID-19, have occasionally been associated with pediatric pericardial effusions, the mechanisms of viral-induced hemopericardium may be similar across different pathogens. Clinically, pediatric hemopericardium often presents with nonspecific symptoms, including fatigue, respiratory distress, pallor, and tachycardia, which can mimic myocarditis, purulent pericarditis, or malignancy. This underscores the importance of echocardiography as the primary diagnostic tool to evaluate effusion size, cardiac tamponade, and ventricular function [1,2]. In our patient, rapid echocardiographic diagnosis enabled timely pericardiocentesis and complete recovery [4].
Management requires individualized assessment based on hemodynamic stability, with urgent pericardiocentesis indicated in tamponade, along with supportive care and monitoring of inflammatory markers [1,2]. Our case highlights that viral-associated effusions may resolve completely with prompt intervention [12,14-16].
Long-term cardiology follow-up is important, as delayed complications may occur even when the acute course resolves favorably. Further research is needed to clarify the mechanisms by which norovirus may cause cardiac involvement and to guide optimal follow-up strategies in affected children.
Conclusions
Although norovirus is typically a self-limited gastrointestinal pathogen in children, this case demonstrates a rare hemopericardium possibly associated with norovirus infection. Pediatricians and emergency physicians should maintain a high index of suspicion for cardiac involvement in children presenting with unexplained cardiopulmonary signs following viral gastroenteritis.
Early recognition with echocardiography and timely pericardiocentesis are critical for diagnosis and survival. Awareness of such rare complications allows for rapid intervention, preventing life-threatening outcomes. To our knowledge, this is the first reported case of hemopericardium associated with norovirus. Additional case reports and studies are needed to better understand the underlying pathophysiology, long-term outcomes, and optimal follow-up strategies for viral-associated hemopericardium.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Management of pericardial effusion Eur Heart J Imazio M Adler Y 118611973420132312527810.1093/eurheartj/ehs 372 · doi ↗ · pubmed ↗
- 2Echocardiographic evaluation of pericardial effusion and cardiac tamponade Front Pediatr Pérez-Casares A Cesar S Brunet-Garcia L Sanchez-de-Toledo J 79520172848468910.3389/fped.2017.00079 PMC 5401877 · doi ↗ · pubmed ↗
- 3Noroviruses: a comprehensive review J Clin Virol Patel MM Hall AJ VinjéJ Parashar UD 184420091908447210.1016/j.jcv.2008.10.009 · doi ↗ · pubmed ↗
- 4Coxsackie B viral infection presenting with hemorrhagic pericardial effusion and pleural effusion Ann Pediatr Cardiol Maram KP Kudumula V Paturi VR 87891520223584740510.4103/apc.apc_21_21PMC 9280111 · doi ↗ · pubmed ↗
- 5Acute myocarditis associated with non-typhoidal Salmonella gastroenteritis Pediatr Emerg Med J Choi SH Son JS Moon HW Kim SJ Park HW Lee R 929662019
- 6Rhinovirus infection presenting with acute myocarditis with complete heart block in a child: a case report Cardiol Young Yuwattana R Singhasee K Saengsin K 248424863420243962799910.1017/S 1047951124036059 · doi ↗ · pubmed ↗
- 7Myocarditis and pericarditis in young patients following Campylobacter jejuni enterocolitis infection: a systematic review of case studies J Med Case Rep Sanicola K Shadani N Nemec EC 2nd Rose SJ 5661820243957889910.1186/s 13256-024-04921-5PMC 11585146 · doi ↗ · pubmed ↗
- 8Myocarditis in a pediatric patient with Campylobacter enteritis: a case report and literature review Trop Med Infect Dis Chantzaras AP Karageorgos S Panagiotou P 212620213494166810.3390/tropicalmed 6040212 PMC 8707348 · doi ↗ · pubmed ↗